Revista Univeritaria 12
64
CUPRINS Adriana Aura Spînu Kinetoterapia în geriatrie............................................................1 Geriatric kinesiotherapy.............................................................3 Adriana Neofit Mircea Ion Ene Optimizarea planificării educării şi dezvoltării psihomotricităţii sportivilor judoka de 10 - 11 ani.................................................6 Planing optimization of education and development of psychomotricity for judoka 10-11 years sportsmen…………..11 Eugen Baştiurea Corelaţia dintre capacitatea de reglare a parametrilor dinamici şi pregătirea fizică a jucătorilor de handbal..................................16 The correlation between the capacity of regulating the dynamic parameter and the physical training of the handball players ....20 Hariton A. Haritonidis, Vasiliki K. Tyrovola Dans si identitate de gen tsift (e)-teli dance în farassa, kappadokia...............................................................................23 Dance and gender identity the tsift(e)-teli dance in farassa, kappadokia………………………………...............................28 Mircea Ion Ene Judo, comunicare şi lucru în echipă……………………….....33 Judo, communication and team working.................................36 Oana Sîrbu Studiu comparativ privind creşterea şi dezvoltarea fizică a copiilor de vârstă şcolară atât din mediul urban cât şi din mediul rural în corelaţie cu factorii de mediu şi socio- economici……………………………………………………..38 Comparative reaserch on growth and phisical development of the school age children both in urban and in rural areas and the correlation between environmental factors and social factors economic……………………………………………………..42 Rodica Marinescu Aspecte imagistice ale complicaţiilor rahidiene postoperatorii ..................................................................................................45 Imaging aspects of postoperative spinal complications…………………………………………………49 Viorica Lefter Oana Andreea Cibu Abordare kinetică şi nutriţională a obezităţii. (studiu)...........52 Kinetic and nutritional approach of the obesity. (study)……...57 Prezentarea cadrelor. F.E.F.S Galaţi: BAŞTIUREA EUGEN ................................6
description
Revista FEFS
Transcript of Revista Univeritaria 12

CUPRINS
Adriana Aura Spînu
Kinetoterapia în geriatrie............................................................1 Geriatric kinesiotherapy.............................................................3
Adriana Neofit Mircea Ion Ene
Optimizarea planificării educării ş i dezvoltării psihomotricităţii sportivilor judoka de 10 - 11 ani.................................................6 Planing optimization of education and development of psychomotricity for judoka 10-11 years sportsmen…………..11
Eugen Baştiurea
Corelaţia dintre capacitatea de reglare a parametrilor dinamici şi pregătirea fizică a jucătorilor de handbal..................................16 The correlation between the capacity of regulating the dynamic parameter and the physical training of the handball players ....20
Hariton A. Haritonidis, Vasiliki K. Tyrovola
Dans si identitate de gen tsift (e)-teli dance în farassa, kappadokia...............................................................................23 Dance and gender identity the tsift(e)-teli dance in farassa, kappadokia………………………………...............................28
Mircea Ion Ene
Judo, comunicare şi lucru în echipă……………………….....33 Judo, communication and team working.................................36
Oana Sîrbu
Studiu comparativ privind creşterea şi dezvoltarea fizică a copiilor de vârstă şcolară atât din mediul urban cât şi din mediul rural în corelaţie cu factorii de mediu şi socio-economici……………………………………………………..38 Comparative reaserch on growth and phisical development of the school age children both in urban and in rural areas and the correlation between environmental factors and social factors economic……………………………………………………..42
Rodica Marinescu
Aspecte imagistice ale complicaţiilor rahidiene postoperatorii ..................................................................................................45 Imaging aspects of postoperative spinal complications…………………………………………………49
Viorica Lefter Oana Andreea Cibu
Abordare kinetică şi nutriţională a obezităţii. (studiu)...........52 Kinetic and nutritional approach of the obesity. (study)……...57
Prezentarea cadrelor. F.E.F.S Galaţi: BAŞTIUREA EUGEN ................................61


1
KINETOTERAPIA ÎN GERIATRIE
Kinetoterapeut: AURA-ADRIANA SPÎNU
[email protected] Cuvinte cheie: geriatrie, kinetoterapie. Rezumat:
Articolul prezintă afecţiunile pacientului vârstnic şi rolul pe care îl are kinetoterapia în recuperarea acestuia. Traumatismele, procesele inflamatorii şi degenerative, deficienţele de postură, afecţiunile neurologice, cardio-vasculare, respiratorii, problemele de greutate reprezintă câteva din problemele importante ale pacientului vârstnic la care kinetoterapia are soluţii atât pe termen scurt cât şi pe termen lung.
Kinetoterapia geriatrică poate fi considerată o disciplină particulară în cadrul kinetoterapiei şi acest fapt se datorează modalităţilor de aplicare şi adaptare prin care se urmăreşte redobândirea unor funcţii afectate de boală, de sechelele unei boli şi reintegrarea pacientului vârstnic în societate.
În cadrul procesului fiziologic de îmbătrânire se constată o scădere a capacităţii de adaptare la nivelul funcţiilor diferitelor aparate şi sisteme, astfel vârstnicul fiind predispus la afecţiuni cardiovasculare, traumatice, respiratorii, psiho-afective, neurologice, reumatologice, oftalmologice, afecţiuni ORL, probleme de greutate dar şi deficienţe de postură.
Kinetoterapia poate să intervină profilactic - atunci când se cunosc particularităţile genetice şi metabolice în vederea întârzierii apariţie unor afecţiuni, pentru a tonifia musculatura, a menţine amplitudinea articulară şi a evita producerea traumatismelor la nivelul diferiletor articulaţii sau la articulaţiile cele mai solicitate şi terapeutic - atunci când apar traumatismele, procesele inflamatorii şi degenerative, deficienţele posturale şi afecţiunile neurologice.
O problemă extem de importantă (deoarece implică apariţia în timp a altor afecţiuni sau le pot accentua pe cele existente) se referă la deficienţele posturale. Conceptul de postură nu se referă doar la statică, ci el se identifică cu concepte precum echilibru raportat la mediu ambiant, stress-ul exercitat asupra corpului în diferite acţiuni ale acestuia. Factorii care determină apariţia deficienţelor posturale sunt: predispoziţii individuale (musculare, articulare, osoase, ale tendoanelor şi ligamentelor, ale viscerelor), alterări morfo-funcţionale dar şi acţiunea mediului asupra individului. Controlul posturii este considerat a fi capacitatea adaptativă a sistemului neuromotor dependentă de integrarea informaţiilor care vin de la receptori. Posturologia permite specialiştilor (oftalmologi, antropologi, ORL-işti, neurologi, psihologi, ortopezi, fizioterapeuţi şi kinetoterapeuţi) interpretări comune a deficienţelor posturale. Modificarea minimă a posturii raportată la mediu este percepută (de retină în special, de bolta plantară şi de muşchii membrului inferior) transmisă SNC(Sistem Nervos Central) care emite răspunsul corespunzător (organizarea şi stabilizarea mişcării). Dereglarea unuia sau mai multor receptori ai sistemului postural presupune trimiterea mai multor date eronate SNC. Răspunsuri multidiscipliare ţin cont de: cunoaşterea ansamblului de procese neurofiziologice şi vestibulare, elemente de statica şi dinamica mersului cu analiza pasului, amprenta plantară, disturbatori posturali, organism, o relaxare generală dar şi o reechilibrare lentă a funcţiei motorii şi neurovegetative. O altă problemă a pacientului vârstnic este tendinţa de îngrăşare care merge până la obezitate. Această problemă se datorează sedentarismului - care poate fi favorizat de îmbătrânirea fiziologică sau de cea timpurie dar şi a lipsei unor activităţi zilnice organizate

2
sau unor afecţiuni ale aparatului locomotor, afecţiuni cardiovasculare, afecţiuni respiratorii dar şi ca urmarea a unei stări depresive. Pacienţii supraponderali sau sedentari sunt predispuşi la probleme osteo-articulare, dezechilibre musculare şi toleranţă scăzută la efort, HTA, insuficienţă cardiacă, insuficienţă respiratorie, diabet, litiază biliară, afecţiuni psiho-afective, boli reumatologice…şi astfel se creează un cerc vicios. Traumatismele, bolile reumatismale şi cele neurologice sunt cele mai frecvente afecţiuni întâlnite la pacientul vârstnic. Imobilizarea prelungită datorată unui traumatism (inclusiv cranio-cerebrale), durerii accentuate, hemiplegii, tumori cerebrale, boala Parkinson, scleroză multiplă(SM) are efecte negative asupra circulaţiei de întoarcere, astfel prin stază venoasă apare edemul interstiţial, imobilizarea articulaţiilor determină apariţia unui proces inflamator sinovial, aderarea sinovialei la cartilajul articular şi dezvoltarea redorii articulare. Imobilizarea prelungită conduce transformarea ţesutului fibro-grăsos care invadează articulaţia în ţesut fibros şi determină blocarea articulaţiei. În cazul hemiplegiei vasculare cerebrale ischemice, în perioada 6-24 luni de la debut, mai mult de un sfert dintre pacienţi dezvoltă sindrom algoneurodistrofic predominant la membrul superior. Simptomele algoneurodistrofice sunt: edem, tulburări vasomotorii şi trofice locale şi regionale, modificări ale structurii osoase din zona afectată şi durere, toate acestea conducând la impotenţă funcţională. În ceea ce priveşte modificările structurii osoase în cadrul algoneurodistrofiei răspunzătoare este osteoporoza localizată. SM este o boală cronică în care sistuaţia se înrăutăţeşte progresiv, nici o altă boală neurologică nu prezintă atât de multe zone afectate. Kinetoterapia în acest caz are un rol deosebit de important pentru calitatea vieţii. În cadrul acestei boli obiectivul principal este întreţinerea pe o perioadă cât mai lungă a independenţei funcţionale, corectarea deformaţiilor instalate, menţinerea mobilităţii, prevenirea atrofiilor, menţinerea troficităţii ţesuturilor moi şi conservarea capacităţii de deplasare. Kinetoterapia în cadrul tratamentului bolii Parkinson influenţează pozitiv starea psihică a pacientului, îi permite şi îl motivează să efectueze activităţi pe care nu le putea efectua. Exerciţiile vizează activitatea musculară şi articulară. Întreţinerea respiratorie este un aspect foarte important, iar programul va fi individualizat şi corespunzător etapei în care se află pacientul.
În cadrul procesului de recuperare a bolnavului vârstnic, obiectivul principal al kinetoterapiei este prevenirea apariţiei complicaţiilor urmat de: obţinerea transferurilor, mobilizare, obţinerea unei amplitudinii de mişcare articulară sau conservarea acesteia (în limite funcţionale), tonifiere musculară, forţă şi rezistenţă musculară, obţinerea coordonării şi a controlului motor, precum şi recâştigarea echilibrului, reluarea mersului (numai în condiţiile în care ortostatismul este stabil) cu scopul de a obţine şi menţine cât mai mult timp autonomia bolnavului.
Obiectivele generale în recuperarea pacientului vârstnic constau în consilierea acestuia cu privire la:
- acceptarea procesului de îmbătrânire şi să distingă aspectele normale de cele patologice;
- controlarea procesului de îmbătrânire, prin intervenţie proprie sau a familiei; - soluţionarea problemelor patologice. - abordarea globală - structurarea programului pe etape - evaluare a rezultatelor pe etape - continuitatea - participarea pacientului dar şi a familiei acestuia Regulile de bază care se impun în recuperarea pacientului vârstnic sunt următoarele:

3
- cunoaşterea exactă a bolii de care suferă pacientul precum şi a stării structurilor anatomice care urmează să fie mobilizate;
- alegerea poziţiei bolnavului în obţinerea condiţiilor de relaxare maximă şi dând posibilitatea pacientului să urmărească mişcarea efectuată pasiv;
- efectuarea mobilizării pasive numai pe axele fiziologice de mişcare; - asocierea elementelor de facilitare cu mişcarea pasivă; - dacă există spasticitate, terapeutul va evita să menţină timp îndelungat mâna pe
grupele musculare spastice; - fiecare articulaţie va fi mobilizată individual; - se interzice mobilizarea unei articulaţii prin intermediul alteia; - se va evita provocarea durerii prin mobilizare, cand amplitudinea articulară este foarte
redusă; - forţa, viteza, durata, frecvenţa vor fi permanent adecvate etapei în care se află
pacientul şi obiectivului vizat Mijloacele de intervenţie vor fi adaptate în permanenţă necesităţilor pacientului vârstnic Comunicarea dintre kinetoterapeut şi pacient este un aspect deosebit de important, astfel
că se va explica pacientului în ce constă programul, care sunt beneficiile acestuia iar comenzile verbale vor fi rostite clar şi tare.
Fiecare bolnav vârstnic având necesităţi diferite de deplasare, în funcţie de perioada zilei, temperatură, oboseală, distanţă, se va recomanda utilizarea dispozitivelor ortetice speciale (cârjă, baston, cadru, orteze), în vederea obţinerii unui consum energetic minim.
Kinetoterapia în geriatrie reuşeşte să dea pacientului autonomie, dar aceasta întotdeauna va depinde de tipul bolii, timpul trecut de la instalarea acesteia şi până la debutul tratamentului, sechele şi nu în ultimul rând de afecţiuni asociate.
BIBLIOGRAFIE
1. Albu, C-tin.; Vlad, T.,L.; Albu, Adriana , Kinetoterapia pasivă, Editura Polirom, Iaşi, 2004. Bucureşti, 1981. 2. Cesarani, A., La postura ed il sistema dell'equilibrio – Alti del II congresso di posturologia, Fiuggi, giugno, 1998. 3. Enoka, R., M., Neuromechanics basis of kinesiology. Human kinetics, S.U.A., 1994. 4. Kiss, I., Fiziokinetoterapia şi recuperarea medicală în afecţiunile aparatului locomotor, Editura Medicală, Bucureşti, 2002. 5.Scalia, Osteopatia e kinesiologia applicata, Ed. Marrapesse, Roma, 1999. 6. Sbenghe, T., Recuperarea medicală a sechelelor posttraumatice ale membrelor, Editura Medicală, Bucureşti, 1981.
GERIATRIC KINESIOTHERAPY
Kinetoterapeut: AURA-ADRIANA SPÎNU [email protected]
Key words: geriatrics, kinesiotherapy. Abstract:
The article depicts certain pathologies of elderly patients, as well as the part played by kinesiotherapy in their recovery. The traumas, degenerative and inflammatory processes, posture deficiencies, neurologic, cardio-vascular, respiratory pathologies and the

4
weight problems are only a few of the major issues the elderly patients are confronted with, issues for which kinesiotherapy offers both long-term and short-term solutions.
Geriatric kinesiotherapy may be regarded as a specific kinesiotherapy field, this being
due to the manners of adaptation and application of certain procedures aiming at recovering various disease or sequelae-affected functions, and restoring the elderly patients to their normal health state.
During the physiologic aging process, a certain decrease in the adapting capacity of various systems’ functions can be noted, consequently the elderly patients being increasingly exposed to cardio-vascular, traumatic, respiratory, psycho-affective, neurologic, rheumatic, ophthalmic and hearing conditions, weight problems, and also posture deficiencies.
The kinesiotherapy approach may be prophylactic – when the genetic and metabolic distinctive features are known, in order to delay the occurrence of certain diseases, to invigorate the muscular system, maintain the amplitude of the joints, especially the intensively-used ones, and therapeutic – when traumas, degenerative inflammatory processes, posture deficiencies and neurologic pathologies occur.
A problem of the utmost importance (as, in time, it involves the occurrence of certain pathologies that may accentuate other pre-existent ones) concerns the posture deficiencies. The posture concept is not to be regarded solely from the static point of view, as it also involved concepts such as the equilibrium with regard to the surrounding environment and the pressure applied to the body in various actions and movements. The factors determining the occurrence of posture deficiencies are: individual predispositions (muscular, joint, bone, tendon, ligament and organ-related), morpho-functional deteriorations, but also the influence the environment has on every individual.
Posture control is considered to be the adaptive capacity of the neuromotor system that relies on integrating the information transmitted by the receptors. Posturology allows specialists (ophthalmologists, anthropologists, neurologists, psychologists, orthopedists, physiotherapists and kinesiotherapists) to make similar interpretations of posture deficiencies.
The minimum modification of the posture with regard to the environment is generally perceived by the retina, the arches of the foot and the muscles of the inferior limb, and then it is transmitted to the Central Nervous System which provides the adequate feedback (the organization and stabilization of the muscles). The improper functioning of one or several receptors of the posture system means that the CNS will be provided with biased information.
The pluridisciplinary answers rely on: knowing the neuro-physiologic and vestibular process array, walking static and dynamics elements, the foot print, postural disturbers, the body as a whole, general relaxation and also a slow recovery of the motor and neurovegetative function.
Another problem of the elderly patient is represented by the predisposition to gaining weigh, which may lead to obesity. This is a direct consequence of the lack of physical activity – which may be induced by the physiologic aging process or by the early aging process, but also by the lack of a daily organized activity or various conditions of the locomotory system, cardiovascular diseases, respiratory diseases and the aftermath of a depressive state. Overweight or sedentary patients are subject to develop problems of the bones and joints, muscular imbalances and little effort tolerance, HTN, heart failure, respiratory failure, diabetes, biliary lithiasis, psycho-affective disorders, rheumatic disorders, thus creating a spiral of negative factors and effects.
Traumas, rheumatic and neurologic disorders are among the most common disorders elderly patients may be confronted with. Trauma induced long-term immobilization (inclusively cranio-cerebral traumas), or the one caused by severe pain, hemiplegia, brain

5
tumors, Parkinson disorder, multiple sclerosis (MS) with its multiple effects on blood circulation, thus creating the interstitial edema through venous stasis and the immobilization of the joints, all lead to a synovial inflammatory process, the adhesion of the synovial to the cartilage in the joints and resulting in joint stiffness.
Long-term immobilization leads to the transformation of the fibro-fatty tissue, that invades the joint in fibrous tissue eventually blocks the joint.
Concerning the vascular ishcaemic hemiplegia, in the first 6-24 months, more than a quarter of the patients develop algoneurodistrophy, especially in the superior limb. The algoneurodistrophic symptoms are: edema, regional and trophic and venous disorders, modifications of the bone structure in the affected area and pain, all leading to functional impotence. Regarding the modifications of the bone structure while suffering from algoneurodistrophy, the main factor determining it is the localized osteoporosis.
MS is a chronic disease that worsens progressively, no other neurologic disorder being known to affect this many areas of the body. In this case, kinesiotherapy plays an extremely important part in improving the quality of life. The main goal is maintaining the functional autonomy as long as possible, correcting any eventual deformity, maintaining the mobility, preventing atrophies, maintaining the trophicity of soft tissues and preserving the ability to move.
The adequate kinestiotherapy practice for the Parkinson disorder positively influences the patient’s mental state, motivating him or her to carry on several activities that may have been restricted by the disease. The activities are focused on the activity of the muscles and joints. Maintaining the he respiratory function is another very important aspect, the program being created so that it corresponds to the phase of the disorder the patient is found in.
Concerning the part played by kinesiotherapy in the recovery of elderly patients, the main goal is represented by the prevention of complications, followed by: obtaining transfers, mobilization, obtaining the joint movement amplitude or preserving it (within functional limits), muscular invigoration, force and muscular endurance, obtaining motor coordination and control, as well as regaining the control of the equilibrium, walking again (only if the body is stable) so that the patient’s autonomy may be maintained as much as possible.
The general goals in the elderly patients’ recovery aim at their psychological preparation in:
- accepting the aging process and distinguishing between the normal and pathological aspects;
- controlling the aging process, by their own intervention, or by thir family’s intervention;
- solving pathological problems; - reaching a global approach; - structuring the program in several phases; - assessing the results of each phase; - continuity; - involving both the patient and his or her family.
Basic rules to be taken into account in the elderly patients’ recovery: - knowing exactly what is the disorder affecting the body, as well as the states of
the anatomic structures which are to be mobilized; - choosing the patient’s position in obtaining the maximal relaxation conditions and
giving them the possibility to passively observe the procedures; - proceeding to the passive mobilization only on the physiological movement axes; - associating the facilitating elements with passive movement; - should any spasms occur, the therapist will avoid a prolonged contact with the
concerned muscular groups;

6
- each joint shall be mobilized individually; - the mobilization of one joint through another is strictly forbidden; - causing pain when mobilizing a joint shall be avoided at all costs, especially
when the amplitude of the joint is considerably reduced; - the force, speed, length and frequency shall be permanently adjusted to the phase
the patient is found in and the goal to be achieved. The intervention manners shall be permanently adapted to the necessities of the elderly patients. The communication between the kinesiotherapist and the patient is an extremely
important aspect of the recovery process, therefore the former will take the necessary time to explain the parameters of the program to the latter, what are the benefits of the program, and the verbal commands shall be expressed clearly.
Given the different necessities of each elderly patient, depending on the period of the day, the temperature, fatigue and distance, the use of special orthetic devices shall be recommended (crutch, cane, walking frame), as to preserve as much energy as possible.
The geriatric-applied kinesiotherapy practice manages to increase the patient’s autonomy, yet this autonomy shall always depend on the type of the disorder the patient is suffering from, the period of time passed until the beginning of the treatment, any possible sequelae and last but not least, adjacent disorders.
OPTIMIZAREA PLANIFIC ĂRII EDUCĂRII ŞI DEZVOLT ĂRII PSIHOMOTRICIT ĂŢII SPORTIVILOR JUDOKA DE 10 - 11 ANI
Adriana Neofit CSS Galaţi Mircea Ion – Ene FEFS Galaţi
Este cunoscut faptul că pentru obţinerea performanţelor sportive în fiecare disciplină
deci şi în judo este necesară o pregătire optimă pe fiecare nivel de vârstă (etapizat) astfel încât cei mai dotaţi sportivi să îşi poată fructifica corespunzător calităţile psihomotrice, abilitaţile tehnice şi cunoştinţele teoretice.
Obiectivele cercetării. Judo face parte din categoria sporturilor individuale care se caracterizează din punct
de vedere tehnic prin dominanta aciclică a mişcărilor, prin solicitare şi efecte cumulative privind aspectele morfologice, funcţionale, motrice ale individului şi o tehnică cât mai corectă a procedeelor de luptă.
Datorită performanţelor tot mai ridicate, procesul de antrenament trebuie revizuit atât ca formă cât şi în conţinut, perfecţionarea mijloacelor şi criteriilor de pregătire dând naştere la noi performanţe. În consecinţă ne-am propus: ☯ Elaborarea planului de pregătire şi a structurilor de acţionare care ar putea contribui la optimizarea instruirii şi realizarea obiectivelor la nivelul grupelor de începători în judo; ☯ Pregătirea şi de folosirea jocurilor şi ştafetelor aplicative pentru îmbunătăţirea tehnicii în judo desprinse din literatura de specialitate; ☯ Formularea unor propuneri pentru îmbunătăţirea metodologiei de dezvoltare a calităţilor psihomotrice şi însuşirea tehnicii procedeelor de judo la grupele de copii de 10-11 ani.

7
Organizarea şi desfăşurarea studiului Intenţia noastră a fost încă de la început, de a optimiza programarea, planificarea şi
îmbogăţirea gamei sistemelor de acţionare necesare dezvoltării calităţilor psihomotrice şi însuşirii procedeelor tehnice specifice judo-ului la sportivii de 10-11 ani.
De aceea, faţă de planurile şi mijloacele propuse în literatura de specialitate, am folosit în exclusivitate un program, o planificare şi sisteme de acţionare selecţionate şi adaptate de noi la acest nivel de vârstă.
Experimentul s-a desfăşurat la Sala de Judo a Clubului Sportiv Şcolar Galaţi în perioada septembrie 2009 – iunie 2010, a cuprins un număr de 15 sportivi judoka.
Subiecţii care fac obiectul acestei cercetări fac parte din grupele cu program de judo din cadrul Clubului Sportiv Şcolar Galaţi.
Prezentam in continuare UN MACROCICLU OPTIMIZAT PENTRU educarea şi dezvoltarea componentelor psihomotricităţii la 10-11 ani

DO
ME
NIU
L: A
ntre
nam
ent s
port
iv, D
ISC
IPLI
NA
: JU
DO
DU
RA
TA
: 35
săptăm
âni (
140
antr
.) /
80-9
0 m
inut
e/an
tren
amen
t
GR
UP
A D
E V
ÂR
STĂ
: 10
-11
ani
ST
RA
TE
GIA
DID
AC
TIC
A
OB
IEC
TIV
E F
INA
LE/C
AD
RU
N
R. D
E
AN
TR
. 3M
F
.OR
G.
TIM
P D
IDA
CT
IC
IND
ICAŢ
II
ME
TO
DIC
E
Să c
onşt
ient
izez
e sc
hem
a co
rpor
ală p
ropr
ie
8 an
tr.
Met
ode:
jocu
l, ex
ersa
rea
, im
itaţia
Mijl
oace
: j
ocu
ri d
e m
işca
re,
exer
ciţii d
in a
tletis
m (
varia
nte
de
mer
s, a
lerg
are
), g
imn
ast
ică (e
xerc
iţii d
e fr
ont ş
i for
maţ
ii, d
e
dez
volta
re fi
zică
arm
onio
asă)
Mat
eria
le: b
ast
oan
e, c
ercu
ri, s
alte
le
fron
tal i
ndi
vid
ual
pe
per
ech
i gru
pe
ech
ipe
2 an
tr.
6 an
tr/1
5 m
inut
e
Tot
al: 2
70'
(4,5
h)
se
cor
ecte
ază
greş
elile
tre
cerii
prin
exe
cuţie
Să c
unoa
scă
plan
urile
de
acţiu
ne a
cor
pulu
i şi a
părţil
or lu
i 8
antr
. M
etod
e: jo
cul,
exer
sare
a,
imitaţi
a
Mijl
oace
: j
ocu
ri d
e m
işca
re,
exer
ciţii d
in a
tletis
m
(va
riant
e d
e m
ers,
ale
rga
re,
săr
ituri)
, gim
nast
ică (
exer
ciţii
de
fron
t şi f
orm
aţii,
de
dez
volta
re fi
zică
arm
onio
asă,
elem
ente
sta
tice şi d
ina
mic
e di
n ac
roba
tică)
Mat
eria
le: m
ingi
de
dife
rite
dim
ensi
uni şi g
reu
tăţi,
salte
le,
jalo
an
e
fron
tal i
ndi
vid
ual
pe
per
ech
i gru
pe
ech
ipe
2 an
tr.
6 an
tr/1
5 m
inut
e
Tot
al: 2
70'
(4,5
h)
se
u
rmăr
eşte
lucr
u
pe
per
ech
i va
loric
e
ap
ropi
ate
Să îş
i sin
cron
izez
e m
işcar
ea s
egm
ente
lor ş
i a c
orpu
lui c
a în
treg
8
antr
. M
etod
e: jo
cul,
exer
sare
a,
imitaţi
a, p
rob
lem
atiz
are
a
Mijl
oace
: joc
uri
dina
mic
e, şta
fete
, pa
rcu
rsu
ri ap
lica
tive,
exe
rci
ţii
din
atle
tism
, gim
na
stică
Mat
eria
le: j
alo
an
e, bă
nci
de
gim
na
stică,
ob
sta
cole
fron
tal i
ndi
vid
ual
pe
per
ech
i gru
pe
ech
ipe
2 an
tr.
6 an
tr/1
5 m
inut
e
Tot
al: 2
70'
(4,5
h)
se
cor
ecte
ază
greş
elile
tre
cerii
prin
exe
cuţie
Să
îş
i îs
uşe
as
că
noţiu
nile
sp
aţia
le
de
trai
ecto
rie,
dist
anţă
, măr
ime,
poz
iţie
şi fo
rmă
8 an
tr.
Met
ode:
jocu
l, ex
ersa
rea
, p
rob
lem
atiz
are
a
Mijl
oace
: joc
uri
dina
mic
e, şta
fete
, pa
rcu
rsu
ri ap
lica
tive,
exer
ciţii
de
învăţa
re a
dep
rind
erilo
r m
otric
e d
e b
az
ă
(prin
der
ea-a
runc
are
a) şi u
tilita
r a
plic
ativ
e (t
ran
spor
t de
greu
tăţi,
esca
lad
are
, căţă
rare
)
Mat
eria
le: m
ingi
de
dife
rite
dim
ensi
uni şi g
reu
tăţi,
obst
aco
le,
zid
ul
de
ant
ren
am
ent
fron
tal i
ndi
vid
ual
pe
per
ech
i gru
pe
ech
ipe
2 an
tr.
6 an
tr/1
5 m
inut
e
Tot
al: 2
70'
(4,5
h)
se
u
rmăr
eşte
lu
cru
p
e p
erec
hi v
alo
rice
ap
ropi
ate
Să î
nsuş
ească
depr
inde
rile
de o
rient
are
spaţi
ală,
tem
pora
ră ş
i de
ap
reci
ere
a tr
aiec
torii
lor,
dire
cţiil
or şi
vite
zelo
r de
dep
lasa
re a
un
or o
biec
te în
cor
elaţi
e cu
pro
priu
l cor
p
10 a
ntr
. M
etod
e: jo
cul,
exer
sare
a,
Mijl
oace
: joc
uri
dina
mic
e, şta
fete
, pa
rcu
rsu
ri ap
lica
tive,
exe
rci
ţii
cu m
inge
a
Mat
eria
le: j
alo
an
e, m
ingi
de
teni
s, h
andb
al,
basc
het
, vo
lei,
fotb
al,
obst
acol
e, z
idu
l de
ant
ren
am
ent
fron
tal i
ndi
vid
ual
pe
per
ech
i gru
pe
ech
ipe
3 an
tr.
7 an
tr/1
5 m
inut
e
Tot
al: 3
75'
(6,2
5 h)
se
cor
ecte
ază
greş
elile
tre
cerii
prin
exe
cuţie
Să
fie
capa
bil
să
real
izez
e o
sarc
ină
mot
rică
sau
mai
m
ulte
co
mbi
nate
într
-un
ritm
şi t
empo
u im
pus
12
ant
r.
Met
ode:
jocu
l, ex
ersa
rea
,
Mijl
oace
: joc
uri
dina
mic
e, şta
fete
, pa
rcu
rsu
ri ap
lica
tive,
rea
liza
rea
un
or s
arc
ini m
otric
e sa
u c
omb
ina
ţii d
e sa
rcin
i mot
rice
într
-un
ritm
şi
tem
pou
imp
us
fron
tal i
ndi
vid
ual
pe
per
ech
i gru
pe
ech
ipe
20
ant
r. 1
5 m
inu
te/
60
ant
r.
Tot
al:2
30
0'
(38
h)
se
u
rmăr
eşte
doz
are
a c
orec
tă
a m
ijloa
celo
r se
core
ctea
ză gr
eşel
ile

Mat
eria
le: j
alo
an
e, m
ingi
de
teni
s, h
andb
al,
basc
het
, vo
lei,
fotb
al,
obst
acol
e, bă
nci
de
gim
nast
ică
trec
erii
p
rin
exec
uţie
Să-ş
i re
aliz
eze
prin
co
ntro
l vo
lunt
ar
menţin
erea
po
ziţiil
or
de
echi
libru
sta
tic ş
i din
amic
10
ant
r.
Met
ode:
jocu
l, ex
ersa
rea
, p
rob
lem
atiz
are
a
Mijl
oace
: joc
uri
dina
mic
e, şta
fete
, pa
rcu
rsu
ri ap
lica
tive,
exer
ciţii
de
mer
s, a
lerg
are
şi
săr
ituri
cu m
enţin
erea
ech
ilib
rulu
i pe
sup
rafeţe
va
riate
Mat
ebria
le:
obst
aco
le,
bănc
i d
e g
imn
ast
ică, p
lanu
ri
încl
ina
te, p
lăci m
obile
, tr
am
bulin
a e
last
ică
fron
tal i
ndi
vid
ual
pe
per
ech
i gru
pe
ech
ipe
3 an
tr.
7 an
tr/1
5 m
inut
e
Tot
al: 3
75'
(6,2
5 h)
se c
orec
tea
ză
greş
elile
tre
cerii
prin
exe
cuţie
Să f
ie c
apab
il să
rea
lizez
e acţiu
ni s
i st
ruct
uri
mot
rice
în a
mbe
le
plan
uri
ale
late
ralităţ
ii ut
ilizâ
nd s
egm
ente
ale
cor
pulu
i at
ât d
in
part
ea d
reap
tă, c
ât şi
din
cea
stâ
ngă
10
ant
r.
Met
ode:
jocu
l, ex
ersa
rea
, p
rob
lem
atiz
are
a
Mijl
oace
: joc
uri
dina
mic
e, şta
fete
, pa
rcu
rsu
ri ap
lica
tive,
exer
ciţii
de
prin
der
e-a
run
care
a u
nor
ob
iect
e, c
ond
ucer
e
a m
ingi
i, a
tât c
u b
raţul (
pici
oru
l) în
dem
âna
tic, c
ât
şi c
u
cel n
eînd
emâ
natic
, tra
nsp
ort d
e gr
eut
ăţi
Mat
eria
le: o
bie
cte,
băn
ci d
e gi
mn
ast
ică
fron
tal i
ndi
vid
ual
pe
per
ech
i gru
pe
ech
ipe
3 an
tr.
7 an
tr/1
5 m
inut
e
Tot
al: 3
75'
(6,2
5 h)
se
u
rmăr
eşte
doz
are
a c
orec
tă
a m
ijloa
celo
r
Să p
erce
apă şi
să
reacţio
neze
cât
mai
rap
id ş
i ef
icie
nt l
a st
imul
i vi
zual
i şi a
uditi
vi
12
ant
r.
Met
ode:
jocu
l, ex
ersa
rea
, p
rob
lem
atiz
are
a
Mijl
oace
: joc
uri
dina
mic
e, şta
fete
, pa
rcu
rsu
ri ap
lica
tive,
ale
rgări c
u
sta
rtu
ri di
n di
ferit
e p
oziţii, l
a s
emna
le v
izu
ale
şi a
udi
tive
varia
te
Mat
eria
le: o
bie
cte
de
culo
ri şi fo
rme
dife
rite,
obs
taco
le
fron
tal i
ndi
vid
ual
pe
per
ech
i gru
pe
ech
ipe
4 an
tr.
8 an
tr/1
5 m
inut
e
Tot
al: 4
80'
(8 h
)
se
u
rmăr
eşte
doz
are
a c
orec
tă
a m
ijloa
celo
r
să p
erce
apă şi
să
reacţio
neze
cât
mai
rap
id ş
i ef
icie
nt l
a st
imul
i ca
re fa
c pos
ibilă
per
cepe
rea
prop
riilo
r m
işcă
ri (s
ilu
lui
chin
este
zic)
12
ant
r.
Met
ode:
jocu
l, ex
ersa
rea
, p
rob
lem
atiz
are
a,
imita
rea
Mijl
oace
:
jocu
ri d
e m
işca
re,
şta
fete
, p
arc
urs
uri
ap
licat
ive,
exer
ciţii
în c
ond
iţii v
aria
te şi
cu
îngr
euie
re
Mat
eria
le: o
bie
cte,
băn
ci d
e gi
mn
ast
ică,
fron
tal i
ndi
vid
ual
pe
per
ech
i gru
pe
ech
ipe
4 an
tr.
8 an
tr/1
5 m
inut
e
Tot
al: 4
80'
(8 h
)
se c
orec
tea
za
greş
elile
tre
cerii
p
rin e
xecuţie
Să
fieca
pabi
l să
-şi
regl
eze
perc
epţia
gr
adul
ui
de
tens
iune
m
uscu
lară
(to
nus
mus
cula
r)
10
ant
r.
Met
ode:
jocu
l, ex
ersa
rea
, p
rob
lem
atiz
are
a,
imita
rea
Mijl
oace
:
jocu
ri d
e m
işca
re,
şta
fete
, p
arc
urs
uri
ap
licat
ive,
exer
ciţii
de
lovi
re a
un
or m
ingi
de
greu
tăţ
i şi m
ărim
i dife
rite
cu
pic
ioru
l la
dis
tanţe
dife
rite ş
i ţin
te fi
xe şi
mob
ile,
exer
ciţii
de
aru
nca
re a
un
or m
ingi
şi
ob
iect
e d
e gr
eutăţi ş
i măr
imi d
iferit
e la
dis
tanţ
e d
iferit
e şi p
unct
e fix
e sa
u m
obile
Mat
eria
le: o
bie
cte,
băn
ci d
e gi
mn
ast
ică, ţi
nte
fixe şi
mob
ile,
min
gi
de
fotb
al,
hand
ba
l, vo
lei,
teni
s, o
ină, b
asc
het
, ru
gby
fron
tal i
ndi
vid
ual
pe
per
ech
i gru
pe
ech
ipe
3 an
tr.
7 an
tr/1
5 m
inut
e
Tot
al: 3
75'
(6,2
5 h)
se
u
rmăr
eşte
d
oza
rea
cor
ectă
a m
ijloa
celo
r se
cor
ecte
aza
gr
eşel
ile t
rece
rii
prin
exe
cuţie
se c
orec
tea
za
greş
elile
tre
cerii
p
rin e
xecuţie
Să e
xecu
te s
tru
ctu
ri d
e a
cţiu
ni
mot
rice
cu e
lem
ente
de
coor
don
are
gen
era
lă
12 a
ntr
. M
etod
e: jo
cul,
exer
sare
a,
pro
ble
ma
tiza
rea
,
Mijl
oace
:
jocu
ri d
e m
işca
re, ş
tafe
te,
pa
rcu
rsu
ri
ap
lica
tive,
exe
rciţii c
u m
inge
şi fără
min
ge,
exer
ciţii d
e
con
solid
are
a d
eprin
der
ilor
mot
rice
de
ba
ză şi
util
itar-
ap
lica
tive
Mat
eria
le: o
bie
cte,
min
gi d
e fo
tba
l, ha
ndba
l, vo
lei,
ten
is,
oin
ă,
ba
sch
et, r
ugb
y
fron
tal i
ndi
vid
ual
pe
per
ech
i gru
pe
ech
ipe
4 an
tr.
8 an
tr/1
5 m
inut
e
Tot
al: 4
80'
(8 h
)

Să f
ie c
apab
il să
com
bine
şi
să c
uple
ze d
iferit
e m
işcăr
i sp
ecifi
ce
coor
donă
rii în
judo
12 a
ntr
. M
etod
e: jo
cul,
exer
sare
a,
pro
ble
ma
tiza
rea
,
Mijl
oace
:
jocu
ri d
e m
işca
re,
şta
fete
, p
arc
urs
uri
ap
licat
ive,
exer
ciţii
cu m
inge
şi fără
min
ge,
exer
ciţii d
e co
nso
lida
re a
dep
rind
erilo
r m
otric
e d
e b
az
ă şi
util
itar-
ap
licat
ive,
exe
rciţii c
u
miş
cări
şi s
arc
ini m
otric
e p
entr
u m
emb
rele
su
per
ioa
re
şi in
ferio
are
sep
ara
t şi în
ace
laşi t
imp
, com
ple
xe t
eh
nice
Mat
eria
le: o
bie
cte,
min
gi d
e fo
tba
l, ha
ndba
l, vo
lei,
ten
is,
oin
ă,
ba
sch
et,
fron
tal i
ndi
vid
ual
pe
per
ech
i gru
pe
ech
ipe
4 an
tr.
8 an
tr/1
5 m
inut
e
Tot
al: 4
80'
(8 h
)
se
u
rmăr
eşte
doz
are
a c
orec
tă
a m
ijloa
celo
r se
core
ctea
ză gr
eşel
ile
trec
erii
prin
exec
uţie
Să-ş
i fo
rmez
e ca
paci
tate
a de
de
co
ncen
trar
e vo
lunt
ară şi
in
volu
ntară
8 an
tr.
Met
ode:
jocu
l, ex
ersa
rea
,
Mijl
oace
: şta
fete
, pa
rcu
rsu
ri ap
licat
ive,
exe
rci
ţii c
u m
ai m
ulte
min
gi
şi s
arc
ini d
iferit
e în
ace
laşi ti
mp
, ex
erciţ
ii cu
min
gea
la z
idu
l de
ant
ren
am
ent,
exe
rci
ţii în
con
diţii
va
riate
şi c
u în
greu
iere
Mat
eria
le: j
alo
an
e, m
ingi
de
teni
s, h
andb
al,
basc
het
, vo
lei,
fotb
al,
zid
ul d
e a
ntre
na
men
t
fron
tal i
ndi
vid
ual
pe
per
ech
i gru
pe
ech
ipe
2 an
tr.
6 an
tr/1
5 m
inut
e
Tot
al: 2
70'
(4,5
h)
se
u
rmăr
eşte
doz
are
a c
orec
tă
a m
ijloa
celo
r se
core
ctea
ză gr
eşel
ile
trec
erii
prin
exec
uţie
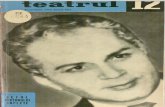
Pre
zent
area
gra
fică
a pr
ogre
sulu
i rea
lizat
pe
com
pone
ntel
e so
mat
ic, p
siho
mot
ric şi teh
nic
Rata
de p
rog
res în
tre
te
sta
re in
itia
la s
i te
sta
rea
inte
rme
dia
ra p
e c
om
po
nen
te
so
matic
,psih
om
ptr
ic,teh
nic 2
8%
61
%11
%
Rat
a de
pro
gre
s în
tre
test
are
inte
rme
diar
a s
i te
star
ea
fina
la p
e c
ompo
nent
e:
som
atic
, psi
hom
otri
c, t
ehn
ic
24%
64%
12%
Rat
a de
pro
gres
între
test
area
initia
la s
i tes
tare
a fin
ala
pe
com
pone
te:
som
atic
, psih
omot
ric, t
ehni
c. 26
%
63%11
%

11
Concluzii: ☯ Planificarea propusă şi utilizată de noi pentru instruirea tehnică este în concordanţă cu posibilităţile copiilor la acest nivel de vârstă; ☯ sistemele de acţionare propuse contribuie la dezvoltarea calităţilor psihomotrice specifice judo-ului; ☯ în procesul de instruire a copiilor, calităţile psihomotrice specifice se dezvoltă treptat, ele având o influenţă majoră în obţinerea de rezultate în competiţiile sportive; ☯ eşalonarea pregătirii copiilor se va face punând în concordanţă dezvoltarea calităţilor psihomotrice specifice cu particularităţile de vârstă şi individuale ale copiilor; ☯ sistemele de acţionare propuse de noi favorizează în acelaşi timp însuşirea unor procedee tehnice şi contribuie la dezvoltarea calităţilor psihomotrice; ☯ jocurile ştafetele şi traseele aplicative lărgesc plaja mijloacelor utilizate în procesul instruirii, îmbogăţesc conţinutul lecţiilor; ☯ jocurile, ştafetele şi traseele aplicative asigură participarea activă şi cu entuziasm a copiilor la antrenamente, le educă spiritul de echipă şi dau totodată posibilitatea antrenorului să-i cunoască mai bine, deoarece în timpul jocurilor copiii se manifestă liber, firesc, eliminând din comportament timiditatea. Bibliografie selectivă 1. ALBU A., ALBU C. "Psihomotricitatea La Varsta De Crestere Si Dezvoltare" – Edit. Spiru Haret, Iasi, 1999 2. DRAGNEA A., BOTA A., Teoria activitatilor motrice. Edit. Didactica si Pedagogica, Bucuresti,1999 3. EPURAN,M.,HOLDEVICI,I.,TONITA,I., "Psihologia sporului de performan - Edit. Fest, Bucuresti,2001 4.HORGHIDAN V .,Psihologie. Sinteza principalelor probleme abordate in cadrul cursurilor si lucrarilor practice. Academia Nationala de Educatie Fizica si Sport, Bucuresti,1999 5. KRAMAR, M ., Psihologia culturii fizice si a sporturilor. Arad, Edit. Fundatia Vasile Goldis, 1997 6. MANNO, R ., Bazele teoretice ale antrenamentului sportiv. Bucuresti, M.T.S.,C.C.P.S, 1996 7. NICU, Alexe si colab., Studii privind pregatirea sportiva a copiilor si juniorilor. Bucuresti, Edit. Stadion,1972
PLANING OPTIMIZATION OF EDUCATION AND DEVELOPMENT O F PSYCHOMOTRICITY FOR JUDOKA 10-11 YEARS SPORTSMEN
Adriana Neofit CSS Galaţi Mircea Ion – Ene FEFS Galaţi
It is known that to achieve performance in each sport and discipline so necessary
training in judo is best for each age level (stages) so that the most gifted athletes are able to properly take advantage of psychomotor skills, technical skills and theoretical knowledge.

12
Research Objectives: Judo is part of the individual sports which are characterized by the technically
dominant acyclic movements by requesting and cumulative effects on morphological aspects, functional and technical drivers of individual processes as fair fight.
Due to ever-higher performance, the training process should be revised both in form and content, improving training methods and criteria for creating new performance. Therefore we propose: ☯ Develop training plan and operating structures that could help optimize the training and achievement of groups of beginners in Judo; ☯ Preparation and use of games and pieces of advice for improving technique in judo applications drawn from the literature; ☯ Formulation of proposals for improving the quality of psychomotor development methodology and learning processes judo technique in groups of children 10-11 years.
Organize and conduct study: Our intention was from the outset, to optimize scheduling, planning and enrich the
range of operating systems for the development of psychomotor qualities and learning specific techniques of judo athletes from 10-11 years.
Therefore, to the plans and proposed means in the literature, we used only one program, planning and operators selected and adapted by us at this age.
The experiment was conducted at room Galati Judo Club School Sports in September 2009 - June 2010 included a total of 15 judo athletes.
Subjects covered by the research groups are part of the judo program in the School Sports Club Galati.
It follows an OPTIMIZED MICROCYCLU for education and development of the
components of psychomotricity from 10 to 11 years .

FIE
LD:
spor
ts tr
aini
ng, S
UB
JEC
T: J
UD
O
DU
RA
TIO
N: 3
5 w
eeks
(14
0 tr
aini
ngs.
) / 8
0-90
min
utes
per
trai
ning
A
ge g
roup
: 10-
11 y
ears
T
EA
CH
ING
ST
RA
TE
GY
FIN
AL
OB
JEC
TIV
ES
/
BA
CK
GR
OU
ND
N
umbe
r of
tr
aini
ng
3M
F.O
RG
.
TE
AC
HIN
G T
IME
M
etho
dica
l ind
icat
ions
To
unde
rsta
nd th
e bo
dy`s
ow
n sc
hem
e 8
tra
in.
Met
hods
: pla
y, p
ract
ice,
imita
tion
M
eans
: m
ovin
g ga
mes
, ex
erci
ses
in a
thle
tics
(opt
ions
fo
r w
alk
ing,
ru
nnin
g),
gym
na
stic
s (e
xerc
ises
fro
nt
and
b
and
s, h
arm
onio
us
phys
ica
l dev
elop
men
t)
Mat
eria
ls: s
ticks
, hoo
ps,
ma
ts
ind
ivid
ua
l p
airs
te
am
s fr
ont
grou
ps
2
tra
in.
6
trai
n.|
15
m
inut
es
tota
l: 27
0m
in`
;(4
.5 h
) p
ass
ing
thro
ugh
im
ple
men
tatio
n m
ista
kes
to b
e co
rrec
ted
To
know
the
plan
s of
act
ion
of th
e bo
dy
and
its p
arts
8
tra
in.
Met
hods
: pla
y, p
ract
ice,
imita
tion
M
eans
: m
ovin
g ga
mes
, ex
erci
ses
in a
thle
tics
(opt
ions
for
wa
lkin
g, r
unni
ng,
ju
mp
ing)
, gy
mn
ast
ics
(exe
rcis
es
fron
t an
d b
and
s,
ha
rmon
iou
s ph
ysic
al
dev
elop
men
t,
sta
tic a
nd
dyn
am
ic e
lem
ents
of a
crob
atic
s)
Mat
eria
ls:
ba
lls o
f d
iffer
ent
size
s a
nd
wei
ghts
, m
ats,
con
es
ind
ivid
ua
l p
airs
te
am
s fr
ont
grou
ps
2
tra
in.6
. tr
ain
./15
m
inut
es
tota
l: 27
0`
;(4.
5 h
) se
ekin
g w
ork
in
pai
rs
clos
e in
va
lue
Syn
chro
nize
the
ir m
ovem
ents
and
bod
y se
gmen
t as
a w
hole
8
tra
in..
M
etho
ds: p
lay,
pra
ctic
e, im
itatio
n, p
rob
lem
M
eans
: d
yna
mic
ga
mes
, re
lay
run
s,
app
licat
ion
exer
cise
s in
ath
letic
s, g
ymn
ast
ics
Mat
eria
ls: l
and
ma
rks,
ban
ks,
gym
, ob
sta
cles
ind
ivid
ua
l p
airs
te
am
s fr
ont
grou
ps
2
trai
n..
6
tra
in/1
5
min
utes
to
tal:
270
` ;(
4.5
h)
pa
ssin
g th
rou
gh
imp
lem
enta
tion
mis
take
s to
be
corr
ecte
d
To
acqu
ire
spat
ial
conc
epts
of
th
e tr
ajec
tory
, di
stan
ce,
size
, po
sitio
n an
d sh
ape
8 t
rain
. M
etho
ds: p
lay,
pra
ctic
e, p
rob
lem
M
eans
: d
yna
mic
ga
mes
, re
lay
run
s,
app
licat
ion
exer
cise
s to
lea
rn b
asi
c m
otor
ski
lls (
catc
hin
g, th
row
ing)
a
nd u
tility
app
lica
tion
s (t
ran
spor
t di
fficu
lties
, cl
imbi
ng,
cl
imbi
ng)
M
ater
ials
: b
alls
of
d
iffer
ent
size
s a
nd
w
eigh
ts,
obst
acle
s, t
rain
ing
wa
ll
ind
ivid
ua
l p
airs
te
am
s fr
ont
grou
ps
2
trai
n
6.
trai
n/1
5
m
inut
es
tota
l: 27
0`
;(4.
5 h
) se
ekin
g w
ork
in
pai
rs
clos
e in
va
lue
To
acqu
ire
the
skill
s of
sp
atia
l or
ient
atio
n,
and
asse
ssin
g te
mpo
rary
pa
ths,
dire
ctio
ns a
nd s
peed
s of
mov
ing
obje
cts
in c
onju
nctio
n w
ith y
our
own
body
10
trai
n.
Met
hods
: pla
y, e
xerc
ise,
M
eans
: d
yna
mic
ga
mes
, re
lay
run
s,
app
licat
ion
exer
cise
s w
ith b
all
Mat
eria
ls:
con
es,
tenn
is
balls
, ha
ndb
all,
b
ask
etba
ll,
volle
yba
ll, s
occe
r, o
bst
acl
e tr
ain
ing
wa
ll
ind
ivid
ua
l p
airs
te
am
s fr
ont
grou
ps
3
tra
in
7.
trai
n./1
5
m
inut
es
tota
l: 37
5`
;(6.
25 h
) p
ass
ing
thro
ugh
im
ple
men
tatio
n m
ista
kes
to b
e co
rrec
ted
To
be a
ble
to p
erfo
rm a
mot
or t
ask
or
mor
e co
mbi
ned
into
a
rhyt
hm
and
tem
po r
equi
red
12
trai
n.
Met
hods
: pla
y, e
xerc
ise,
M
eans
: d
yna
mic
ga
mes
, re
lay
run
s ap
plic
atio
ns,
exec
utio
n o
f m
otor
ta
sks
or c
omb
inat
ion
s of
ta
sks
in a
d
rivin
g rh
yth
m a
nd
tem
po
requ
ired
M
ater
ials
: co
nes
, te
nnis
ba
lls,
han
dba
ll,
ba
sket
ball,
vo
lleyb
all,
soc
cer,
hu
rdle
s, g
ymn
ast
ics
ben
ches
ind
ivid
ua
l p
airs
te
am
s fr
ont
grou
ps
20
trai
n.|
15
min
utes
/ 6
0 t
rain
. T
ota
l: 2
300
` ;(
38
h)
aim
ed a
t co
ntr
ollin
g th
e m
ean
s of
go
ing
thro
ugh
th
e co
rrec
t im
ple
men
tatio
n e
rror
s
To
achi
eve
the
mai
nten
ance
of
vo
lunt
ary
cont
rol
of s
tatic
equ
ilibr
ium
po
sitio
ns a
nd d
ynam
ic
10
trai
n.
Met
hods
: pla
y, p
ract
ice,
sis
tem
atiz
atio
n
Mea
ns:
dyn
am
ic
gam
es,
rela
y ru
ns,
ap
plic
atio
n ex
erci
ses
wa
lkin
g,
run
nin
g a
nd
jum
pin
g w
hile
m
ain
tain
ing
ba
lanc
e on
diff
eren
t su
rfac
es
Mat
ebria
le:
obst
acl
es,
gym
na
stic
s b
anks
, sl
opes
, m
obile
boa
rds,
tra
mp
olin
e sp
ring
ind
ivid
ua
l p
airs
te
am
s fr
ont
grou
ps
3
trai
n
7
tra
in.
/15
min
utes
to
tal:
375
` ;(
6.25
h)
pa
ssin
g th
rou
gh
imp
lem
enta
tion
mis
take
s to
be
corr
ecte
d

To
be a
ble
to o
rgan
ize
activ
ities
and
m
otiv
ity
stru
ctur
es
in
both
pl
ans
of
late
ralit
y d
rivin
g se
gmen
ts o
f th
e bo
dy
usin
g bo
th th
e rig
ht a
nd le
ft si
de
10
trai
n.
Met
hods
: pla
y, p
ract
ice,
sis
tem
atiz
atio
n
Mea
ns:
dyn
am
ic
gam
es,
rela
y ru
ns,
a
pplic
atio
n-
thro
win
g ex
erc
ises
h
old
ing
obje
cts,
d
rivin
g th
e b
all,
b
oth
with
his
arm
(le
g) a
dro
itly
and
with
th
e cl
um
sy,
tra
nsp
ort d
iffic
ulti
es
Mat
eria
ls: o
bjec
ts, g
ymn
ast
ics
ben
ches
ind
ivid
ua
l p
airs
te
am
s fr
ont
grou
ps
3
trai
n
7.
trai
n/1
5
m
inut
es
tota
l: 37
5`
;(6.
25 h
) a
imed
at c
ontr
ollin
g th
e m
ean
s
To
perc
eive
and
rea
ct a
s qu
ickl
y an
d ef
fect
ivel
y to
vi
sual
an
d au
dito
ry
stim
uli
12
trai
n.
Met
hods
: pla
y, p
ract
ice,
sis
tem
atiz
atio
n
Mea
ns:
dyn
am
ic
gam
es,
rela
y ru
ns
app
licat
ions
, ru
nnin
g w
ith
laye
rs
of
diff
ere
nt
pos
ition
s in
va
riou
s vi
sua
l and
aud
itory
sig
na
ls
Mat
eria
ls:
obje
cts
of
diff
eren
t co
lors
a
nd
sh
apes
, ob
stac
les
ind
ivid
ua
l p
airs
te
am
s fr
ont
grou
ps
4 t
rain
.8 t
rain
| 1
5 m
inut
es /
.
Tot
al:4
80
’ ` ;(
8 h
) a
imed
at c
ontr
ollin
g th
e m
ean
s
to p
erce
ive
and
reac
t as
qui
ckly
and
ef
fect
ivel
y to
stim
uli t
hat
ma
ke p
ossi
ble
perc
eptio
n of
the
ir m
ovem
ents
(si
lulu
i K
ines
thet
ic)
12
trai
n.
Met
hods
: pla
y, p
ract
ice,
qu
estio
nin
g, im
itatin
g M
eans
: m
ovin
g ga
mes
, re
lay
run
s, a
pplic
atio
n e
xerc
ises
in
va
riou
s co
nditi
ons
and
bu
rden
ed
Mat
eria
ls: o
bjec
ts, g
ymn
ast
ics
ben
ches
ind
ivid
ua
l p
airs
te
am
s fr
ont
grou
ps
4
tra
in.8
tr
ain
|1
5
min
ute
s /
Tot
al:
48
0(8
h)
corr
ects
er
rors
b
y e
xecu
ting
tra
nsi
tion
To
be a
ble
to r
ealig
n th
eir
perc
eptio
ns
of t
he d
egre
e of
mus
cle
tens
ion
(mus
cle
tone
)
10
trai
n.
Met
hods
: pla
y, p
ract
ice,
qu
estio
nin
g, im
itatin
g M
eans
: m
ovin
g ga
mes
, re
lay
run
s, a
pplic
atio
n e
xerc
ises
of
h
ittin
g ba
lls
with
le
g w
eigh
ts
and
si
zes
an
d
at
diff
eren
t di
stan
ces
from
fix
ed
and
m
obile
ta
rget
s,
exer
cise
b
alls
a
nd
th
row
ing
of
obje
cts
of
diff
eren
t w
eigh
ts a
nd s
izes
at
diffe
ren
t d
ista
nce
s an
d fix
ed o
r m
obile
M
ater
ials
: ob
ject
s,
gym
b
ench
es,
fixed
a
nd
m
obile
ta
rget
s, fo
otba
lls,
han
dba
ll, v
olle
yba
ll, t
enn
is,
oin
a, b
ask
ind
ivid
ua
l p
airs
te
am
s fr
ont
grou
ps
3
trai
n
7
tra
in.
/15
min
utes
to
tal:
375
` ;(
6.25
h)
aim
ed a
t co
ntr
ollin
g th
e m
ean
s of
go
ing
thro
ugh
exe
cutio
n e
rror
s a
re
corr
ecte
d
corr
ects
er
rors
b
y e
xecu
ting
tra
nsi
tion
P
erfo
rm
the
actio
n st
ruct
ures
w
ith
elem
ents
of
dr
ivin
g ov
eral
l co
ordi
natio
n
12
trai
n.
Met
hods
: pla
y, p
ract
ice,
sis
tem
atiz
atio
n
Mea
ns:
mov
ing
gam
es,
rela
y ru
ns,
app
licat
ion
exe
rcis
es
with
out
the
ball
and
ba
ll ex
erc
ises
to
stre
ngt
hen
th
e b
asi
c m
otor
ski
lls a
nd t
ool-a
pplie
d
Mat
eria
ls:
obje
cts,
fo
otb
alls
, ha
ndba
ll,
volle
yba
ll,
ten
nis,
oin
a, b
ask
etb
all,
ru
gby
ind
ivid
ua
l p
airs
te
am
s fr
ont
grou
ps
4 t
rain
8 t
rain
|. 15
min
utes
.
Tot
al:
48
0`
;(8
h)
T
o be
abl
e to
com
bine
and
coo
rdin
ate
enga
ges
diffe
rent
spe
cific
mov
emen
ts in
Ju
do
12
trai
n.
Met
hods
: pla
y, e
xerc
ise,
sis
tem
atiz
atio
n,
Mea
ns:
mov
ing
gam
es,
rela
y ru
ns,
app
licat
ion
exe
rcis
es
with
out
the
ball
and
ba
ll ex
erc
ises
to
stre
ngt
hen
th
e sk
ills
ba
se a
nd u
tility
-driv
en,
app
lica
tion
exe
rcis
es w
ith
mov
emen
ts a
nd m
otor
ta
sks
for
the
upp
er a
nd
low
er
limb
s se
para
tely
a
nd
a
t th
e sa
me
time,
co
mp
lex
tech
nic
al
Mat
eria
ls:
obje
cts,
fo
otb
alls
, ha
ndba
ll,
volle
yba
ll,
ten
nis,
oin
a, b
ask
etb
all,
ind
ivid
ua
l p
airs
te
am
s fr
ont
grou
ps
4 t
rain
8 t
rain
|. 1
5 m
inut
es /
60
entr
epre
. T
ota
l: 4
80
` ;(
8 h
) a
imed
at
con
trol
ling
the
mea
ns
of
goin
g th
rou
gh
the
corr
ect
imp
lem
enta
tion
err
ors
To
build
ca
paci
ty
of
volu
ntar
y an
d in
volu
ntar
y co
ncen
trat
ion
8 t
rain
. M
etho
ds: p
lay,
exe
rcis
e,
Mea
ns:
rela
y p
ass
es,
app
lica
tion
exer
cise
s w
ith b
alls
a
nd s
ever
al
diff
eren
t ta
sks
at t
he
sam
e tim
e, e
xerc
ises
w
ith t
he
ba
ll a
t th
e w
all
tra
inin
g ex
erci
ses
in v
ario
us
con
ditio
ns
and
burd
ened
M
ater
ials
: co
nes
, te
nnis
ba
lls,
han
dba
ll,
ba
sket
ball,
vo
lleyb
all,
soc
cer
tra
inin
g w
all
ind
ivid
ua
l p
airs
te
am
s fr
ont
grou
ps
2
trai
n
6.
trai
n/1
5
m
inut
es
tota
l: 27
0`
;(4.
5 h
) a
imed
at
con
trol
ling
the
mea
ns
of
goin
g th
rou
gh
the
corr
ect
imp
lem
enta
tion
err
ors

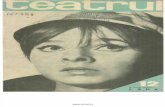
Pre
zent
area
gra
fică
a pr
ogre
sulu
i rea
lizat
pe
com
pone
ntel
e som
atic
, psi
hom
otric
şi t
ehni
c
Rata
de p
rog
res în
tre
te
sta
re in
itia
la s
i te
sta
rea
inte
rme
dia
ra p
e c
om
po
nen
te
so
matic
,psih
om
ptr
ic,teh
nic 2
8%
61
%11
%
Rat
a de
pro
gre
s în
tre
test
are
inte
rme
diar
a s
i te
star
ea
fina
la p
e c
ompo
nent
e:
som
atic
, psi
hom
otri
c, t
ehn
ic
24%
64%
12%
Rat
a de
pro
gres
între
test
area
initia
la s
i tes
tare
a fin
ala
pe
com
pone
te:
som
atic
, psih
omot
ric, t
ehni
c. 26
%
63%11
%

16
Conclusions: ☯ Plan proposed and used by us is consistent with the technical training opportunities at this children age; ☯ proposed drive systems contribute to the development of specific psychomotor qualities of judo; ☯ in the training of children, specific psychomotor skills develop gradually,having a major influence in achieving results in sporting competitions; ☯ timing will be putting children training in line with the specific psychomotor skills development and individual features age children; ☯ proposed new operating systems while favoring the acquisition of technical processes and contribute to the development of psychomotor qualities; ☯ pieces of advice games and beach trails extend applications used in training resources, enrich the content of lessons; ☯ games, pieces of advice and applied routes ensure active participation and enthusiasm of children to train, educate their team spirit and also give the coach the opportunity to know better, because it occurs during the games children free, quite naturally, eliminating the shy behavior.
CORELAŢIA DINTRE CAPACITATEA DE REGLARE A PARAMETRILOR
DINAMICI ŞI PREGĂTIREA FIZIC Ă A JUCĂTORILOR DE HANDBAL
BAŞTIUREA EUGEN – FEFS GALAŢI
Cuvinte cheie: antrenament sportiv, handbal, pregătire fizică, capacităţi de coordonare Rezumat: Jocul de handbal este un joc dinamic axat pe o bună pregătire fizică şi un bagaj tehnico-tactic complex, ceea ce face ca şi procesul de instruire să fie conceput, dozat şi planificat la un nivel superior. În consecinţă, antrenamentele vor avea în structura lor o gamă diversificată de metode şi mijloace de instruire care să ducă la îmbunătăţirea măiestriei sportive. Astfel, jucătorii de handbal vor dobândi o bună viteză de deplasare şi execuţie, rezistenţă specifică şi un grad sporit de coordonare, calităţi motrice atât de necesare pentru execuţiile din timpul jocului.
Introducere Nevoia de rezultate sportive favorabile obţinute într-un timp scurt şi ritm permanent, precum şi valoarea tot mai crescută a adversarilor obligă antrenorii de astăzi să fie foarte atenţi la conceperea, dozarea şi planificarea procesului de instruire a sportivilor. Şansa acestora o reprezintă evoluţia ştiinţei sportului cea care vine să influenţeze în mod real performanţa sportivă şi modul de desfăşurare a procesului de antrenament. Descoperirile oamenilor de ştiinţă ajută antrenorii să ducă la bun sfârşit obiectivele propuse privind creşterea nivelului de efort şi performanţă al sportivilor.
Sportivii cu o bună dezvoltare fizică îşi pot îmbunătăţi mai repede performanţele motrice, tehnice şi sportive comparativ cu cei lipsiţi de acest fundament. Amplul proces de instruire determină dezvoltarea fizică multilaterală a sportivilor, ceea ce constituie suportul

17
energogenetic în baza căruia se desfăşoară jocul modern. Este dezvoltată forţa şi rezistenţa, îmbunătăţită viteza şi perfecţionată coordonarea, situaţie ce duce implicit la creşterea performanţelor sportive.
Capacităţile de coordonare reprezintă un complex de calităţi preponderent psiho-miotrice (Dragnea A., Bota A., 1999), iar dezvoltarea acestora este strâns legată de evoluţia fiziologică a individului întrucât organismul este permanent supus unor schimbări funcţionale, morfologice şi biochimice.
O serie de specialişti ai domeniului consideră capacitatea de coordonare ca fiind un „întreg” cu o structură complexă şi un număr mare de „capacităţi” ce sunt destinate pentru activităţi preponderent coordinative (Blume D.D., 1978, 1984; Bompa T.O., Carrera M.C., 2006; Hirtz P., Ludwig G., Willnitz J., 1981, 1982).
Pentru realizarea cercetării am folosit clasificarea concepută de Platonov V.N. (1997),
iar pentru calcularea coeficientului de corelaţie am selecţionat doar prima „capacitate de coordonare”:
1. Capacitatea de apreciere şi reglare a parametrilor dinamici, spaţiali-temporali a actului motric.
2. Capacitatea de menţinere a echilibrului. 3. Simţul de ritmicitate. 4. Capacitatea de orientare în spaţiu. 5. Capacitatea de relaxare automată a muşchilor. 6. Capacitatea de coordonare a mişcărilor.
Fără coordonare, echilibru, reflexe şi ritm, fără gândire creatoare şi spirit combativ nu se poate ajunge la marea performanţă (Ludu V., 1983).
În final, putem spune că jocul de handbal solicită foarte mult sportivii şi, totodată, îi obligă să participe în mod conştient la procesul de instruire. Această implicare a sportivilor presupune concentrarea tuturor resurselor fizice şi tehnico-tactice pentru a putea rezolva cu succes sarcinile de antrenament şi joc.
Ipoteza de lucru: - reglarea parametrilor dinamici şi spaţio-temporali influenţează nivelul de pregătire
fizică al jucătorilor de handbal? Metodele cercetării Pentru îndeplinirea obiectivelor studiului nostru s-a recurs la următoarele metode de
cercetare: - metoda studiului bibliografic; - metoda testelor; - metoda experimentului; - metoda statistico-matematică; - metoda tabelară.
Desfăşurarea experimentului
Eşantionul de subiecţi a fost alcătuit din 15 sportivi, componenţi ai echipei de handbal C.S.U. Galaţi, cu vârste cuprinse între 19 şi 32 de ani. Aceştia au parcurs un proces de instruire atractiv, dinamic şi complex pentru îmbunătăţirea pregătirii fizice şi dezvoltarea capacităţii de coordonare.
În cadrul experimentului, cei 15 sportivi au fost evaluaţi din punct de vedere fizic şi al coordonării, iar în baza rezultatelor obţinute s-a trecut la determinarea gradului de corelaţie existent între aceşti parametri (tabelul 1 şi tabelul 2).

18
Tabelul 1
Rezultatele dezvoltării capacităţii de coordonare a jucătorilor de handball
m±X
Grupa experiment Grupa martor CAPACITATE DE COORDONARE
INDICI
AI
COORDONĂRII T.I. T.F. t p T.I. T.F. t p t1 P
Aruncarea mingii în ţintă, stând cu spatele la ea (30 mingi) [puncte]
60,07 ± 3,81
72,13 ± 1,17
3,03 <0,01 53,00 ± 3,12
56,13 ± 2,54
0,78 >0,05 5,72 <0,01
Sărituri la marcare [cm] 2,63
± 0,21 1,30
± 0,15 5,10 <0,01
2,90 ± 0,75
2,45 ± 0,21
0,58 >0,05 4,43 <0,01
Capacitatea de apreciere şi reglare a parametrilor dinamici, spaţiali-temporali a actului motric Diferenţa încordării
musculare a braţului îndemânatic [kg/F]
-2,97 ± 0,59
-2,80 ± 0,75
0,17 >0,05 -3,67 ± 0,82
-3,27 ± 0,74
0,36 >0,05 0,44 >0,05
Legendă: “t” - s-a calculat între indicatorii iniţiali şi finali ai fiecărei grupe; “t 1”- s-a calculat între indicatorii finali ai grupelor martor şi experiment;
“p”- tabela lui Fisher la pragul de semnificaţie 0,01-0,05, în conformitate cu eşalonul cercetat. Notă: rezultatele sunt date în valoare absolută.
Tabelul 2 Rezultatele corelaţiei dintre indicii capacităţii de coordonare şi indicii motrici ( r )
Probe fizice
Pentasalt
CAPACITA
TE DE COORDON
ARE
INDICI
AI
COORDONĂRII 5 x
30
m
De
pla
sare
în
tr
iung
hi
Co
mb
ina
ta
Sărit
ura
în
lun
gim
e de
p
e lo
c
Picior stâng
Picior drept
Abd
om
en
2 x
400
m
800
m
Te
stu
l de
sprin
t
Aruncarea mingii în ţintă, stând cu spatele la ea
r = - 0.036 - 0.173 0.056 - 0.241 0.022 - 0.325 - 0.325 0.101 0.174 0.023
Sărituri la marcare
r = 0.268 0.124 - 0.235 - 0.202 - 0.060 0.094 0.094 - 0.113 0.495 0.080
Capacitatea de apreciere şi reglare a parametrilor dinamici, spaţiali-temporali a actului motric
Diferenţa încordării musculare a braţului îndemânatic
r = - 0.321 - 0.214 0.119 0.124 0.109 0.156 0.156 0.285 0.238 -
0.074
Legendă: - r = coeficientul de corelaţie (indică forţa legăturii între cele două valori; cu cât
legătura este mai strânsă cu atât valoarea coeficientului de corelaţie „r” se apropie de valoarea 1; valorile lui „r” sunt cuprinse între 1 şi -1)
Interpretare: - r = 0,20 – corelaţie aproape inexistentă; - r = 0,20 ÷ 0,40 – corelaţie aproape moderată; - r = 0,40 ÷ 0,60 – corelaţie moderată; - r = 0,70 ÷ 0,90 – corelaţie înaltă; - r = 0,90 ÷ 0,100 – corelaţie foarte înaltă (după Guilford).
Concluzii Analizând valorile coeficienţilor de corelaţie dintre capacitatea de apreciere şi reglare
a parametrilor dinamici, spaţiali-temporali a actului motric şi pregătirea fizică, pot fi trase următoarele concluzii:

19
- din numărul total de 30 de indici folosiţi pentru evaluarea jucătorilor de handbal s-a obţinut o corelaţie „aproape moderată” în procent de 33,3% (10 indici), o corelaţie „moderată” în procent de 3.33% (un indice) şi o corelaţie „aproape inexistentă” în proporţie de 63,33% (19 indici);
- din cei 3 indici ai coordonării folosiţi pentru aflarea gradului de corelaţie şi ceilalţi 10 indici motrici, „săriturile la marcare” se situează pe primul loc cu cele mai multe valori care se apropie mai mult de cifra 1;
- cel mai bun nivel de corelaţie există între “Săriturile la marcare” şi proba fizică „800 m” (r = 0,495);
- cel mai scăzut nivel de corelaţie există între “Aruncarea mingii în ţintă, stând cu spatele la ea” şi proba fizică „Pentasalt - piciorul stâng” (r = 0,022).
Întrucât s-au înregistrat valori scăzute la 19 coeficienţi din cei 30 folosiţi, putem concluziona că nu există un grad ridicat de corelaţie între această primă capacitate de coordonare luată în studiu „capacitatea de apreciere şi reglare a parametrilor dinamici, spaţiali-temporali a actului motric” şi indicii fizici aleşi pentru testarea handbaliştilor seniori.
Bibliografie BAŞTIUREA E., Dezvoltarea capacităţilor de coordonare a handbaliştilor seniori în cadrul antrenamentului individualizat, în dependenţă de postul de joc, Teză de doctorat, INEFS Chişinău, Republica Moldova, 2004. BLUME D. D., Grundsatze und methodische ma bnahmen zur schulung koordinativer//Korpererziehung, nr. 2, 1978. BLUME D. D., Enige aktualle probleme des diagnostizierens koordinativer motorischen test//Korperkultur,nr.2, 1984. BOMPA T.O., CARRERA M.C., Periodizarea antrenamentului sportiv. Planuri ştiinţifice pentru forţă şi condiţia fizică pentru 20 de discipline sportive, Editura Tana, 2006. DRAGNEA A., BOTA A., Teoria activităţilor motrice, Editura Didactică şi Pedagogică R.A., Bucureşti, 1999. HIRTZ P., LUDWIG G., WELLNITZ J., Potenzen des sportunterriehtz und ihre nitzung fiir die ausbildung und vervollhommnung koordinativer tatigkeiten // Theorie und Praxis der Korperkultur, nr. 9, 1981. HIRTZ P., LUDWIG G., WELLNITZ J., Entwicklung koordinativer Tatigkeiten.Ja, aber wie?// Korpererziehung, nr. 8/9, 1982. LUDU V., Ritmul şi performanţa, Editura Sport-Turism, Bucureşti, 1983. ПЛАТОНОВ В.Н., Общая теория подготовки спортсменов в олимпийском спорте // Олимпийская литература, Киев, 1997. THE CORRELATION BETWEEN THE CAPACITY OF REGULATING THE DYNAMIC PARAMETER AND THE PHYSICAL TRAINING OF
THE HANDBALL PLAYERS
BAŞTIUREA EUGEN – FEFS GALAŢI
Key words: sportive training, handball, physical training, coordination capacities Summary: Handball is a dynamic game centred on a good physical training and on a complex technical-tactical luggage that make the instruction process to be conceived,

20
measured and planned at a superior level. Consequently, the trainings will have in their structure a various range of instruction methods and ways that will bring about the improvement of the sportive mastery. So, the handball players will get a good speed of the change of place and execution, specific resistance and a bigger degree of coordination, driving qualities so necessary for the executions during the play.
Introduction The need for favourable sportive results obtained in a short time and permanent rhythm, as well as the bigger value of the opponents compel today's coaches to be very careful at the conceive, measure and the planning of the sports men's instruction process. Their chance is the evolution of the sports science that comes to really influence the sportive performance and the way of the progress of the training process. The scientists' discoveries help the coaches achieve the proposed objectives regarding the increase of the sportsmen's effort and performance level.
The sportsmen with a good physical development care improve faster their driving, technical and sportive performances in comparison with those who lack this foundation. The ample instruction process determines the sports men's multilateral physical development that is the energogenetic support according to which the modern game takes place. It is developed the force and the resistance, the speed improved and the coordination perfected, situation that brings about the increase of the sportive performances.
The coordination capacities represent a complex of prevalent psycho-driving qualities (Dragnea A., Bota A., 1999), and their development is tightly tied to the physiological evolution of the person because the body is permanently subjected to some functional, morphological and biochemical changes.
A series of specialists in the field consider the coordination capacity as being a “whole” with a complex structure and a big number of “capacities” that are destinated to the prevalent coordinative activities (Blume D.D., 1978, 1984; Bompa T.O., Carrera M.C., 2006; Hirtz P., Ludwig G., Willnitz J., 1981, 1982).
To achieve the research we used the classification made by Platonov V.N. (1997), and for the calculation of the correlation coefficient we selected only the first “coordination capacity”:
1. The capacity of estimating and regulating of the dynamic, spatial-temporal parameters of the driving act.
2. The capacity of maintaining the balance. 3. The rhythmically sense. 4. The capacity of spatial orientation. 5. The capacity of automatic relaxation of the muscles. 6. The capacity of the coordination of the movements.
Without coordination, balance, reflexes and rhythm, without creative thinking and militant spirit, one can't reach the great performance (Ludu V., 1983).
Finally, we can say that handball challenges the sportsmen very much and, at the same time, compels them to consciously participate at the instruction process. This involvement of the sportsmen means the concentration of all physical and technical-tactical resources to successfully solve the training and play tasks.
The working hypothesis: - does the regulation of the dynamic and special-temporal parameters influences the
level of the physical preparation of the handball players?

21
The methods of the research To achieve the objectives of our study we resorted to the following research methods:
- the method of the bibliographic study; - the tests method; - the experiment method; - the statistical-mathematic method; - the table method.
The progress of the experiment The sample of subjects consisted of 15 sportsmen, components of the CSU Galati
handball team, with ages between 19 and 32. They had an attractive, dynamic and complex instruction process to improve the physical preparation and the development of the coordination capacity.
In the experiment, the 15 sportsmen were evaluated from the coordination and physical point of view, and according to the obtained results we passed to the establishment of the correlation degree extant between these parameters (table 1 and table 2).
Table 1
The results of the development of the coordination capacity of
the handball players
m±X
Experimental group Control group COORDINATION
CAPACITY COORDINATION
INDEXES
T.I. T.F. t p T.I. T.F. t p t1 P
The throwing of the ball in the target, standing with the back at it (30 balls) [points]
60,07 ± 3,81
72,13 ± 1,17
3,03 <0,01 53,00 ± 3,12
56,13 ± 2,54
0,78 >0,05 5,72 <0,01
Jumpings at scoring [cm] 2,63
± 0,21 1,30
± 0,15 5,10 <0,01
2,90 ± 0,75
2,45 ± 0,21
0,58 >0,05 4,43 <0,01
The capacity of estimating and regulating of the dynamic and spatial-temporal parameters of the driving act
The difference of the muscular strain of the deft arm [kg/F]
-2,97 ± 0,59
-2,80 ± 0,75
0,17 >0,05 -3,67 ± 0,82
-3,27 ± 0,74
0,36 >0,05 0,44 >0,05
Legend: “t” - was calculated between the initial and final indicators of each group; “t 1”- was calculated between the final indicators of the control and experimental group; “p”- Fisher's table at the signification edge 0.01-0.05 according to the studied sample.
Note: the results are given in absolute value.

22
Table 2 The results of the correlation between the index of the coordination capacity and the driving
index ( r ) Physical tests
Pentasalt COORDINATION CAPACITY
COORDINATION INDEXES
5 x
30
m
Cha
nge
of
pla
ce in
tr
iang
le
Co
mb
ined
Th
e lo
ng
jum
p fro
m a
p
lace
Left leg Right leg
Abd
om
en
2 x
400
m
800
m
Th
e s
prin
t te
st
The throwing of the ball in the target, standing with the back at it
r = - 0.036 - 0.173 0.056 - 0.241 0.022 -
0.325 -
0.325 0.101 0.174 0.023
Jumpings at scoring
r = 0.268 0.124 -
0.235 - 0.202 - 0.060 0.094 0.094 - 0.113 0.495 0.080
The capacity of estimating and regulating of the dynamic and spatial-temporal parameters of the driving act
The difference of the muscular strain of the deft arm
r = - 0.321 - 0.214 0.119 0.124 0.109 0.156 0.156 0.285 0.238 -
0.074
Legend: r = the correlation coefficient (it shows the force of the link between the 2 values; the tighter the link is more the value of the correlation coefficient “r” comes up to 1; the values of “r” are between 1 and -1)
Interpretation:
- r = 0,20 – almost inexistent correlation; - r = 0,20 ÷ 0,40 – almost moderate correlation;
- r = 0,40 ÷ 0,60 – moderate correlation;
- r = 0,70 ÷ 0,90 – high correlation;
- r = 0,90 ÷ 0,100 – very high correlation (according to Guilford). Conclusions Analyzed the values of the correlation coefficients between the capacity of estimating
and regulating the dynamic, spatial-temporal parameters of the driving act and the physical preparation, the following conclusions can be drawn:
- from the total number of 30 indexes used for the handball players' evaluation it was obtained an “almost moderate” correlation of 33.3% (10 indexes), a “moderate” correlation of 3.33% (one index) and an “almost inexistent” correlation of 63.33% (19 indexes);
- from the 3 indexes of the coordination used to find out the correlation degree and the others 10 driving indexes, “the jumpings at scoring” are on the first place with most of the values that come up to 1;
- the best correlation level is between “the jumpings at the scoring” and the physical test “800 m” (r = 0.495);
- the lowest correlation level is between “the throwing of the ball in the target, standing with the back at it“ and the physical test “Pentasalt - the left leg” (r = 0.022).
Because there were registered low values at 19 coefficients from those 30 used, we can conclude that it isn't a high correlation degree between this first coordination capacity studied “the capacity of estimating and regulating of the dynamic and spatial-temporal

23
parameters of the driving act” and the physical indexes chosen for the senior handball players' testing.
DANS SI IDENTITATE DE GEN TSIFT (E)-TELI DANCE ÎN F ARASSA,
KAPPADOKIA
Hariton Haritonidis A., Vasiliki K. Tyrovola Departamentul de Educaţie Fizică şi Sport Ştiinţei, Universitatea din Atena Kapodistrian
1. Introducere Tsift (e) dance-teli este un element integrant al realităţii dansului modern grec deoarece, cu ritmul său recunoscut instantaneu şi înălţător, acesta constituie o componentă esenţială a divertismentului grec contemporan (Raftis, 1996). Deşi tsift (e) de dans teli (dublu-coardă) astăzi apare ca fiind de genul neutru, practic este, dincolo de orice îndoială, de sex feminin. Tsift (e)-teli face parte din categoria specială de dansuri (Bucheld, 1996) în care predomină anumite mişcări, cum ar fi cele din partea superioară a corpului leganate sau discrete, mişcări ondulatorii ale trunchiului, arcuirea corpului în timp ce se inverseaza simultan mâinile ( Bucheld, 1996, şi Tyrovola, 2002). Mulţi termeni au fost folositi pentru a descrie acest dans, care sunt fie derivati din istoria sa, originile şi proprietăţi simbolice, cum ar fi : dans din burta , oriental , dans salomi , dans harem , horos ton epta peplon , sau de la modul de executare sau a conţinutului său teoretic, cum ar fi senzational , ecstatic, hieratic, dans hip , dans de fertilitate , (Petrides, 1976; Buchheld, 1996; Raftis, 1996; Tyrovola, 1999, 2002). Din cele de mai sus, ar putea fi trasa concluzia la prima vedere că, în ciuda multor nume, tsift (e) se referă la teli-dans în principiu, un anumit tip de dans popular-traditional asociat cu fertilitatea, care în decursul istoriei sale a dat nastere la diferiti hibrizi şi a fost inclus în repertoriul muzical şi dans de tradiţie urban (Tyrovola, 2002), sau a fost văzut conform criteriilor de folclor şi dans artistic (Shay & Sellers-Young, 2005). În plus, rapoartele post crestinismului timpuriu (Suchs, 1963), precum si ilustratii numeroase confirma conexiunea imediată a acestui dans, şi a diferitelor sale sub-forme, exclusiv cu sexul feminin, ca «... mişcarea viguroasa de sân, balansare a şoldurilor şi îndoire a trunchiului şi taliei pentru a obţine sensul exclusiv atunci când este angajat în scopul de a trezi şi excita masculin ... »(Tyrovola, 2002: 46-47). Se poate concluziona cu certitudine că diversele forme de tsift (e) dans teli îşi au originea în moştenirea etnologica comuna a poporului mediteranean si al Orientului Apropiat, din timpul primelor rapoarte cu date nominale specifice din perioada de dezvoltare a unor centre urbane în Imperiul Otoman (Tyrovola, 2002). Rapoarte ale tsift (e)-teli dans au venit din Grecia, şi în special din insulele din nord-estul Mării Egee, cum ar fi Chios (Tyrovola, 2002) şi Lesbos (Tyrovola,2010), din regiunea Macedonia, cum ar fi Irakleia, Serres (Papakostas, 2007), dar şi din regiuni, cum ar fi zona continentală a Asiei Mici, precum şi din tradiţia muzicală şi de dans a populaţiilor vorbitoare de limbă turcă şi ortodoxe de limbă greacă din Kappadokia , cum ar fi zona de Farassa, sau Misti şi altele. Interesant, deşi în funcţie de percepţia comună de Vest tsift (e)-teli este reprezentativ pentru un dans exclusiv feminin, în tradiţiile de Est, dansul este o chestiune atât de bărbaţi cat şi de femei, singura distincţie fiind dacă este dansat în public (bărbaţi) sau în particular (femei), precum şi în forma de dans. O situaţie similară poate fi observată în comunitatea ortodoxă de limbă greacă

24
din Farassa, în cazul în care tsift (e) se referă la ambele sexe şi reflectă organizarea sociala a comunitatii in special în ceea ce scoate în evidenţă relaţiile de gen în rândul membrilor comunităţii, prin mişcările de dans Revizuind literatura de specialitate, este clar că cele mai multe informaţii cu privire la exemplele de dans al tsift (e)-teli sunt de descriere etnografica si folclorica. (Margariti, 1987 şi Lambropoulos, 1994). Cercetarea, care este o excepţie de la această include activitatea de: Tyrovola (1992), în care tradiţia dansului la grecii din Kappadokia este prezentata prin utilizarea datelor etnografice, precum şi cu referire la ritmuri; Kotsia & Charitonidis (1998), care foloseste o analiză structural-morfologica pentru a atesta tsift (e) teli al grecilor din Kappadokian ca pe o categorie speciala de dans, care a inclus diverse forme de dans de bază (hetero-morphies); şi Tyrovola (2002) , care investighează problemele care apar între cultura populară şi dezvoltarea socială, folosind exemplul de tsift (e) de dans-teli. Din cele de mai sus, este clar că există o lipsa de studii privind tsift (e) de dans-teli ca un mijloc de gestionare şi de a evidenţia identitatea relationata la gen legate printr-o analiză a structurii si formei sale. 1.2. Scopul Scopul acestui studiu este investigarea formelor de dansuri” ta kousokka “si “I paigni mo ta houliere” din Farassa de Kappadokia, ca variaţii regionale ale tsift (e) de dans-teli aşa cum este folosit de fiecare sex. În special, studiul de faţă îşi propune să scoată în evidenţă relaţiile de gen în contextul societăţii tradiţionale din Farassa prin utilizarea formei de dans ca un instrument de analiză a structurii şi formei de dansuri menţionate mai sus, acesta din urmă fiind reprezentant al fiecarui sex. 1.3. Metodologie Datele au fost colectate prin metoda etnografica bazata pe surse primare şi secundare (Buckland, 1999; Giurchesku 1999; Koutsouba, 1999; Tyrovola, 2008). Sursele primare de date se referă la date colectate prin intermediul cercetarii de teren sub formă de interviu (Thompson, 2002) şi observarea participativă (Gefou-Madianou, 1999; Lydaki, 2001; Petronoti, 2002). În special, cercetarea de teren a fost realizată în luna februarie 1987 (preliminar) şi a fost finalizata în mai 2003, şi constituie o parte a unei cercetări mai ample privind identitatea culturală a refugiaţilor Kappadokian. Cercetarea a fost axata pe comunitatea de Plati din Imathia, Macedonia, locuita preponderent de refugiaţii din Farassa, Kappadokia. Sursele secundare se referă la date colectate prin cercetare etnografică (Stocking, 1983; Gefou-Madianou, 1999; Tyrovola, 2008). Analiza structural-morfologica şi tipologica cum este aplicata în Ethnochoreology (Tyrovola, 1994, 2001; Tyrovola, 2008) a fost utilizata pentru analiza formelor de dans, în timp ce metoda comparativă a fost utilizată pentru compararea formelor de dans (Holt & Turner, 1972 ; Vallier, 1973; Tyrovola, 2008). Pentru interpretarea datelor,a fost folosita gândirea antropologica pe identitatea de gen , aşa cum apare în aspectele antropologice ale dansului şi în special în Hanna (1987, 1988). Acesta este un model teoretic care considera percepţia de sex ca pe un domeniu de negociere, simbol cultural sau relaţie sociala (Strathern, 1976, 1988; Papataxiarchis, 1992), precum şi ca pe un criteriu de analiză a populaţiei locale (Papataxiarchis, 1992). 2. Analiza datelor Farassa, sau Varassos (nume grecesc care este folosit în zona încă din antichitate), este un oraş mare cu populaţie greacă (Loukopoulos & Petropoulos, 1949; Merlier, 1974; Tyrovola, 1990; Kikisoglou, 1997), în sud-estul Kappadokia, printre chei şi satele turceşti şi la o altitudine de 1050 metri. Potrivit lui Merlier, «... în 1923, grecii de Kappadokia (...) au ajuns în Grecia abandonandu-si patria lor pentru totdeauna ...» (1974:30). Refugiaţi din

25
Farassa s-au stabilit la marginea centrelor urbane din centrul Macedoniei şi al Thessaliei, dar majoritatea s-au stabilit în regiunea Katerini (Plati, Imathia). Tradiţia de dans a populaţiei din Farassa include dansuri circulare şi “antikristoi” (Lambropoulos, 1994:79), care se efectuează la ritm cu patru batai si noua batai (Tyrovola, 1996). Dansurile “antikristoi” la noua batai(“zeibekiko”; cu cutite) sunt dansate exclusiv de bărbaţi, în timp ce dansurile “antikristoi”la patru batai sunt separate pe barbate si femei deoarece rareori ar dansa un barbat cu o femeie - şi asta numai dacă ar fi rude apropiate. Dansurile “antikristoi” cu patru batai sunt caracterizate de acompaniamentul de instrumente idiophone, cum ar fi “zornaitoare” sau, linguri, ţinute de dansatori şi sunt dansate in public. Pe de altă parte, dansurile “antikristoi” pentru femei nu au fost însoţite de astfel de instrumente idiophone (zornăitoare, linguri, “zilia”), deoarece ar fi extrem de nepotrivit pentru o femeie sa danseze in public tinand aceste instrumente (Tyrovola, 1992; Lambropoulos, 1994). In locul lor de origine, Kappadokia, aceste dansuri au fost însoţite de cântece în dialectul de Farassa precum şi în limba turcă, în timp ce sărbătorile Farassian au fost un punct de atracţie pentru armeni, turci, greci convertiti şi cripto-creştini din satele învecinate. Această multime au avut nevoie de oameni au avut nevoie de mijloace comune de comunicare pentru divertisment, un rol îndeplinit de un cântec şi, în principal,de limba cântecului (Lambropoulos, 1994). Dansurile “kousokka” şi “i paigni mo ta houliere” sunt dansuri “antikristoi”cu o măsură de patru batai. “Ta kousokka” (sau “skafidakia”, care înseamnă “găuri mici”) este un dans “antikristos”femeiesc şi îşi datorează numele gaurii ovale care se formează atunci când vârful degetului mare atinge varful degetului arătător (Lambropoulos , 1994) sau atunci când capetele celor trei prime degete vin în contact. “I paigni mo ta houliere” este un dans“antikristos” barbatesc şi numele său înseamnă “dans cu linguri”. În ciuda faptului că aceste dansuri nu sunt denumite în continuare “tsift (e) teli” de către localnici, analiza lor structural-morfologica le clasifică, în funcţie de componentele lor tehnice, în această categorie. Este o practică destul de comună în zonele de coastă din Asia Mică, precum şi în partea continentală (Kappadokia) pentru dansatori să acompanieze dansurile“antikristoi” cu instrumente idiophone, cum ar fi linguri de lemn, “zilia’, pahare de vin, etc cu care menţin ritmul de dans. Dar, în timp ce în zonele de coastă această practică este observata atât la dansurile de femei cat si de barbate atat în cazuri de dans publice cat şi private, în regiunea vorbitoare de limbă greacă din Kappadokia, este văzuta în exclusivitate în rândul bărbaţilor. 2.1. Observaţii Din analiza structural-morfologica a dansurilor de mai sus, se observă că ambele dansuri(“ta kousokka” şi” I paigni mo ta houliere”),sunt dansuri “antikristoi” caracterizate prin folosirea libera a spaţiului şi a structurii coregrafice. Cu toate acestea, femeile au mai puţină libertate de improvizatie, cu variatii mici pe expresia de bază a dansului. Femeile efectueaza miscari mici, simple ale membrelor inferioare în timp ce isi sprijina greutatea corporală pe întreaga suprafaţă a tălpii. Mâinile sunt la nivelul fetei, ca si cum ar incerca sa o ascunda, si executa miscari semi-circulare într-un mod relativ liber, în timp ce primele două sau trei degete sunt în mod constant în contact la varfuri(fara degetul care plesneste). Trunchiul este drept şi nu efectuează nici un fel de miscare de unduire sau balansar. Modul de executare a acestui dans, cu mişcări neelaborate şi reţinute, reflectă introvertire, smerenie şi implică ruşine. Dimpotrivă, dansul barbatilor prezinta un grad mai mare de improvizaţie cu excentricitati caracteristice în timpul spectacolului de dans, cum ar fi unduirea trunchiului şi şoldurilor în timp ce sunt în poziţie semi-ghemuit. Barbatii sunt liberi să mişte partea superioară a corpului,sa se îndoaie şi sa se arcuiasca de la talie cum vor, şi chiar sa isi roteasca soldurile. Mâinile lor se misca libere, deschise la fiecare parte, cu mişcări circulare caracteristică în timp ce tin în acelaşi timp, ritmul de dans utilizand o pereche de linguri

26
(“houliere”), stabilind astfel o identitate dubla de dansator-muzician. Atunci când nu ţin linguri, barbatii danseaza tinand (“zilia”) sau zornăie sau isi pocnesc doar degetele . Dansul lor este mult mai rapid decât cel al femeilor şi mai energic, rezultand din mişcări de picior mai scurte si mai abrupte. Foarte adesea, picioarele bat ritmul pe pamant. Acest mod de dans cu o execuţie plina de viaţă , cu mişcări puternice şi viguroase, reflectă extrovertire şi scoate în evidenţă poziţia dominantă a bărbaţilor asupra femeilor. 3. Discuţii – Concluzii Analiza formei a arătat diferenţele dintre cele două dansuri în ceea ce priveşte elementele lor morfo-sintactice, precum si functia lor şi conţinutul semantic. Dansul “I paigni mo ta houliere” o forma de tsift (e) teli, în contextul cultural al Farassa, apare ca o practică de dans public exclusiv pentru bărbaţi. Dansul “Kousokka” de asemenea, o formă de tsift (e) teli, dar cu semiologie diferite, îşi asumă identitatea unei practice de dans privat al femeilor, care are loc în limitele casei. O practică similară, cu semiologie diferita, dar limitata la graniţele unui spaţiu privat, poate fi întâlnita în haremuri ale domnilor bogaţi şi ale ofiţerilor din Est, unde femeile vor putea realiza “dansul din buric”, din datoria de a distra bărbaţii. În comunitatea din Farassa, la fel ca în orice tip de societate, sexul, şi acţiunile sau funcţiile care derivă din acesta, organizează relaţiile sociale ale grupului şi întăreşte şi “legitimeaza”ierarhia acestor relaţii. Prin urmare, sexul organizează grupuri sociale de bărbaţi şi femei, stabileşte limitele precum şi regulile de comunicare între ele, şi determină conţinutul relaţiei lor (Strathern, 1976). Ierarhia naturala a sexelor ca un criteriu prin care valorile stabileşte relaţii organizeaza comunitatea din Farassa ca un exemplu de societate patriarhala, în care punctele de pivot de referinţă sunt religia, căsătoria şi înrudira (cu accent puternic pe relaţiile pe partea tatălui ), şi în care barbatul deţine centrul simbolic. Astfel, femeile apar obiecte slabe şi pasive în acest sistem social special, în timp ce bărbaţii sunt forta conducatoare primara si factorii decizionali. Acest tip de comportament stabileşte “capacitatea de dominare” a bărbaţilor asupra femeilor. În acest context, feminitatea este o datorie care trebuie să fie controlata de nimeni altul decât de femeie prin suprimarea de sine (a se vedea Papataxiarchis, 1992). Puritatea, modestia şi rezervarea reda femeii “ timiditatea” şi, astfel, sunt asociate cu ideea de timiditate într-o tendinta ascunsa. Puritate, ca atitudine şi poziţie, este adecvata pentru “femeile morale” - femeile care adoptă abtinerea, astfel încât să contribuie la apărarea onoarei familiei, în care, desigur, ele joacă un rol secundar, deoarece rolul primordial aparţine barbatilor. În concluzie, în contextul comunităţii creştine, monogamă şi patriarhala din Farassa, dansul “I paigni mo ta houliere”, o forma de tsift (e)-teli, cu utilizarea unor instrumente muzicale idiophone, a fost identificatcu dominaţia barbatilor. Ar fi foarte nepotrivit pentru o femeie sa practice acest dans tinand linguri şi agitand umerii,unduindu-si trunchiul sau soldurile. Traditiile stricte nu ar permite nici măcar să se pocneasca degetele. Cu toate acestea, cu trecerea timpului, noile structuri sociale, care au stabilit relaţia dintre cele două sexe pe o bază diferită şi au revendicat pentru femei o “egalitate instituţionala” neoficiala dar generalizata, a permis treptat, participarea femeilor la dans, utilizarea instrumentelor muzicale idiophone , iniţial pornind de la cercul retras al familiei şi întotdeauna în interior progresand practicarea în public, cum ar fi în piaţa satului. Cu toate acestea, chiar şi astăzi în ciuda repertoriului de dans, populaţia din Farassa, bărbaţi şi femei, continua sa participe la dans în perechi strict masculine sau feminine. Prin urmare, sexele organizeaza societatea din Farassa şi se permite continuarea elementelor care evidenţiază particularităţile sociale ale fiecărui sex şi ale grupurilor sociale corespunzătoare - elemente care sunt reflectate în formele de dans şi in participarea celor două sexe în dansurile menţionate anterior.

27
TABELUL I: Tabelul pentru intelegerea si compararea elementelor de forma ale dansului”TSIFT (E)-TELI” din FARASSA, KAPPADOKIA Zona Farassa, sau Varasos, Kappadokia Numele de dans
“ta kousokka” “I paigni mo ta houliere”
Dansatori Perechi de femei Perechi de barbati Utilizarea de spaţiu
Dansul“antikristos “ • folosirea libera a spaţiului (poziţii de tranzacţionare - revoluţii complete în jurul axei corpului
dansul“antikristos” • folosirea libera a spaţiului (poziţii de tranzacţionare - revoluţii complete în jurul axei corpului
Coregrafie Structura coregrafiei libere Structura coregrafiei libere model de formular / model
Bazat pe improvizatii relative bazate pe mici variaţii ale expresiei dansului de bază
improvizatii bazate pe modificări diverse ale expresiei dansului de baza
Elemente acustice
• acompaniament instrumental cu liră (kemane), tamboura-mpoulgari (instrumente cu coarde), daire (defi) • melodii în dialect de Farassa (din vremuri stravechi) sau în turcă
• acompaniament instrumental cu liră (kemane), tamboura-mpoulgari (instrumente cu coarde), daire (defi) • melodii în dialect de Farassa (din vremuri stravechi) sau în turca. instrumente muzicale idiophone (linguri, zilia, zornăitori)
Ritm 4/4 (♩.♪♩♩) or (♩.♪ ♫ ♫ ) 2/4 or 4/4 (♩. ♩ ♫) or (♩.♪♩♩) Tempo lent - mediu şi de echilibru mediu - rapid Motivul dansului
a. Expresia dansului de baza: [T 1(δ
1/4+α1/4+δ1/4+α1/4)]
b. Heteromorphy: [T 1(δ
1/4+α1/4+δ1/4+(δ)α11/4) +
T 2(α1/4+δ1/4+α1/4+(α)δ1
1/4)]
c.Improvizaţie (limitat)
a. Expresia dansului de baza [Ŧ 1(δ
1/8+α1/8+δ1/8+α1/8)]
b. Heteromorphy: [Ŧ 1(δ
1/8+α1/8+δ1/8+(δ)α11/8) +
Ŧ 2(α1/8+δ1/8+α1/8+(α)δ1
1/8)]
c.Improvizaţie membrele inferioare
• mişcărilentei, simple şi taraite • intinderea piciorului (drept de obicei) • greutate corporală susţinută de toata talpa piciorului Ridicari lente ale membrelor
• miscare libera cu intoarceri caracteristice • lovirea ritmica a lingurilor
Membrele superioare
• mişcări semi-circulare limitate la nivelul capului (ca în cazul în care l-ai ascunde), cu primele 2-3 degete care ating varfurile[formând un orificiu oval (skafida, sau kousokka)]
• miscare libera cu intoarceri caracteristice • lovirea ritmica a lingurilor
Trunchi • mişcări transversale neelaborate • mişcări transversale • unduirea / agitarea trunchiului superior (de foarte multe ori cu pauză de mişcare simultană a membrelor inferioare în poziţie ghemuit-jumătate) • îndoire la talie
Interpretare • mişcări simple restranse care implica modestie şi moralitate • atenţie la detalii • coordonarea miscarilor membrelor inferioare şi superioare • miscare alternativa
•miscari relative restranse cu ridicari scurte improvizate(fara exagerari) in timpul executarii dansului . • atenţie la detalii • coordonarea mişcărilor membrelor inferioare şi superioare • miscare alternativa
DANCE AND GENDER IDENTITY THE TSIFT(E)-TELI DANCE IN FARASSA, KAPPADOKIA
Hariton A. Haritonidis1, Vasiliki K. Tyrovola1
1Department of Physical Education and Sport Science, Kapodistrian University of Athens 1. Introduction The tsift(e)-teli dance is an integral element of the modern Greek dance reality as, with its instantly recognizable and uplifting rhythm, it constitutes an essential component of

28
contemporary Greek entertainment (Raftis, 1996). Although the tsift(e)teli dance (double-chord) today appears as being of neuter gender, practically it is, beyond doubt, of female gender. Tsift(e)-teli belongs to the special category of dances (Bucheld, 1996) in which certain movements prevail, such as those of upper body swaying or slinking, wavelike motions of the torso, arching of the body while simultaneously reversing the hands (Bucheld, 1996, and Tyrovola, 2002). Many terms have been used to describe this dance, which are derived either from its history, origins and symbolic properties, such as ‘belly dance’, ‘oriental’, ‘Salomi’s dance’, ‘harem dance’, ‘horos ton epta peplon’ or from its manner of execution or its notional content, such as ‘sensational’, ‘ecstatic’, ‘hieratic’, ‘hip dance’, ‘fertility dance’ (Petrides, 1976; Buchheld, 1996; Raftis, 1996; Tyrovola, 1999, 2002). From the above, it could be concluded at a first glance that, despite its many names, the tsift(e)-teli dance concerns basically a certain kind of popular-traditional dance associated with fertility, which in the course of its history spawned various hybrids and was included in the musical and dance repertoire of urban tradition (Tyrovola, 2002), or was seen through the criteria of folklore and artistic dance (Shay & Sellers-Young, 2005). Additionally, reports from early post-Christian times (Suchs, 1963) as well as numerous illustrations confirm the immediate connection of this dance, and its various sub-forms, exclusively with the female sex, as «…the bouncing movement of the breast, the rocking of the hips and the bending of the torso and waist obtain meaning exclusively when employed in order to arouse and excite the male…» (Tyrovola, 2002: 46-47). It could be concluded with relative certainty that the various forms of the tsift(e)teli dance have their origins in the common ethnological legacy of the people of the Mediterranean and Near East, while the first reports with the specific name date from the period of the development of urban centres in the Ottoman Empire (Tyrovola, 2002). Reports of the tsift(e)-teli dance have come from Greece, and in particular from islands of the northeastern Aegean such as Chios (Tyrovola, 2002) and Lesbos (Tyrovola, 2010), from the Macedonian region such as Irakleia, Serres (Papakostas, 2007), but also from regions such as the mainland of Minor Asia as well as from the musical and dance tradition of non-Christian Turkish-speaking and orthodox Greek-speaking populations of Kappadokia, such as the area of Farassa, or Misti and others. Interestingly, although according to common Western perception the tsift(e)-teli is representative of an exclusively female dance, in the traditions of the East, the dance is a matter of both men and women, the only distinction lying in whether it is danced in public (men) or in private (women) as well as in the form of the dance. A similar situation can be observed in the orthodox Greek-speaking community of Farassa, where the tsift(e)-teli concerns both sexes and reflects the social organization of the particular community as it highlights the gender-related relationships among the community members through its dance movements. From the review of relevant literature, it is clear that most of the information concerning dance examples of the tsift(e)-teli is ethnographic or folklore-descriptive (Margariti, 1987 and Lambropoulos, 1994). Research which is an exception to this includes the work of: Tyrovola (1992), in which the dance tradition of the Greeks of Kappadokia is presented through the use of ethnographic data as well as with reference to rhythms; Kotsia & Charitonidis (1998), which uses a structural-morphological analysis to document the tsift(e)teli of the Kappadokian Greeks as a special dance category which included various forms of the basic dance (hetero-morphies); and Tyrovola (2002), who investigates the problems arising between popular culture and social development, using the example of tsift(e)-teli dance. From the above, it is clear that there is an absence of studies approaching the tsift(e)-teli dance as a means of managing and highlighting the gender-related identity through analysis of its structure and form.

29
1.2. Aim The aim of this study is the investigation of the forms of the "ta kousokka" and "i paigni mo ta houliere" dances from Farassa of Kappadokia, as regional variations of the tsift(e)-teli dance and as used by each sex. In particular, the present study aims at highlighting the gender relationships in the context of the traditional society of Farassa by utilising the dance form as a tool for the analysis of the structure and form of the aforementioned dances, the latter being representative of each sex. 1.3. Methodology Data was collected using the ethnographic method based on primary and secondary sources (Buckland, 1999; Giurchesku 1999; Koutsouba, 1999; Tyrovola, 2008). The primary sources concern data collected through field research in the form of interview (Thompson, 2002) and participative observation (Gefou-Madianou, 1999; Lydaki, 2001; Petronoti, 2002). In particular, the field research was conducted in February 1987 (preliminary) and was completed in May 2003, and constitutes part of a wider research on the cultural identity of Kappadokian refugees. The research focused on the community of Plati of Imathia, Macedonia, inhabited mainly by refugees from Farassa, Kappadokia. The secondary sources concern data collected through ethnographic research (Stocking, 1983; Gefou-Madianou, 1999; Tyrovola, 2008). The structural-morphological and typological analysis as applied in Ethnochoreology (Tyrovola, 1994, 2001; Tyrovola, 2008) was used for the analysis of the dance forms, while the comparative method was used for the comparison of dance forms (Holt & Turner, 1972; Vallier, 1973²; Tyrovola, 2008). For the interpretation of the data, anthropological thought on the gender identity was used, as it appears in anthropological views of dance and particularly in Hanna (1987, 1988). This is a theoretical model which views the perception of sex as a field of negotiation, cultural symbol or social relationship (Strathern, 1976, 1988; Papataxiarchis, 1992), as well as a criterion for the analysis of the local population (Papataxiarchis, 1992). 2. Data Analysis Farassa, or Varassos (Greek name that is used in the area since ancient times), is a major town with Greek population (Loukopoulos & Petropoulos, 1949; Merlier, 1974; Tyrovola, 1990; Kikisoglou, 1997) in south-eastern Kappadokia, among gorges and Turkish villages and at an altitude of 1050 metres. According to Merlier, «…in 1923, the Greeks of Kappadokia (…) arrived in Greece abandoning their homeland for good…»(1974:30). The refugees from Farassa settled on the fringes of urban centres in central Macedonia and Thessalia, but the majority settled in the region of Katerini (Plati, Imathia). The dance tradition of the population of Farassa includes circle and ‘antikristoi’ dances (Lambropoulos, 1994:79), which are performed at four-beat and nine-beat rhythms (Tyrovola, 1996)1. The nine-beat ‘antikristoi’ dances (‘zeibekiko’ with knives) are danced exclusively by men, while the four-beat ‘antikristoi’ dances are distinguished in all-male and all-female, since rarely would a man dance with a woman – and that, only if they were close relatives. The four-beat ‘antikristoi’ dances are characterized by the accompaniment of idiophone instruments, such as ‘rattles’ or spoons, held by the dancers and are danced in public. On the other hand, the female ‘antikristoi’ dances were never accompanied by such idiophone instruments (rattles, spoons, ‘zilia’) as it would be enormously inappropriate for a woman to dance in public holding these instruments (Tyrovola, 1992; Lambropoulos, 1994).
1‘Antikristos’ in Greek means ‘opposite the other’. The term ‘antikristoi’ for dances, freely translated, means that the participants perform the dance facing each other.

30
In their place of origin, Kappadokia, these dances were accompanied by songs in the dialect of Farassa as well as in Turkish, while the Farassian celebrations were an attraction for Armenians, Turks, converted Greeks and crypto-Christians from neighbouring villages. This gathering of people required a common means of communication in entertainment, a role fulfilled by the song and, mainly, the song language (Lambropoulos, 1994). The dances "ta kousokka" and "i paigni mo ta houliere" are ‘antikristoi’ dances with a four-beat measure. "Ta kousokka" (or ‘skafidakia’, which means ‘little holes’) is a female ‘antikristos’ dance and owes its name to the oval hole that is formed when the tip of the thumb touches the tip of the index finger (Lambropoulos, 1994) or when the tips of the three first fingers come in contact. "I paigni mo ta houliere" is a male ‘antikristos’ dance and its name means “the dance with the spoons”. Despite the fact that these dances are not referred to as ‘tsift(e)teli’ by the locals, their structural-morphological analysis classifies them, according to their technical components, in this category. It is quite a common practice in the coastal areas of Minor Asia as well as in the mainland (Kappadokia) for the dancers to accompany the ‘antikristoi’ dances with idiophone instruments such as wooden spoons, ‘zilia’, wine glasses, etc. with which they maintain dance rhythm. But while in the coastal areas this practice is observed in both male and female dances, both in private and public dancing instances, in the Greek-speaking region of Kappadokia, it is exclusively seen among men. 2.1. Observations From the structural-morphological analysis of the above dances, it is observed that both ("ta kousokka" and "i paigni mo ta houliere") are ‘antikristoi’ dances characterized by free use of space and free choreographic structure. However, women have less improvisational freedom with little variations on the basic dance phrase. The women perform small, simple and shuffling movements of the lower limbs while supporting body weight on the whole area of the sole. The hands are at face level, as if in an attempt to obscure it, and execute semi-circular movements in a relatively free manner, while the two or three first fingers are constantly in contact at the tips (absence of finger snapping). The torso is straight and does not perform any sort of slinking or swaying movement. The manner of execution of this dance, with unelaborated and restrained movements, reflects introversion, humbleness and implies “shame”. On the contrary, the dance of men exhibits a greater degree of improvisation with characteristic peaks during the dance performance, such as slinking the torso and hips while in half-squat position. The men are free to move the upper body, bend and arch at the waist at will, and even rock the hips. Their hands move freely, open at each side with characteristic circular movements while simultaneously holding the dance rhythm pattern with the use of a pair of spoons (‘houliere’), thus establishing a dual identity of dancer-musician. When they do not hold spoons, the men dance holding ‘zilia’ or rattles or just snap their fingers. Their dance is more quickly-paced than that of the women and more vigorous, resulting in shorter and more abrupt leg movements. Very often, the feet stomp the rhythm on the ground. This manner of lively execution of the dance, with loud and vigorous movements, reflects extroversion and highlights the dominance of men over women. 3. Discussion - Conclusions Analysis of the form showed differences between the two dances in terms of their morpho-syntactic elements as well as their function and semantic content. The dance "i paigni mo ta houliere", a form of tsift(e)teli, within the cultural context of Farassa, emerges as a public dance practice exclusive to men. The "kousokka" dance, also a form of tsift(e)teli but with different semiology, assumes the identity of a private dance practice of women that occurs within the boundaries of the home. A similar practice, with different semiology but confined to the boundaries of a private space, can be encountered in the harems of the wealthy lords

31
and officers of the East, where women would perform the ‘belly dance’ as a part of their duty to entertain the men. In the community of Farassa, just like in every kind of society, the sex, and the actions or functions that derive from it, organizes the social relationships of the group and strengthens and ‘legitimises’ the hierarchy of these relationships. Therefore, the sex organises the social groups of the ‘men’ and the ‘women’, establishes the boundaries as well as the communication rules between them, and determines the content of their relationship (Strathern, 1976). The ‘natural’ hierarchy of sexes as a criterion by which values organise relationships establishes the community of Farassa as an example of a patriarch society, in which pivotal points of reference are religion, marriage and kinship (with heavy emphasis on relations on the side of the father) and in which the man holds the symbolic centre. Thus, the women appear as weak and passive objects in this particular social system while the men are the primary driving force and decision makers. This type of behaviour establishes the ‘dominating ability’ of men over women. In this context, femininity is a ‘liability’ which must be controlled by no other than the woman by suppressing her self (see Papataxiarchis, 1992). Purity, modesty and reserve render the woman ‘shy’ and, thus, are associated with the idea of ‘shyness’ in an undercurrent way. Purity, as an attitude and stance, is appropriate for “moral women” - the women who adopt self-restraint so as to contribute to the protection of family honour, in which, of course, they play a secondary role since the primary role belongs to men. In conclusion, in the context of the Christian, monogamous and patriarch community of Farassa, the dance "i paigni mo ta houliere", a form of tsift(e)-teli, with the use of idiophone musical instruments, was identified with the dominance of men. It would be greatly inappropriate for a woman to perform this dance holding spoons and shaking her shoulders, torso or hips. The strict customs would not even allow snapping her fingers. However, with the passing of time, the new social structures, which established the relationship of the two sexes on a different basis and had the women claiming an unofficial but generalized ‘institutional equality’, gradually allowed the woman’s participation in dance using idiophone musical instruments, initially starting from the secluded family circle and always indoors and progressing to performing in public, such as in the village square. However, even today and despite the crossover of dance repertoire, the population of Farassa, men and women, persist in participating in dance in strictly male or female pairs. Therefore, the sexes organise the society of Farassa and condone the continuation of the elements that highlight the social particularities of each sex and the corresponding social group - elements which are reflected in the dance forms and the participation of the two sexes in the aforementioned dances.
Table 1: comprehensive and comparative table of the form elements of the ‘tsift(e)-teli’ dance of farassa, kappadokia
Area Farassa, or Varasos, Kappadokia Name of dance "ta kousokka" "i paigni mo ta houliere" Dancers Pair of women Pair of men Use of space • ‘antikristos’ dance
• free use of space (trading positions – full revolutions around body axis
• ‘antikristos’ dance • free use of space (trading positions – full revolutions around body axis
Choreography Free choreographic structure Free choreographic structure Form pattern/model
Relative improvisation based on small variations of the basic dance phrase
improvisation based on various alterations the basic dance phrase
Acoustic elements
• instrumental accompaniment with lyre (‘kemane’), tamboura-mpoulgari (stringed instruments), daire (defi) •songs in the dialect of Farassa (earlier times) or in Turkish
• instrumental accompaniment with lyre (‘kemane’), tamboura-mpoulgari (stringed instruments), daire (defi) •songs in the dialect of Farassa (earlier times)

32
or in Turkish • idiophone musical instruments (spoons, ‘zilia’, rattles)
Rhythm 4/4 (�.♪��) or (�.♪ ♫ ♫ ) 2/4 or 4/4 (�. � ♫) or (�.♪��) Tempo slow – medium and steady medium – fast Dance motif a. Basic dance phrase:
[T 1(δ1/4+α1/4+δ1/4+α1/4)]
b. Heteromorphy:
[T 1(δ1/4+α1/4+δ1/4+(δ)α1
1/4) +
T 2(α1/4+δ1/4+α1/4+(α)δ1
1/4)]
c. Improvisation (limited)
a. Basic dance phrase:
[Ŧ 1(δ1/8+α1/8+δ1/8+α1/8)]
b. Heteromorphy:
[Ŧ 1(δ1/8+α1/8+δ1/8+(δ)α1
1/8) +
Ŧ 2(α1/8+δ1/8+α1/8+(α)δ1
1/8)]
c. Improvisation
Lower limbs • small, simple and shuffling movements • extension of the right (usually) foot • body weight supported by whole area of the sole of the foot • low leg lifts
• small, abrupt movements • frequent stomping of the rhythm on the ground • extension of the right (usually) foot • body weight supported by whole area of the sole of the foot • low leg lifts • pauses
Upper limbs • limited semi-circular movements at head level (as if in an attempt to hide it) with the 2 or 3 first fingers touching at the tips [forming an oval hole (‘skafida’, or ‘kousokka’)]
• free movement with characteristic turns • rhythmic striking of spoons
Torso • unelaborated transverse movements • transverse movements • slinking/shaking of the upper torso (very often with simultaneous pause of movement of lower limbs in half-squat position) • bending at the waist
Interpretation • simple, restrained movements implying modesty and morality • attention to details • coordination of upper and lower limb movements • alternating movement
• relatively restrained movements with short improvisational peaks (without exaggerations) during the dance performance • attention to details • coordination of upper and lower limb movements • alternating movement
Selective Bibliography 1. Buckland, Th. (Ed). (1999). Dance in the Field. Theory, Methods and Issues in Dance Ethnography, Macmillan Press, Great Britain. 2. Gefou-Madianou, D. (1999). Πολιτισµός και Εθνογραφία (Culture and Etnography). Αthens: Hellinika Grammata. 3. Giurchesku, A. (1999). "Past and Present in Field Research: A Critical History of Personal Experience". In T. J. Buckland (Εd.), Dance in the Field. (σσ. 41-54). London: Macmillan Ltd. 4.Hanna, J. (1988). Dance, Sex and Gender. Chicago: The University of Chicago Press. 5. Holt, T. R. & Turner, E. J. (Eds). (1972). The Methodology of Comparative Research.
New York: The Free Press.

33
Judo, comunicare şi lucru în echipă
Conf dr. ION ENE MIRCEA Cuvinte cheie: încredere, interdependenţă, responsabilitate, maturitate, echipă.
Rezumat: Comunicarea prin intermediul sportului oferă şansa stăpânirii unui limbaj specific, de
cunoaştere şi autocunoaştere, de evaluare, perfecţionare, de susţinere a speranţelor, a proiectelor, a valorificării experienţelor sportive în viaţa cotidiană. Ea ne dă şansa formării conştiinţei de sine, a numelui şi renumelului, a respectului, a demnităţii, a recunoaşterii valorii. În anumite condiţii asigură orientarea profesională şi permite transferul achiziţiilor comunicării şi colaborarii în acest plan.
Comunicarea prin sport îşi poate aduce contribuţia pe toată durata vieţii în influenţarea pozitivă a tuturor categoriilor de cetăţeni. Prin regulamente, disciplină, tipologie, ramurile sportive asigură nivele şi direcţii diferite de integrare.
Sporturile individuale ne apropie, prin obiective de cerinţele “Eu-ului” personal, în timp ce sporturile de echipă, ne asigură modele psiho-adaptative integrative relaţionale legate de: respect, asigurare, ajutor, responsabilitate faţă de sine şi faţă de grup, colaborare, interacţiune, sinergie acţională, etc.
Rigorile fiecărui sport impun valenţe educative, etice, estetice, artistice, culturale specifice.
În acest context remarcăm poziţionarea judo-ului ca disciplina în care competiţiile sunt organizate atât individual cât şi pe echipe, practicanţii beneficiind de ambele direcţii de integrare. Comunicarea prin sport este valorificată din ce în ce mai mult şi la nivelul relaţional. Site-urile, forum-urile de pe Internet, grupează pe zone de interes un număr din ce în ce mai mare de persoane ce doresc să beneficieze de efectele socio-integrative ale sportului.
Se dau şi se primesc sfaturi de la mii de km., se ţin lecţii on-line. În jurul fenomenului sportiv se întăresc alianţe şi prietenii între persoane de diverse naţionalităţi. Comunicarea prin sport formează conduite, amplifică procesul cunoaşterii, mediază răspândirea mesajelor valoroase cum ar fi cele ale mişcării Olimpice şi nu numai. Ea oferă soluţii alternative de manifestare psiho-comportamentală pentru situaţii diferite de prietenie, colaborare sau adversitate. Comunicarea prin sport oferă dimensiunea unor concepte, stări, soluţii, acţiuni ce pot fi adaptate: luptă, fair-play, măiestrie, antrenament, sacrificiu, câştig, adversar, echipă, colaborare, muncă, dăruire, perseverenţă, voinţă, eroism, altruism etc. Comunicarea prin sport amplifică realităţile spiritului sportiv: ”suntem adversari, suntem luptători, cunoaştem preţul victoriei şi al înfrângerii, învăţăm să pierdem şi să câştigăm, suntem corecţi, respectăm adversarul, arbitrii şi pe noi înşine”. Atuuri ale comunicării şi colaborării în echipa sportivă şi la locul de muncă
Beneficiari la nivel formativ ai comunicării prin sport sunt toţi cei aflaţi în contact cu fluxul informaţional: sportivi, antrenori, arbitrii, specialişti, oficiali, organizatori, comentatori, ziarişti, spectatori, cititori, oameni de diferite vârste, profesii sau categorii sociale. Comunicarea prin intermediul sportului oferă şansa stăpânirii unui limbaj specific, de cunoaştere şi autocunoaştere, de evaluare, perfecţionare, de susţinere a speranţelor, a proiectelor, a valorificării experienţelor sportive în viaţa cotidiană. Ea ne dă şansa formării

34
conştiinţei de sine, a numelui şi renumelului, a respectului, a demnităţii, a recunoaşterii valorii. În anumite condiţii asigură orientarea profesională şi permite transferul achiziţiilor comunicării şi colaborarii în acest plan.
S-au scris multe despre LUCRUL IN ECHIPA, activitate în care se regăsesc oameni lucrând cu bucurie împreună şi având drept rezultat o productivitate sporită, spre binele firmei şi al lor. Tot ceea ce le trebuie: un anumit nivel de instruire şi educaţie, un set de exerciţii de sudare a colectivului, un scop comun şi o serie de obiective.
Nu-i putem alege pe cei cu care lucrăm zilnic. Şi – să recunoaştem – cele mai multe locuri de muncă sunt departe de a fi lipsite de animozităţi între angajaţi. Prin urmare, cum poţi încuraja încrederea într-un cadru în care nu tu ai ales participanţii, iar nivelul stresului este ridicat? Comunicare, maturitate, responsabilitate reciprocă, interdependenţă, controlul stării conflictuale, încredere în capacitatea de a depăşi obstacolele, asumarea riscurilor şi implicare, sunt posibile răspunsuri la aceasta întrebare. Comunicarea – piatra de temelie a oricărei acţiuni reuşite, incluzând alcătuirea unei echipe şi încredere între membrii acesteia. Deşi este uşor să recunoşti o comunicare sinceră, deschisă, e greu să o implementezi. într-o echipă, fiecare ar trebui încurajat să vorbească deschis – într-un mod constructiv – şi fără să-i atace sau denigreze pe colegi, deoarece fiecare vine cu propriul său stil de a comunica. Iarăşi, un lucru important este stabilirea unor reguli ca: „Nimic nu iese din camera asta, în afară de cele stabilite de comun acord şi care nu sunt tabu”. Încrederea va creşte mai repede dacă fiecare simte că echipa este un forum pentru a-şi dezvolta ideile şi o fereastră pentru a vedea gândurile celorlalţi. Încrederea în capacitatea de a depăşi obstacolele – această credinţă sau atitudine pozitivă este crucială pentru succesul unei echipe. Adesea, echipele se formează tocmai pentru a depăşi obstacole şi a rezolva probleme. Trebuie să existe o încredere reciprocă în cadrul colectivului. Cine nu crede în noţiunea de echipă va declanşa o stare negativă în ceilalţi, care va irosi timpul şi energia echipei. Mai ales dacă i se pare că ea este o pierdere de vreme şi că nu va merge-n veci.
Maturitatea – este cheia încrederii care se clădeşte odată cu echipa. Cel care aparţine unei echipe trebuie să fie suficient de matur pentru a lua în considerare o părere sau o personalitate, în funcţie de cum aceasta afectează colectivul; nu doar cum l-ar atinge pe fiecare. Maturii sunt capabili şi să discearnă părerea echipei faţă de una dintre ideile lor, în paralel cu opinia echipei faţă de ei personal. De asemenea, îşi pot menţine părerea bună despre sine chiar când ceilalţi sunt în dezacord cu ei şi nici nu devin isterici, părându-li-se că echipa vrea „să-i termine”. Responsabilitatea reciprocă – nu este un lucru pe care am fost obişnuiţi să-l acceptăm la locul de muncă. Pornind de pe băncile şcolii şi trecând prin mai multe locuri de muncă, am fost recompensaţi pentru performanţele personale, şi nu pentru realizările grupului. Multor oameni le este greu să recunoască faptul că reuşita şi avansarea lor sunt – fie şi parţial – meritul celorlalţi. Adesea, unii nu cred că şi colegii lor fac o muncă serioasă ori de calitate. Interdependenţa – o altă trăsătură care nu se găseşte „de-a gata” în societatea noastră (cu excepţia familiei, în unele cazuri). Suntem învăţaţi să ne ferim de „Number One” şi să nu fim surprinşi când alţii ne lasă de izbelişte. Totuşi, studiile au arătat că două (sau trei, sau patru, sau cinci) capete sunt mai bune decât unul singur . Interdependenţa este extrem de importantă pentru bunul mers al unei echipe, fiindcă nici un membru al ei nu valorează cât întreaga echipă. Controlul stării conflictuale – din păcate, prea des totul se preschimbă într-o încercare de evitare. Membrii unei echipe îşi dau seama că este cu mult mai bine să se ocupe din vreme de un conflict, atunci când stă să izbucnească, decât să-l lase să se „umfle” odată cu

35
trecerea timpului. Puţinul disconfort care este resimţit acum este minor faţă de o izbucnire de mai târziu. Încrederea nu poate „înflori” într-o atmosferă ostilă. Într-o echipă, fiecare membru vine cu un stil diferit de a controla starea conflictuală. Este foarte important să se stabilească nişte reguli de bază pentru grup şi cel mai important lucru va fi să se ţină sub control toate disputele într-un mod cât se poate de prompt. De fapt, lipsa unui acord de păreri este o componentă naturală şi sănătoasă a procesului de constituire a echipei, dacă este controlată aşa cum se cuvine. Asumarea riscurilor ca afinitate – e în strânsă legătură cu cele de până acum. Toate noţiunile discutate anterior implică şi asumarea unui risc oarecare. Oamenii se pot împotrivi celor care riscă, fie prin natura lor, fie datorită unor experienţe trecute. Pentru unii, asumarea riscurilor este dificilă, existând teama să nu le fie furate ideile. Succesul şi bunul mers al unei echipe constă în obişnuinţa fiecărui membru de a-şi asuma un anume risc, pentru a lăsa loc încrederii să se dezvolte. Implicarea – preocuparea pentru alcătuirea unei echipe este la îndemâna oricui şi este necesară la consolidarea încrederii. Dacă lipseşte măcar un singur „fir”, „mănunchiul” va avea de suferit. Toţi trebuie să fie încredinţaţi că vin la lucru gata pregătiţi şi concentraţi asupra problemelor de rezolvat.
În sfârşit, adevăraţii lideri de echipă vor acorda mai multă atenţie faptelor şi mai puţină spuselor. Nu poţi clădi încredere şi bună reputaţie numai pe planuri .
Sa nu uitam ca la baza structurării şi consolidării unei echipe stau respectul, onestitatea, politeţea, seriozitatea, prietenia, curajul, autocontrol, modestia, sinceritatea, întrajutorarea, într-un cuvânt CODUL MORAL, atât de apreciat de practicanţii artelor marţiale, a judo-ului în mod deosebit.
Bibliografie selectivă: 1. Cucos, Ctin., (coord.), 1998, Psihopedagogie, Ed. Polirom, Iasi 2. Dave, R., H., 1991, ( în traducere), Fundamentele educatiei permanente, Ed..Didactica si Pedagogica, R. A., Bucuresti. 3. Delors, J., (coord.), 2000, (în traducere), Comoara launtrica, , Ed.. Polirom, Iasi 4. Mihailescu, L., 2008, Calitate în educatie - o abordare pragmatica, Caled 1, Ed.Universitatea din Pitesti 5.Vaideanu, G., 1988, Educatia la frontiera dintre milenii, Ed.Politica, Bucuresti 6. Vaideanu, G.,1996, UNESCO –50 Educatie, Ed.. Didactica si Pedagogica, R. A.,Bucuresti
Judo, communication and team working Key words: trust, interdependence, responsability, maturity, team.
Summary: Communication by sports offers the chance of having a specific language of knowing
and selfknowing valuation, improvement supporting hopes, projects, putting to good use of the sport experiences in the daily life. It gives us the chance of building the self conscience, of the name and fame, respect, dignity, knowing the real value. In certain conditions it guarantees the professional orientation and it allows the transfer of the communication acquisitions and of colaboration in this plan.

36
The communication by sports can contribute all life long to the positive influence of all the citizens categories. By rules, discipline, typology, the sports domains guarantee different levels and directions of integration.
The individual sports have such targets which help us to be near the personal “I” requirement, while the team sports guarantee patterns of psycho adaptation, of relations concerning: respect, help, self responsability, concerning the group, collaboration, interaction and so on.
The rigourousity of every sport asks for specific cultural, educative, ethical, artistic values.
So we see judo as the discipline with individual and group competitions where the players have both integration directions.
The communication by sports is turned to account more and more at the level of relations too.
The sites and forums on Internet present a great number of people who want to profit by the integrative-social effects of sports.
Pieces of advice are given and received from thousands of km, there are lessons on-line. Friendship among different nationalities is created by sports.
Sport communication contributes to a good behavior, amplifies the knowledge process, help people to participate to the Olympic Games and that is not all.
It offers alternative solutions of behavior manifestations for different friendship situations and partnership.
The sport communication offers the following concepts: states, solutions, adapted actions fight, fair-play, skillfulness, training, sacrifice, winning, opponent, team, collaboration, work, love for sports, tenacity will, heroism, altruism.
The sport communication amplifies the realities of the sportive spirit: “we are opponents, we are fighters, we learn to loose and to win, we are honest, we have respect for the opponent, the referee and for ourselves”. The trumps of communication and collaboration in the sport team and for the working place. Formative level of customer communication through sports are all those in contact with the flow of information: athletes, coaches, officials, experts, organizers, commentators, journalists, spectators, readers, people of different ages, professions and social categories.
Communication offers a chance domination through sport-specific language, knowledge and self-awareness, evaluation, improvement, supporting the hopes, the Projects, the capitalization of sports in everyday life experiences. It gives us a chance formation of self-consciousness of the name and fame, respect, the dignity, the recognition of the value. In certain circumstances provide guidance for transferring procurement professional communication and cooperation in this plan.
Have written a lot about team work, which included business people working together and having a happy result improved productivity for the good of the company and their own.
Everything they need: a certain level of training and education, a set of welding team exercises, a common purpose and a series of objectives.
We can not choose who work with daily. And recognize most of the jobs are far from being devoid of animosity among the employees. Therefore, how to encourage trust in a setting where you did not choose the participants, and the stress level is high?
Communication, maturity, mutual responsibility, interdependence, conflict state control, confidence in the ability to overcome obstacles, risk-taking and involvement, are possible answers to this question.
Communication – The ground team and trust among members. While it is easy to recognize an honest communication, opened it is difficult to implement it a team, everyone

37
would be encouraged to talk openly – in a constructive way – and without attacking or denigrate colleagues because each comes with its own style of communicating. Again, the important thing is to establish rules like ”nothing comes out of this room, except for those agrees and not taboo”. Confidence will grow faster if each feels the team is a forum to develop ideas and a window to see the others’thoughts..
Confidence in the ability to overcome obstacles – this belief or positive attitude is crucial to the success of a team. Often, teams are formed precisely to overcome obstacles and solve problems. There must be mutual trust in the team. Who does not believe in the notion of team will trigger a negative feeling it is a waste of time and it will not work forever.
Maturity – is a key that builds trust with the team. One who belongs to a team must be mature enough to consider an idea or personality, depending on how it affects the team, not just how it would touch everyone. Adults are able to discern from a team think opposite their ideas, along with the opinion of the team. Also, they can maintain their good opinion of themselves even when others disagree with them and not become hysterical, thinking that the team “wants to finish them”.
Mutual responsibility – not something we were accustomed to accept at work. Starting in school and going through several jobs, we were rewarded for our personal performances, and not for achievements group. Many people find it difficult to recognize that their success and promotion even partial – the others’ merit. Often people don’t think that their collegues do a serious work of quality.
Interdependency – another feature not found ready-made in our society (except the family, in some cases). We learned to stay away from number one and not be surprised when others abandon us. However, studies have shown that two (or three, or four, or five) heads are better that one. Interdependence is extremely important for the good of a team, because no member of it not worth the whole team.
The control of conflicting state – unfortunately, all too often is changed in an attempt to erupt when standing, than to let it swell over time. Which is now felt little discomfort is minor compared to a later outburst. Trust can not flourish is a hostile atmosphere. One team, each member brings a different style to control the state conflict. It is very important to keep under control all disputes in a timely manner as possible. In fact, no agreement of opinion is a natural and healthy part of the process of establishing the team, if controlled as properly.
Taking risks affinity – is in close touch with so far. All concepts discussed before involves some risk-taking. People may resist those who take risks, either by their nature or because of past experiences. For some, taking Risks is difficult, being afraid their ideas not to be stolen. The success and smooth running of a team consists of each member’s habit of assuming some risk, to leave room to develop confidence.
Involvement – concern for the composition of a team is available to everyone and it is necessary to strengthen confidence. If missing even one thread, “bunch” will suffer. We all need to be confident that we come to work ready and prepared to resolve problems.
Finally, the true leaders, will pay more attention to facts and less words. You can’t
only build trust and reputation but on the plans. Do not forget that the basis for structuring and consolidation of a team are
respect, honesty, politeness, seriousness, friendship, courage, self-control, modesty, sincerity, helping, in a word MORAL CODE, so appreciated by trainees of martial arts, judo in the particular.

38
STUDIU COMPARATIV PRIVIND CRE ŞTEREA ŞI DEZVOLTAREA FIZIC Ă A COPIILOR DE VÂRST Ă ŞCOLARĂ ATÂT DIN MEDIUL URBAN CÂT ŞI DIN
MEDIUL RURAL ÎN CORELA ŢIE CU FACTORII DE MEDIU ŞI SOCIO-ECONOMICI
Masterand Sîrbu Oana-Alexandra
FEFS Galaţi
Cuvinte cheie: creştere, dezvoltare fizică, copii de vârstă şcolară, factori de mediu, factori socio-economici. Rezumat: Creşterea şi dezvoltarea copiilor reprezintă una dintre problemele de biologie umană cu deosebită semnificaţie teoretică şi practică. Elementul esenţial care deosebeşte copilul de adult este tocmai acest proces complex al creşterii şi dezvoltării. Una din etapele importante ale dezvoltării organismului uman este adolescenţa care debutează în jurul vîrstei de 10 ani. Etapa pubertară (şcolar mijlociu) diferă pe sexe: 10 ani la fete (10 - 14 ani); 12 ani la băieţi (11 – 16 ani), etapă în care copilul creşte brusc, apoi creşterea încetineşte, toate segmentele corpului cresc concomitent, se dezvoltă musculatura şi creşte forţa fizică.
Introducere: Creşterea este un proces unic pentru fiecare copil, încadrându-se, în limite largi, în ceea ce se cheamă normalitate. Principalii indicatori de creştere sunt talia, greutatea, perimetrul cranian, dar se mai pot adăuga perimetrul toracic şi măsurătorile segmentare.
Dezvoltarea fizică a copiilor prezintă unul din cei mai importanţi indici ai sănătăţii organismului în creştere şi reprezintă totalitatea capacităţilor morfologice şi funcţionale ale organismului, care caracterizează procesul de creştere şi dezvoltare. În aprecierea creşterii se folosesc, de regulă, criterii cantitative: uşor, greu, mic, mare, scund, înalt. Dezvoltarea se apreciază folosind criteriile calitative. Se poate vorbi de o dezvoltare bună, rea, rapidă, lentă, timpurie, întârziată. Motiva ţia alegerii temei: Având în vedere faptul că în zona judeţului Galaţi nu există studii privind ritmul de creştere şi dezvoltare a copiilor de vârstă şcolară şi nici corelaţii privind modul în care factorii de mediu şi socio-economici influenţează creşterea şi dezvoltarea, considerăm necesară efectuarea unui studiu longitudinal care să urmărească ritmul de creştere şi dezvoltare fizică a copiilor de ciclu gimnazial în corelaţie cu factorii de mediu şi socio-economici. Scopul lucrării: Studiul de faţă reprezintă o etapă intermediară a unui studiu longitudinal ce se desfăşoară în decursul a 4 ani având ca obiectiv primar evaluarea factorilor ce influenţează ritmul de creştere şi dezvoltare a copiilor de vârstă şcolară. Aşadar, scopul lucrării de faţă este de evaluare a ritmului de creştere şi dezvoltare a copiilor de vârstă şcolară în corelaţie cu factorii de mediu, socio-economici şi cu nivelul de activitate fizică.
Ipoteza de lucru: Privind creşterea şi dezvoltarea sub aspect fizic a copiilor de vârstă şcolară, presupunem că factorii de mediu şi socio-economici pot influenţa pozitiv sau negativ aceste procese.

39
Materialul de studiu şi metode de cercetare folosite: Această lucrare se întemeiază pe studiul a 909 copii, toţi din judeţul Galaţi, cu vârste cuprinse între 10 şi 16 ani, dintre care 749 din mediul urban şi 160 din mediul rural (localităţile Băneasa şi Vârlezi). Acest studiu s-a bazat pe următoarele evaluării: - antropometrice:înălţime, greutate corporală, înălţime şezând, diametru biacromial, diametru bitrohanterian, diametru transvers-toracic, diametru toracic antero-posterior.
Pe baza datelor antropometrice s-a calculat indicele Quetelet (BMI sau IMC), fiind considerat de către OMS drept criteriu fundamental în evaluarea creşterii copiilor cu vârste cuprinse între 2-20 de ani. Pentru analiza evoluţiei indicelui Quetelet am recurs la metoda percentililor, metodă recomandată de către OMS.
De asemenea s-au efectuat evaluări în ceea ce priveşte nivelul de noxe atmosferice din zona de reşedinţă şi evaluarea nivelului de activitate fizică – indicele de activitate fizică (metoda chestionarului).
Prelucrarea statistică a rezultatelor s-a efectuat separat pentru fiecare din cele două loturi de subiecţi, în funcţie de sex şi categoria de vârstă, astfel:
Din figurile nr. 1 şi 2 se constată că aproximativ o treime din copiii studiaţi în această etapă nu sunt dezvoltaţi normal, fie ei subponerali (3,89%), supraponderali şi obezi (27,23%).
Stare ponderala Baieti2009-2010
normoponderali, 68.88
subponderali, 3.89 suprponderali&ob
ezi, 27.23
Figura nr. 1
Stare ponderala Fete2009-2010
subponderal, 4%supraponderal si
obezi 19%
normoponderal, 77%
s
Figura nr. 2

40
În ceea ce priveşte graficul nr. 1 constatăm că ponderea cea mai ridicată de fete/băieţi, obezi şi supraponderali o întâlnim în zonele periferice ale oraşului Galaţi iar cea mai scăzută în mediul rural.
0
5
10
15
20
25
30
35
1 2 3
centru periferie ru ral
Grafic comparativ stare ponderala fete/baieti pe zone 2009-2010
supraponderali&obezi fete
supraponderali&obezi baieti
Graficul nr. 1
Analizând graficul nr. 2 constatăm că fetele (20%) sunt mai sedentare decât băieţii (18%) în studiul realizat în perioada 2009-2010.
Graficul nr. 2
În urma desfăşurării acestei cercetări ştiin ţifice, din datele obţinute dorim să punctăm următoarele concluzii:
• Factorii care influenţează semnificativ ritmul creşterii şi dezvoltării sunt: vârsta, sexul, mediul (urban, rural) şi nivelul de activitate fizică. Mai mult de o treime din lotul studiat este sedentară şi foarte sedentară cu un procentaj mai ridicat la fete.
• Copiii studiaţi de noi cresc diferenţiat în decursul intervalul 10-16 ani şi îşi modifică succesiv proporţiile corporale, fenomene ce vor duce in final la realizarea conformaţiei dismorfice exprimate, în general prin dimensiuni mai mari la sexul masculin faţă de cel feminin.
• Datorită pubertăţii mai precoce, fetele între 12-14 ani sunt mai înalte decât băieţii, iar băieţii în această perioadă nu îşi realizează încă caracterele lor dismorfice.
0,0%
20,0%
40,0%
60,0%
masculin feminin
Grafic comparativ privind indicele de activitate în func ţie de sex
2009-2010
foarte sedentar sedentar activ foarte activ

41
Propuneri: În urma rezultatelor obţinute din studiul de faţă, punctăm anumite propuneri şi măsuri de combatere în acest sens:
• Promovarea utilizării în condiţii de siguranţă a transportului public şi mişcare activă- cum ar fi bicicleta sau mersul pe jos, ca alternative la folosirea vehiculelor personale – ar putea reduce emisiile de dioxid de carbon şi îmbunătăţirea sănătăţii publice. Aşadar, reducerea emisiilor de gaze cu efect de seră sau diminuarea impactului asupra sănătăţii de schimbările ar putea avea efecte pozitive asupra sănătăţii;
• Promovarea activităţii fizice sistematice prin intervenţia kinetoterapeutică şi a profesorului de educaţie fizică în această perioadă, a pubertăţii ar putea influenţa pozitiv evoluţia stării de sănătate, mai ales că intervenţia kinetoterapeutului are rolul de a antrena întregul corp în mişcare şi de a pregătii organismul copilului pentru efort;
• Dată fiind importanţa unei bune respiraţii în vederea menţinerii stării de sănătate a organismului şi pentru buna lui dezvoltare în perioada de creştere şi dezvoltare, recomandăm şi un program de gimnastică respiratorie;
• De aceea consider că prin exerciţiile specifice pe care le oferă, kinetoterapia este o soluţie pentru problemele de sănătate ale copiilor din perioada pubertară şi nu numai, învăţându-i în acelaşi timp că mişcarea reprezintă un mod de viaţă sănătos şi armonios.
Bibliografie:
• Alexandrescu, Constantin - Igiena şi controlul medical în sport. Ed. C.N.E.F.S, 1967, pag. 67-80
• Antal, Andrei. Igiena şcolară - Teoria şi practica promovării sănătăţii copiilor şi tinerilor din colectivităţi. Andrei Antal; Colaboratori-consultanţi M. Deleanu ; Magda Farkas, Ed. A 2-a revăzută şi completată: Bucureşti: Editura Medicală, 1978. pag. 37-61
• Ionescu, Adrian N, Mazilu, Virgil - Creşterea normală şi dezvoltarea armonioasă a corpului. Ed. Consilului Naţional pentru educaţie fizică şi sport, Bucureştei, 1968. pag. 104-118 COMPARATIVE REASERCH ON GROWTH AND PHISICAL DEVELOP MENT OF THE SCHOOL AGE CHILDREN BOTH IN URBAN AND IN RUR AL AREAS
AND THE CORRELATION BETWEEN ENVIRONMENTAL FACTORS A ND SOCIAL FACTORS ECONOMIC
Masterand Sîrbu Oana-Alexandra
FEFS Galatzi Keywords: growth, physical development, school age children, environmental factors, social factors economic. Summary: Growth and development of children is one of the problems of human biology with a particular theoretical and practical significance. The essential element that distinguishes the adult child is just the growth and development complex process. One of the important development of human body stages is adolescence wich begins around age of 10

42
years. Pubertal stage (middle school) differ depending on sex: 10 years for girls (10-14 years); 12 years for boys (11-16 years), stage in wich the child grows sharply, then growth slows, all body segments simultaneously grow, develop muscles and increase physical strength. Introduction: Growth is a unique process for each child, fits in large limits, in what is called normality. The main indicators of growth are size, weight, head perimeter, but may be supplemented and chest perimeter and segmentation measurements. Physical development of children presents one of the major indices rising health body and represent all morphological and functional capacity of the body, characterizing the growth and development process. In estimating the growth used usually, quantitative criteria: easy, hard, small, large, short, tall. Development is assessed using qualitative criteria. Is there a good, bad, fast, slow, early, late development. Motivation for choosing the theme: Considering that in the Galati county area, there is no research on the growth and development of the school age children and no correlation on how environmental factors and socio-economic affect growth and development, we consider necessary conducting a longitudinal research to pursue the growth and physical development of children from gymnasium cycle correlated with environmental factors and soio-economic. The aim of research: This research represents an intermediate stage of a longitudinal research that takes place within 4 years, primarily aimed at evaluating factors influencing the growth and development of the school age children. Therefore, the aim of this research is to assess the pace of growth and development of school age children correlated with environmental factors, socio-economic and the level of physical activity. The hypothesis of research: We suppose that environmental factors and socio-economic may influence positively or negatively the growth and development. Material and research methods used: This research is based on a sample of 909 children of secondary school, aged between 10 and 16 years of whom 749 urban and 160 rural (Baneasa and Varlezi localities) and on the following assessment: - anthropometric: height, weight, sitting height, biacromial diameter, bitrohanterian dimeter, transverse thoracic diameter, anterior-posterior chest diameter. Anthropometric data was calculated based on Quetelet index (BMI- body mass index) being considered by WHO as a fundamental criterion in assessing growth of child aged between 2 and 20 years. For analysis of changes in Quetelet index we used the percentile method, the method recommended by WHO. The ratings also were made regarding the level of air pollutants in the area of residence and assessing the physical activity level – physical activity index (questionnaire methode). Statistical processing of results was performed separately for each of the two groups of subjects according to sex and age group, thus: In figures 1 and 2 it can be noted that approximately one third of the children studied at this stage are not developing normally, whether underweight (3,89%), overweight and obese (27,23%).

43
Status share for boys
normal weight 68.88%
underweight 3.89% overweight&obese
27.23 %
Figure number 1
Status share for girls
normal weight 77%
overweight&obese19%
underweight 4%
s
Figure number 2
Regarding drawing number 1 note that the highest ratio of girls/boys, obese and overweight we meet the outskirts of town Galati and lowest in rural areas.
0
5
10
15
20
25
30
35
1 2 3
center periphery rural
Status share for girls/boys by area 2009-2010
supraponderali&obezi fete
supraponderali&obezi baieti
Drawing number 1 Analyzing drawing number 2 we find that girls (20%) are more sedentary than boys (18%) in the study conducted in 2009-2010.

44
Drawing number 2 After carrying out the scientific research of data we want to point the following conclusions:
• Factors that influence the pace of growth and development are: age, gender, environment (urban, rural) and level of physical activity. More than one third of the research group is very sedentary and sedentary with a higher percentage for girls;
• Children studied further increase differences during the period 10-16 years and their body proportions change successively, phenomena which will eventually lead to achieving dismorfic conformation cast, generally the larger male to female;
• Due to early puberty, girls between 12-14 years are higher than boys and boys in this period not yet made their dismorfic characters.
Suggestions: Taking into account this research we point some proposals and control measures in this regard:
• Promoting the safe use of public transportation and active movement, such as cycling or walking as alternatives to using private vehicles – could reduce carbon dioxide emissions and improving public health. Therefore, reducing greenhouse gas could have positive effects on health;
• Promoting physical activity through systematic intervation by physical therapist and physical education teacher at this period, could positively influence the development of health, especially since physical therapist intervation is to train the entire body and to prepare for the effort the body of the child;
• Given the importance of a good breathing to maintain the body health and for his proper development during growth and development, we recommend a respiratory exercise program too;
• Through specific exercises that it offers, physical therapy is a solution for health problems of children and not only during pubertary, teaching them in the same time that movement is a healthy lifestyle and balanced.
0,0%
20,0%
40,0%
60,0%
male female
Comparision chart of physical activity index by sex 2009-2010
very sedentary sedentary active very active

45
ASPECTE IMAGISTICE ALE COMPLICA ŢIILOR RAHIDIENE POSTOPERATORII
Lect dr. Marinescu Rodica
Cuvinte cheie: biomecanica , postoperator fibroza epidurala, spondilo-discita,
laminectomie, imagistica prin rezonanta magnetica, meningocel Rezumat: Coloana vertebrală constituie axul de susţinere a întregului schelet al
corpului. În ansamblul ei este un complex de vertebre cu diversele lor legături (articulaţii, cartilaje, ligamente). Unitatea funcţională în biomecanica coloanei vertebrale este „segmentul motor”. Examenul prin rezonanţă magnetică a segmentului vertebro-medular a devenit în multe situaţii examenul de primă intenţie, deoarece este neiradiant, neinvaziv şi permite examenul tuturor compartimentelor. Cele mai frecvente complicatii postoperatorii sunt : fibroza peridurala, arahnoidita, spondilo-discita, pseudomeningocelul si sindromul de hipotensiune intracraniana spontana
1. Noţiuni generale de anatomie şi biomecanică a coloanei vertebrale
Coloana vertebrală constituie axul de susţinere a întregului schelet al corpului. În ansamblul ei este un complex de vertebre cu diversele lor legături (articulaţii, cartilaje, ligamente). Coloana este împărţită în cinci segmente, după criterii anatomice, biomecanice, patologice, etc. Între cele cinci segmente enunţate, se remarcă zonele intermediare,
tranziţionale, numite şi „zone de joncţiune”. Acestea sunt: - joncţiunea occipito-cervicală (C0-C2); - joncţiunea cervico-toracală (C7-T1); - joncţiunea toraco-lombară (T12-L1); - joncţiunea lombo-sacrată (L5- sacru). Unitatea funcţională în biomecanica coloanei vertebrale este „segmentul motor”,
denumit astfel de către Junghanns şi cuprinde totalitatea formaţiunilor disco-ligamentare dintre două corpuri vertebrale, pe care le solidarizează şi le conferă mobilitate.
2. Tehnica examenului IRM verterbro-medular
Examenul prin rezonanţă magnetică a segmentului vertebro-medular a devenit în multe situaţii examenul de primă intenţie, deoarece este neiradiant, neinvaziv şi permite examenul tuturor compartimentelor (osos, epidural, intradural şi medular), precum şi examinarea multiplanară. O examinare standard trebuie să cuprindă secvenţe sagitale T1 şi T2, secvenţe rapide de tipul T2 FSE, secţiuni coronale T1 sau T2, axiale T2 sau T2*, secvenţe STIR şi administrare de contrast i.v. Grosimea secţiunilor trebuie să fie adaptată regiunii examinate. Astfel, grosimea va fi de 4mm pentru coloana cervicală, 4-5mm pentru regiunea toracală şi 5-6mm pentru coloana lombară. Se utilizează benzi anterioare de presaturare. Antenele folosite sunt de tip ”body” şi antene de suprafaţă. Cele de tip „body” sunt încorporate în gantry şi au rol de emisie şi de recepţie, iar cele de suprafaţă au numai rol de recepţie.

46
3. Aspecte normale postoperatorii Următoarele imagini pot apare în mod normal în perioada postoperatorie a unei hernii
discale: - hemilaminectomie cu absenţa ligamentelor galbene şi eventual rezecţia parţială a faţetei articulare superioare; - laminotomie; - ţesut cicatriceal pe traiectul abordului chirurgical; -deformarea sacului dural asemănător cu perioada preoperatorie, în primele trei săptămâni; - imagini în hipersemnal în regiunea curetată, vizibile pe secţiunile axiale, cu priză de contrast; - încărcare heterogenă a spaţiului epidural, a zonei de laminectomie, a faţetelor articulare, tecilor nervoase şi a ţesutului muscular adiacent, încărcare care poate persista până la o lună; - mici colecţii hemoragice în spaţiul epidural; - remanieri inflamatorii ale platourilor vertebrale; -artefacte prin susceptibilitate magnetică a microparticulelor metalice de pe traiectul operator.
4. Imagistica unor complicaţii postoperatorii
Fibroza peridurală
Reprezintă o cicatrice apărută postintervenţie chirurgicală pe coloana lombară şi este responsabilă de 10% din cauzele durerii recurente de după discectomie. Ea este situată în continuitatea cicatricei de pe calea de abord chirurgical. Patogeneză- extinderea fibrozei e posibil legată e extinderea inciziei chirurgicale, precum şi de răspunsul inflamator al gazdei. Ţesutul cicatriceal comprimă, irită şi exercită o tracţiune anormală pe rădăcinile nervoase. În acelaşi timp, aportul sanguin este compromis şi transportul axoplasmic întrerupt. Aspect IRM – de reţinut că în fazele iniţiale este greu de diferenţiat imagistic o fibroză epidurală patologică de o reacţie cicatriceală reparatorie, fiziologică ; deaceea se preferă examinare după 4-6 săptămâni postoperator.
Se observă infiltrarea grăsimii epidurale şi perineurale de către structuri cu semnal de ţesut moale. Uneori poate să îmbrace aspect tumoral şi să exercite efect de masă asupra sacului dural şi a rădăcinilor nervoase (trama de ţesut de colagen are aspect hipertrofic). La început, semnalul este intermediar T1 şi hiperintens T2, iar după 2-3 luni când începe organizarea scleroasă, apare hiposemnal T1 şi se menţine hipersemnalul T2.
Caracteristic este întărirea semnalului imediat postcontrast. Această întărire postGd prezintă acurateţe de aproximativ 96% în ceea ce priveşte diferenţierea fibrozei de hernia de disc recurentă. Un fragment discal se poate încărca şi el cu substanţă de contrast, dar mult mai târziu.
Supresia grăsimii pre- şi post- contrast, poate să crescă sensibilitatea. Gadolinofilia fibrozei este maximă la o lună postoperator, iar după 6-14 luni apare semnal de tip fibros.

47
Pseudomeningocelul Se mai numeşte şi dehiscenţă durală sau pseudochist şi reprezintă un chist spinal nedelimitat de meninge, care se continuă cu sacul tecal. Se formează prin hernierea arahnoidei printr-o breşă durală, apărută cel mai adesea postoperator.
Poate fi şi o complicaţie posttraumatică şi în acest caz nu sunt elemente nervoase. Pseudomeningocelul postoperator poate conţine elemente nervoase. Patogeneză- posttraumatic, cel mai frecvent prin avulsia rădăcinii cervicale sau postoperator prin dilacerare durală, cu scurgerea LCR-ului. Aspect imagistic – chist spinal cu semnal lichidian identic cu LCR-ul şi aspect pediculat la inserţia sa durală. Orientarea este de-a lungul inciziei şi poate conţine elemente nervoase herniate. Comunicarea cu sacul tecal se demonstrează folosind T2 axial şi sagital. Post contrast semnalul se intensifică doar dacă este inflamat sau infectat. Totuşi se poate observa întărire şi îngroşare durală craniană şi spinală la pacienţii cu hipotensiune LCR simptomatică.
Între rădăcinile nervoase şi pseudomeningocel se pot forma aderenţe. Pseudochistul poate fi compresiv dacă are dimensiuni crescute.
Secvenţele ponderate T2 sau FSE IR sunt cele mai bune pentru a demonstra existenţa pseudomeningocelului şi pentru a localiza comunicarea sa durală. Examenul trebuie completat cu secţiuni axiale subţiri. Diagnosticul diferenţial se face cu :
- meningocelul adevărat (nu are istoric traumatic sau chirurgical şi adesea coexistă cu displazia durală);
- neurofibromul plexiform (nu apare la fel de strălucitor ca LCR-ul şi se încarcă postcontrast);
- colecţii lichidiene seroase sau abcese dezvoltate în musculatura paraspinală (nu comunică cu sacul dural);
- ectazii laterale ale sacului dural în zona de laminectomie pe traiectul operator. Spondilo-discita
Spondilo-discita postoperatorie este de obicei inflamatorie şi se instalează în intervalul 1săptămână-3 luni. Aspectul IRM – modificările sunt de tip lichidian, în hiposemnal T1 şi hipersemnal T2 , cu captarea substanţei de contrast, la care se poate asocia edem şi gadolinofilie epidurală şi paravertebrală.
Se consideră patologică încărcarea platourilor vertebrale adiacente discectomiei după 6 săptămâni de la actul operator. Modificările degenerative tip ModicI nu se încarcă cu contrast sau se încarcă foarte puţin.
Sindromul de hipotensiune intracraniană spontană (SIH)
Acest sindrom constă în presiune scăzută a LCR-ului, cu congestie venoasă compensatorie. Poate fi: spontan, traumatic sau iatrogen (după puncţie lombară, postchirurgical). Patogenie – scăderea presiunii LCR precipitată prin:
- manevre chirurgicale; - traumatisme; - exerciţii fizice intense sau tuse violentă; - puncţii lombare; - anomalii ale durei (sdr. Marfan); - diverticul arahnoidian rupt; - deshidratare severă.

48
Sindromul este de două ori mai frecvent la femei, cu un vârf de vârstă de 30-40 ani. Aspecte imagistice – examenul IRM evidenţiază îngroşarea durei, mărirea venelor
epidurale şi colecţie de lichid în izosemnal cu LCR-ul. În ponderaţie T1 se pune în evidenţă lichid izointens cu LCR ventral şi anterolateral, eventual fenomenul de „flow voids”. În ponderaţie T2 apare lichid extraaxial în izosemnal LCR (poate fi hiperintens în PD) şi se poate observa diverticul arahnoidian.
După administrarea de gadolinium se constată captare intensă, plex venos mult lărgit, îngroşare durală variabilă şi captare a substanţei de contrast.
Secvenţele STIR sau ponderate T2 cu FS pot pune în evidenţă diverticuli arahnoidieni (adesea multipli) şi pot demonstra scurgerea LCR.
Se recomandă mai întâi examinare cerebrală, care poate arăta: - îngroşarea durei şi gadolinofilie; - „sagging midbrain”; - hernie tonsilară; - hygrom subdural.
Se va avea în vedere că nu toate cazurile prezintă toate caracteristicile clasice de diagnostic. Diagnosticul diferenţial se face cu:
- alte cauze de lărgire a plexului venos (anevrisme, tromboza venei jugulare, congestie venoasă deasupra stenozei spinale de grad înalt);
- pahimeningopatii (abcese epidurale).
Arahnoidita
Produce aderenţe ale rădăcinilor nervoase, care par acolate pe sacul dural, conferindu-i un contur neregulat. Inflamaţia meningelui îl face să apară îngroşat şi cu semnal crescut postcontrast. În cazurile avansate, rădăcinile sunt deformate şi pot fi confundate cu tumori ale tecilor nervoase. În timp se pot forma chiste arahnoidiene care să comunice sau nu cu spaţiile subarahnoidiene. BIBLIOGRAFIE
1. Brant- Zawadzki, M.;Norman D.; Magnetic Resonance Imaging of the Central Nervous System- Raven Press New York-1997;
2. Exergian Fl.; Tratat de patologie spinală – Bucureşti , 2004; 3. Mihăiţă I.; Opriş L; IRM vertebro- medular; - Bucureşti 2000; 4. Rohen; Color Atlas of Anatomy – Lippincott WW-2003; 5. Stoller; Pocket Radiologist- Musculoskeletal; - Saunders- 2002.
IMAGING ASPECTS OF POSTOPERATIVE SPINAL COMPLICATI ONS
Keywords: biomechanics, postoperative epidural fibrosis, spondylo disk, laminectomy, magnetic resonance imaging, meningocele
Abstract: The spine is the axis of support of the entire skeleton of the body. The whole complex is connected with their different vertebrae (joints, cartilage, ligaments).
Biomechanics of the spine functional unit is the ‘engine segment.” Magnetic resonance examination of the spine segment in many instances become the first choice examination because it is irradiated, and allows noninvasive examination of all compartments. The most common postoperative complications are epidural fibrosis, Arachnoiditis, spondylo-disk pseudomeningocelul spontaneous intracranial hypotension syndrome

49
1. General knowledge of anatomy and biomechanics of the spine The spine is the axis of support of the entire skeleton of the body. The whole complex
is connected with their different vertebrae (joints, cartilage, ligaments). The column is divided into five segments, anatomical criteria, biomechanics, pathology, etc..
Among the five sections mentioned, it is noted in intermediate, transitional, called junction zones they are:
- Occipito-cervical junction (C0-C2); - Cervico-thoracic junction (C7-T1); - Thoraco-lumbar junction (T12-L1); - Lumbo-sacral junction (L5-sacred). The functional unit in the biomechanics of the spine is “engine segment,” so named by
Junghanns and includes all formations disco-ligament between two vertebral bodies, which are common cause and give them mobility.
2. MRI technique verterbro-marrow examination: Magnetic resonance examination of the spine segment has become in many cases
examination of first choice because it is irradiated, and allows noninvasive examination of all compartments (bone, epidural and spinal intradural) and many planar examination.
A standard examination should include sagittal T1 and T2 sequences, a sequence type T2 ESF, T1 or T2 coronal sections, axial T2 or T2 * sequences ESRF and iv contrast administration should be appropriate thickness sections of the region considered. Thus, thickness is 4mm to cervical spine, thoracic Region 4-5mm and 5-6mm for the lumbar spine. Previous bands of presaturation are used. The antennas used are of the body type surface antennas. The type body are incorporated into the gantry and act as transmission and reception, and those are only part of the reception area.
3. Normal postoperative aspects The following images may appear normal in the postoperative period of a disc hernia: - Hemilaminectomie yellow ligament and the absence of any partial resection of
superior articular facet; - - Laminotomie; - - Scar tissue on the surgical approach path; - Dural sack deformation which is like during the preoperative period, in the first
three weeks; - hipersemnal images in the region cleaned visible on axial sections with contrast
setting; - heterogeneous loading of the epidural space, the area of laminectomy, the facet
joints, nerve and muscle sheaths adjacent loading may persist up to a month; - Small collections of bleeding in the epidural space; - reshuffle inflammatory vertebral plateaus; - magnetic susceptibility artifacts through the metal micro-controller path.
4. Imaging of postoperative complications
Epidural fibrosis Represents a surgical scar on the lumbar spine appeared postsurgery and is responsible for
10% of cases of recurrent pain after discectomy. It is located in the path continuity scar surgical approach.
Pathogenesis- the extension of fibrosis is possible in connection with the extension of the surgical incision, and with the hostess’ inflammatory response. Scar tissue compress, irritate

50
and exercise abnormal traction on the nerve roots. At the same time, the blood supply is compromised and interrupted axoplasmic transport.
MRI Appearance - please note that in the early stages is difficult to distinguish epidural fibrosis imaging a pathological reparative scar reaction, physiological, therefore it is preferred examination after 4-6 weeks postoperatively.
Observe epidural fat and perineural infiltration by soft tissue structures with signal. Sometimes it could take part and exert tumor mass effect on the dural sack and nerve roots (the texture looks hypertrophic collagen tissue). In the beginning,it is intermediate T1 signal and hyperintense T2 and after 2-3 months when the organization begins sclera appears hiposemnal T1 and T2 is maintained.
Characteristic is to strengthen the immediate postcontrast signal. This strength has postGd approximately 96% accuracy in the differentiation of recurrent disc herniation fibrosis. A disc fragment can be loaded with contrast too, but much later.
Fat suppression pre-and post-contrast, may increase sensitivity. Gadolinofilia fibrosis is maximum one month after surgery and after 6-14 months signs
of fiber type appear.
Pseudomeningocelul Also known as dural dehiscence is a cyst or pseudocyst and unlimited spinal meningitis,
which continues to tecal bag. It is formed by arachnoid herniation through a dural hole, occured most often after surgery.
It can be a traumatic complication and in this case there are not nervous elements. Pseudomeningocelul surgery may contain nerve elements. Pathogenesis-trauma, most
commonly by cervical root avulsion or postoperative dural through dilacerare with CSF leakage site.
Aspect imaging - spinal cyst with fluid signal identical to LRC and pediculated aspect in the dural insertion. Orientation is along the incision and may contain nerve elements hernia. Communication tecal bag is demonstrated using axial and sagittal T2. Post contrast enhances the signal only if it is inflamed or infected. However, it is apparent hardening and thickening of cranial and spinal dural hypotension in patients with symptomatic CSF.
Between pseudomeningocel nerve roots can form adhesions. Pseudocyst may be compressive if the size is increased.
ESF IR or T2-weighted sequences are the best to prove the existence and to locate pseudomeningocelului dural communication. The exam must be completed by axial thin sections.
The differential diagnosis is made with: - Meningocele true (not traumatic or surgical history, and often coexists with dural
dysplasia); - Plexiform neurofibroma (does not appear as bright as LCR and it is postcontrast
loaded); - Serous fluid collections or abscesses developed in paraspinal muscles (not
communicating with the dural sack); - Ectasis on sides of the dural sack in the area of laminectomy on the operator path.
Spondylo disk Spondylo disk postoperative is usually inflammatory and it is installed within 1week-3
months.

51
MRI appearance - changes are fluid type in hiposemnal hipersemnal T1 and T2, with the capture of the contrast, which may be associated edema and epidural and paravertebral gadolinofilie.
It is considered pathological loading shelves adjacent vertebral discectomiei act after 6 weeks from the surgery act. Modici degenerative changes do not charge with contrast or they charge very little.
Spontaneous intracranial hypotension syndrome (SIH) This syndrome consists of low pressure of CSF`s, with compensatory venous congestion.
Can be: spontaneous, traumatic or iatrogenic (after lumbar puncture, postsurgical). Pathogenesis - precipitated by lowering CSF pressure:
- Surgical procedures; - Trauma; - Strenuous exercise or violent cough; - Lumbar puncture; - Abnormalities of the dura (Marfan sdr.) - Diverticulum arahnoidian broken; - Severe dehydration.
The syndrome is twice as common in women, with a peak age of 30-40 years. Issues imaging - MRI examination shows thickening of the dura, and epidural veins increased collection of fluid in the CSF izosemnal site. In T1 ponderation underline the CSF fluid izointens ventral and anterolateral possibly phenomenon of flow voids.In ponderation T2 appears in izosemnal extraaxial CSF fluid (may be hyperintense on PD) and you can see arahnoidian diverticulum. After gadolinium administration there is intense abstraction, much enlarged venous plexus, dural thickening and variable capture of the contrast. T2-weighted sequence with FS news and highlights diverticula can arahnoidieni (often multiple) and may demonstrate CSF leakage. It recommends first examining brain, which can show:
- Thickening of the dura and gadolinofilie; - midbrain sagging - Hygrom subdural.
It will take into account that not all cases have all the classic characteristics of the diagnosis. The differential diagnosis is made with:
- Other causes of venous plexus enlargement (aneurysm, jugular vein thrombosis, venous congestion, high above the spinal steno
- Pahimeningopatii (epidural abscess).
Arachnoiditis
It produces adhesions of nerve roots, which seem acolytes on dural sack, giving an irregular contour. Inflammation of the meninges that makes him appear strong and increased postcontrast signal. In advanced cases, the roots are deformed and can be confused with tumors of nerve sheaths. In the meanwhile arahnoidiene can form cysts that communicate or not with the suarachnoid spaces .

52
ABORDARE KINETIC Ă ȘI NUTRI ȚIONAL Ă A OBEZITĂȚII.
(STUDIU)
Dr. Viorica Lefter , Facultatea KinetoterapiGalați. Dr.Oana Andreea Cibu ,Facultatea deMedicină Galați Cuvinte cheie:kinetoterapie,aport caloric,indice de masaă corporală.IMC(BMI) Obezitatea .Definiție.Este starea patologică datorată tulburării funcţiei de nutriţie sau endocrine, ce perturbă echilibrul între aportul caloric şi pierderile energetice ale organismului, evidenţiată prin depuneri excesive de de grăsime, uniform sau localizate în anumite regiuni ale corpului.(1) Tipurile de obezitate : după debut; 1.hiperplazica -este de debut caracteristica copiilor supraalimentati 2.hipertrofica- debutează după 18-20 de ani. Etiopatogenie ; I.factori endogeni; predispoziţia genetică 80% din 2 părinți,50% 1 părinte.,predispoziţia constituţională II. factori exogeni (supra alimentaţia , 80%-90%). Incidența :OMS (1997) ,,epidemie de obezitate,, SUA 36%,Europa centrală 15-20%, Est 40-50%,România 20-25% din populaţia generală. Incidenţa mai mare la sexul feminin si după 40 de ani.(2) Ex. clinic .1.cântărire 2.măsurarea pliului cutanat3.circunferințe 4.calcularea IMC. Material și metodă.Cercetarea a fost realizată pe un lot 138 de subiecţi (femei) cu probleme ponderale ,de diverse vîrste și grade de afectare,în perioada septembrie 2007 - 2009, în stațiunea Lacu-Sărat și Centru de Recuperare Medicală ,,Sc Fiziter SRL.,,Brăila.Lotul de studiu a fost împărțit în 2 subloturi și anume un lot martor A ,compus din 57 (41%) paciente care au beneficiat doar de dietă,calculate tot după consumul energetic zilnic și care nu au dorit să participe la programele kinetice de grup și la domiciliu, și un lot experimental B, compus din 81(69%) paciente care au beneficiat atât de dietă cât și de programe kinetice, Programele kinetice au fost individualizate fucție de posibilitățile kinetice ale fiecărui caz. Parametrii urmări ți au fost; IMC,dimensiunea taliei, greutate , au fost testați săptămînal dar pentru studiu au fost estimate (inițial, intermediar și final.) Rezultate:Evoluția taliei s-a redus de la 95cm la 87 cm,de la 120cm la 99cm și de la 148cm la 139cm respectiv cu 7,5 cm la 24,5% din pacienți, cu 11cm la 54,5% din pacienți și cu 9 cm la 19,5% din pacienți.S-a constatat o asuplizare a persoanelor ,o abilitate mai mare în mișcări , atît la sală cît și în viața de zi cu zi.IMC supraponderali la intrarea în studiu au fost 24,3% inițal, la final procentul ajuns la 42,6% prin preluare de la obezitate și ob extremă.Procentul de obezitate s-a redus de la 54,4% la 37,6% la finele studiului.Procentul obezității exterme s-a redus de la 19,3% la 17,8 %. Controlul greutăţii, pas obligatoriu în monitorizarea obezităţii. Am obținut ;1.Scădere în gr. 2-5kg.(14%)2.Scădere în gr. 5-8 kg.(16%) 3.Scădere în gr. 10-12kg.(21%)4.Scădere în gr. 12-15 kg.(26 %) 5.Scădere în gr. 15-20-kg.(9%) 6.Fluctuații nesemnificative statistic(14%) Concluzii.Terapia constă în optimizarea stilului de viaţă, respectiv dietă moderat hipocalorică şi activitate fizică regulată, terapie comportamentală, medicaţie specifică şi motivație. . Aceste metode se aplică diferit în faza de scădere ponderală şi cea de menţinere şi mai ales în funcţie de obiective. Introducere.Obezitatea .Definiție.Este starea patologică datorată tulburării funcţiei de nutriţie sau endocrine, ce perturbă echilibrul între aportul caloric şi pierderile energetice ale organismului, evidenţiată prin depuneri excesive de de grăsime, uniform sau localizate în anumite regiuni ale corpului(1).Tipurile de obezitate : după debut; 1.hiperplazica -este de debut caracteristica copiilor supraalimentati ,2.hipertrofica- debutează după 18-20 de ani. După formă %- obezitate uşoara creşterea greutăţii corporale cu peste 15% din greutatea ideala;obezitate mijlocie cu peste 20%; obezitate mare cu peste 30%.După repartizarea depozitelor ; tip "ginoid “ - pe burta, şolduri si coap, ,,tip android ,, - ştergere a liniei taliei, ,,tip general,, Etiopatogenie 1. factori endogeni Predispoziţia genetică 80% din 2

53
părinți,50% 1 părinte.Predispoziţia constituţională(3) 2. Factori exogeni.Supra alimentaţia , 80%-90.Numărul meselor ,masa unică luată seara,Consumulde alcool ,Sedentarismu ,Stresul ,Traumele psihice (7,40% pentru femei şi 10% pentru bărbaţi .Incidența :OMS (1997) ,,epidemie de obezitate,, SUA 36%,Europa centrală 15-20%, Est 40-50%,România 20-25% din populaţia generală. Incidenţa mai mare la sexul feminin si după 40 de ani. Ex. clinic 11.cântărire 2.măsurarea pliului cutanat3.circunferințe 4 IMC.Pentru a măsura supra-ponderalitatea şi obezitatea putem folosi un indicator IMC (Indexul Masei Corporale) sau BMI (Body Mass Index) se calculează astfel: IMC(kg/m2) = masa corporală(kg) / înălţime(m2). Valorile acceptate internaţional ale indicatorului BMI sunt redate în
Tabelul 1
(:tabel 1)DIAGNOSTIC se bazează pe;Excesul ponderal.Repartizarea depozitelor .Edeme declivbe.Dispnee de efort .Suprasolicitare hemodinamică.Dureri în artic. suprasolicitate Diagnosticul diferențial: Sindromul Couching , Hipotiroidismul , Hiperinsulinismul , Limfedemele, Evoluție. 1. I-a fază este dinamică și se caracterizează prin: - polifagie și lipogeneză.2. a-II-a fază, statică, greutatea se
stabilizează se instalează treptat complicaţiile.Complicaţii : Metabolice, respiratorii, osteoarticulare , infiltrarea grasă a ficatului , ateroscleroza hipogonadism .Prognostic; Speranţa de viaţă este cu 10 ani mai mică decât la restul populaţiei.Managementul obezității este redat în tabelul ORGANIZAREA ȘI DESFĂȘURAREA CERCETĂRII Cercetarea a fost realizată pe un lot 138 de subiecţi (femei) cu probleme ponderale ,de diverse vîrste și grade de afectare,în perioada septembrie 2007 - 2009, în stațiunea Lacu-Sărat și Centru de Recuperare Medicală ,,Sc Fiziter SRL.,,Brăila.Lotul de studiu a fost împărțit în 2 subloturi și anume un lot martor A ,compus din 57 (41%) paciente care au beneficiat doar de diverse forme de dietă,calculate tot după consumul energetic zilnic și care nu au dorit să participe la programele kinetice de grup și la domiciliu, și un lot experimental B, compus din 81(69%) paciente care au beneficiat atât de diversele forme de dietă cât și de programe kinetice, stabilite în funcție de particularitățile fiecărui caz.(grafic I)
1
2
3
Graficul I .Structura lotului de studiu
sub-ponderal
< 18.5
normal 18.5-24.9
supra-ponderal 25 - 29.9
obezitate 30 -39.9
obezitate extremă
> 40
-- 5544,,44%%oobbeezziittaattee ,, -- 2244,,33%%ssuupprraappoonnddeerree,, -- 1199,,33%% oobb.. eexxttrreemmăă
1
2
A 57 (41%)-dietă B 81 (69%) -dietă+kineto

54
În această perioadă am efectuat subiecţilor 3 testări (ini ţială, intermediară (la o lună )și finală, după 6 luni), urmărind evoluţia fiecărui caz și elaborând noi programe de exerciţii corespunzătoare receptibilităţii pacienţilor la programele kinetice impuse iniţial. Lotul A a beneficiat de aceleași diete : 1.dieta de testare, 2.dieta de 14oo kcal, 3.dieta de 1500 kcal, 4.dieta de 1600 kcal, 5.dieta de 1800 kcal.Pentru lotul experimental am structurat programul de slăbire in felul următor:Dieta de testare metabolică 14 zile.Dietă funcție de consumul energetic, vîrstă, sex după tabel.Program kinetic de inițiere.Program kinetic de dificultate mică.Program kinetic de dificultate medie .Program kinetic de dificultate mare .Reevaluare la 30 zile.Program pe termen :scurt, mediu și lung după posibilități. În funcţie de gradul obezităţii, obiectivele propuse şi caracteristicile personale am recomandat următoarele diete: 1.Dieta cu deficit de 1800 kcal/zi faţă de alimentaţia anterioară, ce poate determina o scădere ponderală de 0,5-1 kg/săptămână, 5-10 kg în 3 luni (aproximativ 5-10% din greutatea iniţială); 2.Dieta cu deficit de 1.600 kcal/zi faţă de alimentaţia anterioară, urmată de scădere ponderală de 1-2 kg/săptămână (aproximativ 20% din greutatea iniţială), recomandată la pacienţii cu risc crescut şi foarte crescut; 3.Dieta hipocalorică standard de 1.500 kcal/zi, care necesită recomandarea şi urmărirea de medicul specialist în diabet, nutriţie, boli metabolice; 4.Diete intens hipocalorice, 1400 kcal/zi, care produc o scădere ponderală marcată şi rapidă, dar nu lipsită de efecte secundare, motiv pentru care acest tip de dietă are indicaţii specifice, se aplică pe o durată scurtă de maximum 1-2 luni şi doar sub supravegherea specialiştilor în diabet, nutriţie, boli metabolice. Nu există evidenţe ştiinţifice asupra superiorităţii diverselor diete comerciale sau a celor disociate, bogate în proteine şi sărace în glucide. În plus, acest tip de diete se pot însoţi de efecte negative asupra organismului, motiv pentru care nu sunt recomandate decât, eventual, sub stricta supraveghere a specialiştilor consacraţi în nutriţie. În perioada de menţinere a greutăţii, dieta hipocalorică va putea fi completată cu 200-300 kcal, în condiţiile intensificării exerciţiului fizic, astfel ca balanţa energetică să se menţină negativă. Programele kinetice au fost individualizate fucție de posibilitățile kinetice ale fiecărui caz Parametrii urm ări ți: Parametrii urmăriți au fost; IMC,dimensiunea taliei, greutate , parametrii au fost testați săptămînal dar pentru studiu au fost estimate (inițial, intermediar și final.) Programul a cuprins și un studiu al motivației (inițial și final) Programele kinetice au fost individualizate fucție de posibilitățile kinetice ale fiecărui caz.Exemplu : pentru începători, Pilates,exerciții de dificultate mică Tip I ;pentru ciclul 2-3 exerciții de dificultate medie și severă.Tip II,III.(Fig. 2) La începutul ciclului de tratament motivația a fost în proporție de 76, 1 % prezentă, pe parcursul ciclurilor se menține ridicată la persoanele care au avut rezultate în terapie ,cu fluctuații lunare scade progresiv la persoanele cu rezultate nesatisfăcătoare, chiar sunt perioade de depresie.La sfirșitul ciclurilor persoanele care și-au schimbat modul de viață motivația crește. .EVOLUȚIA DIMENSIUNILOR TALIEI În urma tratamentului aplicat, dimensiunile taliei sunt primele care se modifică , uneori fără modificări de greutate kg.Evoluția taliei a variat între 1,95cm-12cm, 12 cazuri au avut oscădere a taliei de peste 12cm.Evoluția taliei s-a redus de la 95cm la 87 cm,de la 120cm la 99cm și de la 148cm la 139cm respectiv cu 7,5 cm la 24,5% din pacienți, cu 11cm la 54,5% din pacienți și cu 9 cm la 19,5% din pacienți.S-a constatat o asuplizare a persoanelor ,o abilitate mai mare în mișcări , atît la sală cît și în viața de zi cu zi.

55
0
5
10
15
20
25
1 2 3
1
2
3
Graficul II . Evoluția taliei lot studiu, lot martor. Evoluția taliei la lotul martor.(57) din care 13(23%) și-au redus talia ci 2-5cm,23 pacienți (40%) cu 5-7 cm și 21 pacienți (37%) cu7-10cm.. Pentru a măsura supra-ponderalitatea şi obezitatea putem folosi un indicator IMC (Indexul Masei Corporale) sau BMI (Body Mass Index) se calculează astfel: IMC(kg/m2) = masa corporală(kg) / înălţime (m2).Valorile IMC se modifică cel mai lent în evoluția lotului de studiu. Pentru acuratețea studiului am verifical IMC la începutul și sfîrșitul fiecărui ciclu. Vlorile de referință statistică au fost cele inițiale și finale.Dacă supraponderali la intrarea în studiu au fost 24,3% inițal la final procentul ajuns la 42,6% prin preluare de la obezitate și ob extremă. Procentul de obezitate s-a redus de la 54,4% la 37,6% la finele studiului.Procentul obezității exterme s-a redus de la 19,3% la 17,8 %.În decursul studiului au fost și abandonuri ,dar au intrat alte persoane , astfel încît procentele au rămas aceleași După cel puțin 3-5 cicluri într-un an. Diferențele semnificative statistic față de lotul martor la care s-a aplicat doar tratamentul dietetic specific .(grafic II)
0
10
20
30
40
50
60
1 2 3
1
2
3
Graficul II . Evoluția IMC inițial și final
Controlul greutăţii, pas obligatoriu în monitorizarea obezităţii Am obținut scăderea ponderală în trepte, cu unul sau mai multe cicluri de „scădere ponderală-menţinere”. Această strategie de abordare a obezităţii se bazează pe succesiunea de cicluri “scădere ponderală-menţinere”. Un astfel de ciclu constat în etapa de scădere ponderală, ce a avut ca obiectiv reducerea greutăţii cu 5-10%, obţinută în 3-6 luni, urmată de o perioadă de 3-6-9 luni de menţinere a noii greutăţi. Ciclurile au fost repetate până la atingerea greutăţii optime propuse.
1.Scădere în gr. 2-5kg.(14%) 2.Scădere în gr. 5-8 kg.(16%) 3.Scădere în gr. 10-12kg.(21%) 4.Scădere în gr. 12-15 kg.(26%) 5.Scădere în gr. 15-20-kg.(9%) 6.Fluctuații nesemnificative statistic(14%)
Graficul III. Evoluția greutății lot de studiu
0
2
4
6
8
10
12
1 2 3
1
2
3
77 ccmm 2244,,44%%
1111 ccmm 5544,,33%%
99ccmm 1199,,33%%
0
10
20
30
40
50
1 2 3
,42,6 %
1
2
3
17,8%
37,6%
1. IMC 25-29,9 24,3%suprapondere
2. IMC 30-39,9 obezitate 54,5%
3. IMC > 40 ob. Extremă 19,3%
0
10
20
30
40
50
1 2 3 4 5 6
1
2
3
4
5
6
99ccmm 1199,,33%%
2233%% 55--77ccmm
3377%%77--1100ccmm 4400%% 22--55ccmm ccmm 1199,,33%%

56
Lotul de studiu a beneficiat de 3 săptămîni de dietă de testare la care 89% dintre paciente au pierdut în greutate minim 4 kg.Dupa care s-a intocmit fi șa personală cu tipul de dietă (nr . kcal admis conform tipului de efort al fiecărei persoane) obținîndu-se valorile din graficul III ȘI adaptîndu-se de la ciclu la ciclu slăbire /menținere. CONCLUZII Principiile de bază ale managementului clinic în obezitate sunt: 1.Intervenţie continuă, cu obiective eşalonate pe termen scurt şi lung; adaptate periodic și individual.2. Colaborare strânsă cu persoana cu obezitate în stabilirea obiectivelor şi metodelor terapeutice după parametriclinici, monitorizare,evaluare periodică.3. scăderea ponderală în trepte, cu unul sau mai multe cicluri de „scădere -menţinere”. Această strategie de abordare a obezităţii se bazează pe succesiunea de cicluri “scădere ponderală-menţinere”. Un astfel de ciclu constă în etapa de scădere ponderală, ce are ca obiectiv reducerea greutăţii cu 5-10%, obţinută în 3-6 luni, urmată de o perioadă de 6-9 luni de menţinere a noii greutăţi. Ciclurile pot fi repetate până la atingerea greutăţii optime propuse. Obiectivele pe termen lung ar trebui să fie obţinerea greutăţii normale, adică cea corespunzătoare unui IMC <25 kg/m². În realitate, acest lucru este foarte greu de realizat şi mai ales de menţinut. Din acest motiv, se consideră că cel mai realist obiectiv pe termen lung este menţinerea pentru cel puţin 2 ani a noii greutăţii obţinute după etapa de scădere ponderală. BIBLIOGRAFIE 1.Harrison - editia 14, vol. 2 “Educatia terapeutica specifica in managementul clinic al obezitatii“. 2.www. amf-b.ro. 3.Kopelman P.G. Obesity as a medical problem. Nature 2000; 404:635-643 Cummings D.E., Schwartz M.W. Genetics and pathophysiology of human obesity. Annu Rev Med 2003; 54:453-471. 4.Cornelia Pencea, Constantin Ionescu-Tirgoviste. Obezitatea. In: Constantin Ionescu-Tirgoviste. Capitol 34. Tratat de Diabet Paulescu. Bucuresti: Editura Academiei Romane; 2004: 710-725. 5.Fraga Paveliu, Sorin Paveliu, Abordarea moderna a scăderii in greutate, Editura AII, Bucureşti, 2004 pp132-15
KINETIC AND NUTRITIONAL APPROACH OF THE OBESITY. (S TUDY )
Dr. Viorica Lefter , Faculty of Kinetotherapy of Galați. Dr.Oana Andreea Cibu , Faculty of Medicine of Galați ABSTRACT Keywords: kinesitherapy, caloric contribution, IMC (BMI.)body mass index. Obesity. Definition. It is a pathological condition caused by the nutrition or endocrine function disorders that disturb the equilibrium between the caloric contribution and the body’s energetic losses, highlighted by excess body fat uniformly or localized in particular body regions. (1) Types of obesity: first appearance; 1. hyper plastic – develops typically in children who are over-nourished.2. Hypertrophic obesity – develops after the age of 18 -20. Etiopathogeny; I. endogenous factors; genetic predisposition 80% of 2 parents, 50% 1

57
parent, constitutional predisposition II. Exogenous factors (over-nourishment, 80%-90%). Incidence: OMS (1997)”obesity outbreak, USA 36%, Central Europe 15-20%, Eastern Europe 40-50%, Romania 20-25% of the population. There’s an increase in obesity incidence that goes for women and for those aged over 40. (2) Clinical examination. 1. weighing 2. Measurement of skin fold thickness 3. Girth 4. BMI calculation. Material and method. The research was made during September 2007-2009, in Lacu-Sărat Resort and ,,Sc Fiziter SRL” Medical Recovery Centre in Braila. The study batch was split in two sub-batches, that is a witness batch A made of 57 women patients (41%) that benefited only from the diet, calculated after the daily energetic consumption and who did not want to take part in the group kinetic and home programs and an experimental group B, made of 81 women patients (69%) that benefited both from the diet and the kinetic programs. The kinetic programs were personalized based on the kinetic possibilities of each case. The followed parameters were: BMI, waist girth, weight and which have been tested weekly, but for the study they have been previously estimated (initially, intermediary and finally). Results: The waist evolution reduced from 95 cm to 87 cm, from 120 cm to 99 cm and from 148 cm to 139 cm respectively with 7,5 cm to 24,5% of the patients, with 11 cm to 54,5% of the patients and with 9 cm to 19,5% of the patients. A flexibilization of the people involved in the study has been noticed, a bigger ability in movements both in the gym and in daily life. The overweight BMI that started the study were initially in the percentage of 24,3% and at the end of the study they were 42,6%, the reason being the persons that entered the category from the obesity and extreme obesity studies. The obesity percentage reduced from 54, 4% to 37, 6% at the end of the study. The extreme obesity percentage reduced from 19, 3% to 17,8 %. The weight control is a compulsory step in the obesity monitoring. We obtained: 1. Weight loss 2. 5 kg. (14%) 2. Weight loss. 5-8 kg.(16%) 3. Weight loss 10-12kg. (21%) 4. Weight loss 12-15 kg. (26 %) 5. Weight loss 15-20-kg. (9%) 6. Insignificant fluctuations – statistically (14%). Conclusions. The therapy consists in the optimization of the life style, respectively a low calorie diet and regular physical activity, behavioral therapy, specific medication and motivation. These methods apply differently, starting with the weight loss phase and the maintenance phase, according to the objectives. Introduction. Obesity. Definition. It is a pathological condition caused by the nutrition or endocrine function disorders that disturb the equilibrium between the caloric contribution and the body’s energetic losses, highlighted by excess body fat uniformly or localized in particular body regions. (1) Types of obesity: first appearance; 1. hyper plastic – develops typically in children who are over-nourished. 2. Hypertrophic obesity – develops after the age of 18 -20. By body shape % - low body obesity – increase of the body mass with over 15% more than the ideal body weight; average obesity - increase of the body mass with over 20% more than the ideal body weight; big obesity - increase of the body mass with over 30%. By the fat settlement we have: “gyno type” – the fat accumulates on the belly and hips area, “android type” – the wrist line disappears, “the general type” Etiopathogeny; I. endogenous factors; genetic predisposition 80% of 2 parents, 50% 1 parent, constitutional predisposition II. Exogenous factors: Over-nourishment, 80%-90%). Number of meals, sole meal had in the evening, alcohol consumption, sedentariness, stress, psychical trauma (7,40% for women and 10% for men). Incidence: OMS (1997)”obesity outbreak, USA 36%, Central Europe 15-20%, Eastern Europe 40-50%, Romania 20-25% of the general population. There’s an increase in obesity incidence that goes for women and for those aged over 40. Clinical examination. 1. Weighing 2. Measurements of skin fold thickness 3. Girth 4. BMI – In order to calculate the overweighting and the obesity we can use the IMC (Body Mass

58
Index) or BMI (Body Mass Index) that can be made using the formula: BMI (kg / meters²) = body mass (kg) / height (in meters²). Clinical obesity The internationally BMI values accepted are presented below in
Table 1 (:table 1) the DIAGNOSIS is based on the weight excess. Body Fat Settlement. Peripheral oedema. Effort dyspnoea. Pains in the over-stressed joints. Differential diagnosis: Couching Symptom, Hypothyrodism, Hyperinsulism, Lymphedems,Evolution. 1. The 1st stage is dynamic and characterized by polyphagia and lipogenesis. 2 The 2nd stage is static, the body weight settles and complication soon arrive. Complications:Metabolic, respiratory, osteoarticular, fatty infiltration of the liver, atherosclerosis, hypogonadism. Prognostic;Life expectancy is 10 years shorter than for the rest of the population. ORGANIZING AND DEVELOPING THE RESEARCH The research was realized on a 138 subject lot (women) with weight problems, of various ages and affection degrees, between September 2007 and 2009, in the Lacu Sarat resort and the “SC Fiziter SRL” Medical Rehabilitation Center, Braila. The study lot was divided into 2 sub-lots, that is, a witness lot A, comprising 57 (41%) female patients benefiting only from different forms of diet, still calculated depending on the daily calories consumption, patients who did not want to participate to group and home kinetic programs, and an experimental lot B, comprising 81 (69%) female patients benefiting from both different forms of diet and kinetic programs, established depending on the physical features of each case (graphic I).
1
2
3
Graphic I. The structure of the study lot Within this period we have realized 3 tests on the subjects (initial, intermediary (once a month) and final, after 6 months), observing the evolution of each case and elaborating new exercise programs adjusted to patients’ receptivity to the initially enforced kinetic programs. Lot A has benefited from the same diets: 1) test diet, 2) 1400-calory diet, 3) 1500-calory diet, 4) 1600-calory diet, 5) 1800-calory diet. For the experimental lot we have structured the loss weight program as follows: 14-day metabolic test diet; diet depending on the energy consumption, on age, sex, according to the table; initiation kinetic program; low difficulty kinetic program; average difficulty kinetic program; high difficulty kinetic program; reevaluation after 30 days; short, medium and long term programs, depending on possibilities. Depending on the degree of obesity, on the established objectives and on the personal features, we have recommended the following diets: 1) diets with 1800 kcal less than the previous diet, which can lead to a weight loss of 0,5-1kg / week, 5-10 kg within 3 months (about 5-10% of the initial weight); 2) diets with 1600 kcal less than the previous diet, followed by a weight loss of 1-2 kg / week (about 20% of the initial weight), recommended for increased and extremely increased risk patients; 3) standard low calorie diet of 1500 kcal / day, which requires the recommendation of and the monitoring performed by the doctor
Underweight
< 18.5
normal 18.5-24.9
Overweight 25 - 29.9
Obesity 30 -39.9
Extreme Obesity
> 40
-- 5544,,44%% oobbeessiittyy,, -- 2244,,33%% oovveerrwweeiigghhtt,, -- 1199,,33%% eexxttrreemmee oobbeessiittyy
1
2
A 57 (41%) - diet B 81 (69%) – diet + kineto

59
specialized in diabetes, nutrition, metabolic disorders; highly low calorie diets, 1400 kcal / day, which lead to an obvious and rapid weight loss, but which does not lack side effects, reason for which this type of diet has specific indications, being applied only for a short period of time no longer than 1-2 months, and only under the supervision of specialists in diabetes, nutrition, metabolic disorders. There is no scientific proof with respect to the superiority of various commercial diets or of the dissociated ones, reach in proteins and low in sugars. Moreover, this type of diets can be accompanied by negative effects on the organism, reason for which they are, if so, recommended under the strict supervision of recognized specialists in nutrition.Within the weight maintenance period, the low calorie diet will be able to be complemented with 200-300 kcal, provided that physical exercises are intensified, so the energetic balance remains negative. Kinetic programs have been individualized depending on the kinetic possibilities of each case. Monitored parameters: The monitored parameters were: IMC, girth, weight. The parameters have been tested weekly, but for the study they were estimated (initially, intermediary, and finally).The program also included a study on motivation (initially and finally). Kinetic programs have been individualized depending on the kinetic possibilities of each case. For instance, for beginners, Pilates, Type I low difficulty exercises; for cycles 2-3, Types II, III average and high difficulty exercises (Fig. 2). At the beginning of the treatment cycle, the featured motivation had a percentage of 76,1%; during cycles, it maintains high in people having results in therapy, and it presents monthly fluctuations; motivation decreases progressively in people with unsatisfactory results who present even periods of depression. At the end of the cycles, motivation increases in people who have changed their way of life.EVOLUTION OF GIRTH DIMENSIONS Following the applied treatment, girth dimensions are the first to modify, sometimes in the absence of modifications in weight. The evolution of girth varied between 1,95 cm-12cm, and a decrease of more than 12 cm occurred in 12 cases. Girth reduced from 95 cm to 87 cm, from 120 cm to 99 cm, and from 148 cm to 139 cm, respectively, with 7,5 cm in 24,5% of the patients, with 11 cm in 54,5% of the patients, and with 9 cm in 19,5% of the patients. The flexibilization of people and their increased ability in movement were ascertained, both in gym and in their daily life.
0
5
10
15
20
25
1 2 3
1
2
3
Graphic II. The evolution of girth in the study lot, the witness lot.
The evolution of girth in the witness lot (57): 13 patients (23%) reduced their girth with 2-5 cm, 23 patients (40%) reduced it with 5-7 cm, and 21 (37%) patients reduced it with 7-10 cm. In order to measure overweight and obesity we can use the BMI indicator (Body Mass Index), which is calculated as follows: body mass (kg) / height (m²). BMI values modify the slowest during the evolution of the study lot. For the accuracy of the study, we have verified BMI at the beginning and at the end of each cycle. Statistical reference values are the initial and the final ones. If, initially, upon entering the study, overweight people yielded a percentage of 24,3%, at the end, the percentage mounted up to 42,6% by undertaking obesity and extreme obesity.
0
2
4
6
8
10
12
1 2 3
1
2
3
77 ccmm 2244,,44%%
1111 ccmm 5544,,33%% 99ccmm 1199,,33%%
2233%% 55--77ccmm
3377%%77--1100ccmm 4400%% 22--55ccmm ccmm 1199,,33%%

60
The obesity percentage reduced from 54,4% to 37,6% at the end of the study. The percentage of extreme obesity reduced from 19,3% to 17,8%. There has been abandonment during the study, but other people have entered the study, so the percentage remained the same. Following at least 3-5 cycles within a year, the statistically significant differences as compared to the witness lot upon which only the diet treatment was applied were as shown (graphic II).
0
10
20
30
40
50
60
1 2 3
1
2
3
Graphic II. The evolution of initial and final MBI
Weight control, an imperative step in monitoring obesity We have obtained weight loss gradually, with one or more “weight loss – maintenance” cycles. This strategy of approaching obesity is based on the succession of “weight loss – maintenance” cycles. A cycle of this kind, during the weight loss phase, was meant to decrease weight cu 5-10%, objective realized in 3-6 months, followed by a 3-6-9-month new weight maintenance period. The cycles have been repeated until the established optimum
weight was attained. 1. 2-5kg. (14%) weight loss 2. 5-8 kg. (16%) weight loss 3. 10-12kg. (21%) weight loss 4. 12-15 kg. (26%) weight loss 5. 15-20-kg. (9%) weight loss
6. (14%) statistically insignificant fluctuations Graphic III. The evolution of weight in study lot The study lot benefited from a 3-week test diet, during which 89% of the female patients lost at least 4 kg, subsequently to which the personal sheet of each patient containing the diet type (no. of admitted calories according to the type of effort of each person) was drawn, obtaining the values shown in graphic III. The personal sheet was adapted from weight loss / maintenance cycle to weight loss / maintenance cycle. CONCLUSIONS The basic principles of clinical management of obesity are: 1) Continuous intervention, with short and long term echeloned objectives, periodically and individually adjusted. 2) Close collaboration with the obese person with respect to establishing the objectives and the therapeutic methods according to clinical parameters, monitoring, and periodical evaluation. 3) Gradual weight loss, with one or more “loss – maintenance” cycles. This strategy of approaching obesity is based on the succession of “weight loss – maintenance” cycles. A cycle of this kind consists of a weight loss phase, the objective of which is the decrease of weight with 5-10% attained in 3-6 months, followed by a 6-9-month new weight maintenance period. The cycles can be repeated until the optimum established weight is attained. Long term objectives should be the obtaining of normal weight, that is, the weight corresponding to a BMI < 25 kg/m². In reality, this objective is very difficult to realize and, in particular, to maintain. This is why it is considered that the most realistic long term objective is the maintenance for at least 2 years of the new weight obtained subsequently to the weight loss phase
0
10
20
30
40
50
1 2 3
,42,6 %
1
2
3
17,8%
37,6%
1. BMI 25-29,9 24,3% overweight
2. BMI 30-39,9 obesity 54,5%
3. BMI > 40 extreme obesity 19,3%
0
10
20
30
40
50
1 2 3 4 5 6
1
2
3
4
5
6

61
CURRICULUM VITAE
1. Date biografice Numele: BAŞTIUREA Prenumele: EUGEN
Cetăţenie: română Data şi locul naşterii: 14.04.1959, Galaţi Starea civilă: căsătorit Domiciliul: str. Constructorilor nr. 12, bl. C 2, sc. III, etaj II, ap. 51, Galaţi Profesia şi locul de muncă:
Conferenţiar universitar doctor la Universitatea „Dunărea de Jos” din Galaţi, Facultatea de Educaţie Fizică şi Sport, Catedra de Jocuri sportive şi educaţie fizică
2. Studii
Ciclul liceal Liceul Industrial Nr. 4, Galaţi (1974-1978)
Studii universitare Universitatea din Galaţi, Facultatea de Învăţământ Pedagogic, Specializarea: Educaţie fizică (1980-1983)
Academia Naţională de Educaţie Fizică şi Sport, Facultatea de Educaţie Fizică, Bucureşti (1990-1992)
3. Specializări, grade didactice şi titluri ştiin ţifice Profesor de educaţie fizică şi sport – definitivat (ANEFS Bucureşti, 1986) Antrenor cu specializarea handbal – categoria I (CNFPA Bucureşti, 2008) Doctor în pedagogie - INEFS Chişinău, Republica Moldova (2004) Atestat doctor în domeniul educaţie fizică şi sport – Ministerul Educaţiei şi Cercetării (2005) 4. Contribuţii ştiin ţifice Teză de doctorat = 1 Cărţi publicate în edituri naţionale şi internaţionale = 5 Cursuri şi caiete de lucrări practice publicate = 6 Brevet de invenţie = 1 Proiecte/contracte de cercetare (responsabil/membru) = 4 Articole ştiinţifice publicate în reviste recunoscute de CNCSIS = 17 Articole ştiinţifice publicate în reviste nerecunoscute de CNCSIS = 7 Lucrări publicate în volumul unor conferinţe ştiinţifice naţionale şi internaţionale = 27 Citări în cărţi (capitole din carţi, bibliografie) = 16 Citări în teze de doctorat şi habilitat (capitole din teză, bibliografie) = 16 Colectivul redacţional al unor reviste şi volume ştiinţifice = 15 Comisia de concurs a cadrelor didactice din învăţământul universitar = 7 Comisia de finalizare a studiilor de învăţământ superior, domeniu licenţă = 11 Lucrări de gradul I îndrumate = 16 Lucrări de licenţă şi disertaţie îndrumate = 106 5. Responsabilităţi
Secretar ştiinţic al facultăţii (din febr. 2007) Membru în Consiliului Profesoral al facultăţii (din 1997)

62
Director program de studiu, specializarea “Educaţie fizică şi management în sport” (2002-2005) 6. Realizări specifice domeniului Locul II la Campionatul Naţional de handbal juniori I, Suceava, 1978 (sportiv) Locul II la Campionatul Naţional de handbal juniori III, Ploieşti, 1992 (antrenor) Locul II la Campionatul Naţional Universitar de handbal masculin, Timişoara, 1998 (profesor FEFS) Promovarea echipei de handbal masculin CSU Galaţi în Liga Naţională, 2000 (antrenor principal) Calificarea echipei de handbal masculin CSU Galaţi în turul II al Challenge Cup, 2001 Promovarea echipei de handbal feminin Oţelul Galaţi în Divizia A, Bistriţa, 1993 (antrenor principal) Antrenor secund al lotului naţional universitar de handbal (2000-2001) Antrenor secund al lotului naţional de tineret (2001, 2003) 7. Premii/medalii ştiin ţifice Medalie de argint obţinută la Festivalul Internaţional de Invenţii şi Tehnologii, pentru „Metodă şi aparat pentru determinarea dezechilibrelor musculare la nivelul torsului”, ediţia a VI-a, Suzhou, China, 2008 Premiul de excelenţă în inovare primit din partea Fundaţiei pentru Promovarea şi Dezvoltarea Proprietăţii Intelectuale, Galaţi, 2008 Premiul IT&C EXPO 2008 acordat de Camera de Comerţ, Industrie şi Agricultură Galaţi pentru „Aparat pentru determinarea dezechilibrelor musculare prezente la nivelul trunchiului”, ediţia a VIII-a, Galaţi, 2008