1. Antracoza - Prez Caz

of 5
-
Upload
alina-boiangiu -
Category
Documents
-
view
18 -
download
0
Transcript of 1. Antracoza - Prez Caz
-
Black lungs and tuberculosisCase report
A never-smoking 82-year-old woman with apast medical history of type-2 diabetespresented to the outpatient clinic with a 34 months history of purulent bronchitis,haemoptysis, weight loss and fevers.
She had lived in a small village in Indiaand Pakistan all her life and had been visitingthe UK intermittently until setting up perma-nent residency a few months ago.
She denied any history of tuberculosis orany previous recent contacts.
Clinically, she had no lymphadenopathyand had bilateral crackles in the upper zoneson auscultation. Her oxygen saturations were98% on air.
HERMES syllabus links:B.4.1, D.2.11, D.2.22,D.3.1
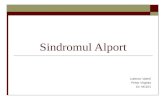
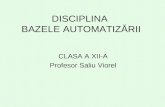
Figure 1Chest radiograph
Task 1
Interpret the chest radiograph(fig. 1)
Breathe | March 2012 | Volume 8 | No 3 247DOI: 10.1183/20734735.018311
A. Aujayeb1,
S. Worthy1,
C. Stenton1
Royal Victoria Infirmary,Newcastle Upon TyneHospitals, Newcastle uponTyne, UK
Royal Victoria Infirmary,Newcastle Upon TyneHospitals, Queen VictoriaRoad, Newcastle upon Tyne,NE1 4LP, UK
-
A diagnosis of tuberculosis was entertainedand sputum sent for analysis. A helical CTscan was also performed.
Answer 1. The chest radiograph showsgeneralised nodularity with left upper lobecollapse and right middle lobe collapse.Crowding of the left upper ribs suggestslong-standing volume loss.
a)
b)
c)
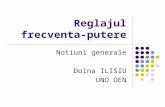
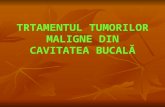
Figure 2Computerised tomography images
Task 2
Please interpret her CT scans(fig. 2)
Black lungs and TB
Breathe | March 2012 | Volume 8 | No 3248
-
Her sputum cultures yielded no positiveresults and hence she underwent fibre optic
bronchoscopy with the view of obtaininglavages for culture and microscopy.
a) b)
c) d)
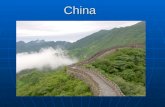
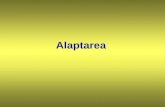
Figure 3Bronchoscopy images
Answer 2. There is right middle lobe collapse with fluid-filled distal bronchi and patent originof bronchus. There is marked volume loss and scarring in left upper lobe with fluid-filledbronchi and distorted left upper lobe bronchus, but also a larger low attenuation area on theleft peri-hilar region. There are also numerous mainly peri-bronchovascular nodules in bothlungs. There is also reduced lung attenuation in left lower lobe
Task 3
Interpret the bronchoscopic images(fig. 3)
Black lungs and TB
Breathe | March 2012 | Volume 8 | No 3 249
-
She was started on anti-tuberculous che-motherapy consisting of pyrazinamide,ethambutol, rifampicin and isoniazid giventhe high index of suspicion. She had areaction to the medications which includedvomiting and a transient bilirubin rise, whichrecurred when single agents were slowly re-introduced. No acid fast bacilli (AFB) wereseen on direct microscopy of the bronchiallavage and cultures were negative.
On repeated follow-up visits, she felt verywell with no reported symptoms or ongoingweight loss. Even if she had active tubercu-losis, she was non-infective. After a discus-sion with the patient, her family and all healthpractitioners about the riskbenefits of treat-ment versus non-treatment and careful follow-up, a decision was reached to not start anyfurther treatment.
A more detailed history revealed that shehad been a housewife all her life in a ruralregion of India and Pakistan and had had noexposure to coal. However, she has cookedon an open wood fire all her life prior tocoming to the UK.
With the CT and bronchoscopic appear-ances, we conclude that the diagnosis was ofbronchial anthracofibrosis (BAF), post-tuber-culous scarring and possible superimposedactive tuberculosis.
DiscussionBronchial anthracofibrosis (BAF) is a termthat encompasses bronchial wall narrowingand anthracotic pigmentation visible on thebronchial walls. The term was first used in acase series from Korea [1] where the pre-dominance seemed to be in never-smokingelderly female subjects with prolonged sus-tained exposure to wood smoke. The narrow-ing and pigmentation was mostly seen in theright middle lobe. 17 of the 28 patients in thatcase series also had active pulmonary tuber-culosis. However, endobronchial pigmenta-tion with airway narrowing was first describedin 1951 by ABRAHAM [2] in patients withperforated tuberculous lymph nodes.
In adults who are exposed to carbonmaterials, mild lung deposition is commonand benign. In susceptible individuals withoverexposure in various occupations, such ascoal mining, may result in significant par-enchymal disease such as coal workerspneumoconiosis [3]. BAF has been postulatedto be caused by endobronchial tuberculosis[4]. Endobronchial TB or tuberculous lympha-denopathy are more common in youngwomen, hence perforation of a lymph nodecan occur very slowly with no clinicalsymptoms and the healing process wouldmanifest as fibrosis and be discovered later inlife. However, it has been observed that BAFis not synonymous with active or oldtuberculosis. A series of 102 patients fromIran [5] confirmed BAF in full-time housewivesliving in rural regions and using biomass asfuel but none of them had tuberculosis. Aseries of patients from the UK had occupa-tional exposure to coal dust and only one hadpast history of tuberculosis [6]. Alternatively,BAF has been thought to be an endobronchial
Key learning points
N Anthracosis can occur without coal exposure and is more common in elderly women who have been exposed tobiomass fuel pollution.
N Anthracofibrosis is a clinical entity where there is anthracosis and bronchial wall stenosis. This predominantly affectsthe right middle lobe.
N There is an association of anthracofibrosis with tuberculosis.N Typical CT appearances are distal atelectasis and lymphadenopathy and the main differential diagnosis is of
malignancy.N Bacteriological evidence of TB should be ascertained before starting anti-tuberculous chemotherapy.
Answer 3. There are areas of blackpigmentation, which is known asanthracosis along with bronchial wallnarrowing. Histology would classicallyshow soot-laden macrophages.
Black lungs and TB
Breathe | March 2012 | Volume 8 | No 3250
-
form of pneumoconiosis and a variant ofprogressive massive fibrosis and the termhut lung was coined to describe a form ofpneumoconiosis in rural African women [7].
In a survey of 260,000 Indian adults [8]and in a casecontrol study [9], tuberculosiswas more common in people exposed tobiomass fuel pollution. Chronic smoke expo-sure might impair the mucociliary defences ofthe respiratory system and reduce macro-phage activity, increasing susceptibility toeven mycobacterial infections [10]. On theother hand, HWANG et al. [11] found thatcarbonaceous particles, silica and silicatespredominated in tissue specimens of patientswith BAF, which might explain the predis-position to tuberculosis.
Radiological features of BAF have beendescribed. In a case series from Korea [12],94% of patients had atelectasis distal to thesmoothly narrowed bronchus. 94% of patientsalso had mediastinal or hilar lymphadenopathyand 57% of those were calcified. The main
differential diagnosis is of malignancy andcareful evaluation of the patients should beundertaken. Parenchymal abnormalities caninclude consolidation, low attenuation nodulesand interstitial infiltrations. Various reasons havebeen postulated for the predisposition of BAF forthe right middle lobe; namely its location inrelation to the bronchus intermedius or anato-mical and ineffective collateral ventilation [13].
It had been postulated that anti-tubercu-lous chemotherapy should always be given tosomeone with BAF but current evidencedemands positivity of cultures first [14]. Westarted the quadruple regimen as the patienthad reported systemic symptoms. On follow-up, she had remained stable clinically andradiologically. With non-tuberculous BAF,steroids achieved clinical improvement butwith post tuberculous BAF, there is noconsensus on treatment [15].
Our patient has remained well on followup with no change in her radiologicalappearance and clinical state.
References
1. Chung MP, Lee KS, Han J, et al. Bronchial stenosisdue to anthracofibrosis. Chest 1998; 113: 344350.
2. Abraham GC. Atelectasis of the right middle loberesulting from perforation of tuberculous lymphnodes into bronchi in adults. Ann Intern Med 1951; 35:820835.
3. Alois D. Pneumoconioses: Encyclopedia of occupa-tional health and safety, Geneva: InternationalLabour Organization, 1998; p. 10.32..
4. Kim JY, Park JS, Kang MJ, et al. Endobronchialanthracofibrosis is causally associated with tubercu-losis. Korean J Intern Med 1996; 51: 351357.
5. Amoli K. Bronchopulmonary disease in Iranianhousewives chronically exposed to indoor smoke. EurRespir J 1998; 11: 659663.
6. Wynn GJ, Turkington PM, ODriscoll BR.Anthracofibrosis, Bronchial Stenosis With OverlyingAnthracotic Mucosa: Possibly a New OccupationalLung Disorder* A Series of Seven Cases From OneUK Hospital. Chest 2008; 134: 10691073.
7. Grobbelaar JP, Bateman ED. Hut lung: a domesticallyacquired pneumoconiosis of mixed aetiology in ruralwomen. Thorax. 1991; 46: 334340.
8. Mishra VK, Retherford RD, Smith KR. Biomasscooking fuels and prevalence of tuberculosis in India.Int J Infect Dis 1999; 3: 119129.
9. Perez-Padilla R, Perez-Guzman C, Baez-Saldana R,et al. Cooking with biomass stoves and tuberculosis:a casecontrol study. Int J Tuberc Lung Dis 2001; 5:441447.
10. Smith KR, Samet JM, Romieu I, et al. Indoor airpollution in developing countries and acute lowerrespiratory infections in children. Thorax 2000; 55:518532.
11. Hwang J, Puttagunta L, Green F et al. Bronchialanthracofibrosis and tuberculosis in immigrants toCanada from the Indian subcontinent. Int J TubercLung Dis 2010; 14: 231237.
12. Kim HY, Im JG, Goo JM, et al. Bronchial anthracofi-brosis inflammatory bronchial stenosis with anthra-cotic pigmentation: CT findings. Am J Roentgenol2000; 174: 523527.
13. Brock RC. Post-tuberculous broncho-stenosis andbronchiectasis of the middle lobe. Thorax 1950; 5: 539.
14. Han SH, Cha GY, Lee YM, et al. Study ofantituberculous medications in antracofibrosis.Tuberc Respir Dis 2001; 51: 224231.
15. Jang SJ, Lee SY, Kim SC, et al. Clinical andradiological characteristics of non-tuberculous bron-chial anthracofibrosis. Tuberc Respir Dis 2007; 63:139144.
Black lungs and TB
Breathe | March 2012 | Volume 8 | No 3 251