Necrobiosis lipoidica diabeticorum: Response to pentoxiphylline
4
Click here to load reader
Transcript of Necrobiosis lipoidica diabeticorum: Response to pentoxiphylline

(J. Endocrinol. Invest. 26: 1037-1040, 2003) ©2003, Editrice Kurtis.
1037
ABSTRACT. Necrobiosis lipoidica diabeticorum(NLD) is a condition that can be physically andpsychologically distressing. Angiopathy leadingto thrombosis and occlusion of the cutaneousvessels has been implicated in its etiology.Pentoxiphylline is a hemorrheological agent thatimproves blood flow and decreases red cell andplatelet aggregation. Based on these data, aimof our study was to report clinical course of a20-yr-old diabetic woman with NLD during ther-apy with Pentoxiphylline 400 mg 3 times daily.After 1 month of therapy, the lesions stoppedenlarging. After 3 months, the lesions showed
initial signs of healing. At 6-month follow-up,there was near resolution of the lesions. The pa-tient continued therapy and remained in remis-sion at 2-yr follow-up. This improvement relievedpsychological stress on the patient. No side ef-fects of treatment were reported. In conclusion, patients with NLD may benefitfrom treatment with pentoxiphylline. We rec-ommend therapy with 400 mg 3 times daily.The drug should be continued for at least 6months.(J. Endocrinol. Invest. 26: 1037-1040, 2003)©2003, Editrice Kurtis
INTRODUCTION
Necrobiosis lipoidica diabeticorum (NLD) is a char-acteristic skin lesion that occurs in about 0.3% of thediabetics (1). This entity was first described in 1929by Oppenheim (2). Although the exact pathophysi-ology remains unknown, vasculopathy of the der-mal vessels with resulting inflammation and obliter-ation is present in the majority of these lesions (3).These lesions may be associated with pain and pru-ritis and ulceration is seen in 35% of the patients (4).Cosmetic disfigurement may be the most distressingelement in some patients. Pentoxiphylline, a hem-orrheological agent, has been used for decades inthe treatment of intermittent claudication and dia-betic foot ulcers (5). Earlier reports have shown pen-toxiphylline to be effective in the treatment of ul-
cers within the NLD lesion (6, 7). We report a pa-tient with Type 1 diabetes mellitus with lesions ofNLD on both her shins who showed an excellent re-sponse to pentoxiphylline.
CASE REPORT
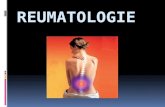
A 20-yr-old woman with a 15-yr history of Type 1 di-abetes mellitus presented for the evaluation of NLDon both her shins. The lesions initially appeared onher right shin 4 yr ago in form of annular papuleswhich over time coalesced to form a 16x4 cm serpinginous lesion. One yr later, annular lesions al-so appeared on her left shin, which were progres-sively enlarging (Fig. 1A and 1B). There was no his-tory of trauma to the legs. The patient did not reportpruritis, pain or ulceration. Her glycemic control hadbeen excellent over the years with glycosylatedhemoglobin ranging between 5-6% and she was freefrom any of the microvascular or macrovascular com-plications. The patient was in significant psychologi-cal distress secondary to the lesions and could notengage in several sports like swimming and athlet-ics and other recreational activities. The rest of herphysical exam was normal. The patient was startedon pentoxiphylline 400 mg 3 times daily. One month
Key-words: Necrobiosis, coagulative necrosis, diabetes, Pentoxiphylline,hematinics.
Correspondence: Shehzad Basaria, M.D., Division of Endocrinology andMetabolism, John Hopkins University Bayview Medical Center, 4940Eastern Avenue, B-114, Baltimore, MD-21224.
E-mail: [email protected]
Accepted July 17, 2003.
CASE REPORT
Necrobiosis lipoidica diabeticorum: Response topentoxiphylline
S. Basaria1 and M. Braga-Basaria2
1Division of Endocrinology and Metabolism, John Hopkins University Bayview Medical Center,Baltimore, USA; 2MD, Baltimore, USA

NDL therapy with pentoxiphylline
1038
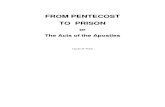
into therapy, the patient noticed that the lesions hadstopped enlarging and within 3 months, the lesionsshowed initial signs of healing. At 6-month follow-upvisit, there was near resolution of the lesions bilater-ally with active yellowish-brown lesions replaced bysmooth shiny atrophic scars (Fig. 2A and 2B). This im-provement eased much of the psychological stresson the patient as she engaged in activities and sports
that required wearing shorts. There were no side ef-fects secondary to pentoxiphylline like nausea, dizzi-ness, palpitations or bleeding. The patient was givenan option to discontinue pentoxiphylline and watch
Fig. 1 - A) A 16x4 cm serpinginous lesion on the right shin. Twoannular lesions on the left shin. Note the small brownish papulesuperior to the upper annular lesion (this is the initial lesion ofNLD). B) Magnified view of the serpinginous lesion. Note thecentral yellowish core with telangiectatic vessels and an activereddish-brown border.
Fig. 2 - Near resolution of lesions on both the extremities 6months into therapy. A) Annular lesions on the left shin. B)Serpinginous lesion on the right shin.
A A
B B

S. Basaria and M. Braga-Basaria
for recurrence. However, the patient continued tak-ing the current dose of pentoxiphylline and at 2-yrfollow-up, she remained in remission.
DISCUSSION
NLD is a rare condition affecting 0.3% of diabet-ics. It is 3-5 times more common in women (4).The age of onset is usually in the third or fourthdecade, however, NLD has been observed frominfancy to the tenth decade of life (1). There is nocorrelation between the development of these le-sions and the degree of glycemic control. In 60%of the patients, the diagnosis of diabetes ante-dates the onset of NLD, in 25% of the patients,diabetes and NLD appear concomitantly, and inthe remaining 15%, NLD antedates the diagnosisof clinical diabetes (1). Typically, the patients pre-sent with bilateral involvement of the pretibialarea, however, upper extremities, abdomen,popliteal area, face and scalp have also been in-volved. In some cases there is a history of pre-ceding trauma to the region where the lesions ul-timately develop.The earliest lesion of NLD is a reddish-brownpapule which spreads centrifugally and coalesceswith other such lesions to form large plaques. Thetypical lesion is an irregular round or serpinginousplaque with a yellowish atrophic central area withprominent telangiectatic vessels and an active ele-vated reddish-brown border (4).Recent dermatopathologic and immunopatholog-ic studies have shown vasculopathy of the dermalvessels (3). Deposition of immunoglobulins andcomponents of complement pathway (such as C3)have been documented in the vessel wall. Initiallythere is swelling of the endothelial cells and thick-ening of the basement membrane followed by fib-rinoid necrosis, and finally thrombosis and evencomplete obliteration of the vascular lumen (8).Low blood flow to the NLD lesion is further sup-ported by a low transcutaneous oxygen gradientover NLD lesions (7). Furthermore, diabetes is aprothrombotic state with increased platelet ag-gregation and impaired fibrinolysis, which may fur-ther impede blood flow to the skin (5). Generally, NLD is a difficult condition to treat. Thereis no standard medical therapy available for thisdermopathy. Steroid injections are helpful eitherwhen the lesion is at an early stage or in the treat-ment of a nodule within the lesion (4). Furthermore,surgical treatment with split skin grafting is suc-cessful only if there is a deep excision of the lesion(sometimes up to the periosteum) along with liga-tion of the perforating blood vessels (9, 10).
Superficial excision and grafting is associated witha high incidence of recurrence. Since vasculopathy is seen in virtually all cases ofNLD, it is logical to use agents that improveblood flow and prevent thrombosis. Earlier re-ports with ticlopidine, though showed improve-ment of NLD in the majority of the patients, weremarred by the lethal side effect of agranulocyto-sis in a significant number of patients (11). Aspirinand dipyridamole have been used in combina-tion for NLD, however, they mainly resulted inthe improvement of ulcerated lesions (12, 13).Furthermore, in one study the response rate ofpatients on this combination was no differentthan placebo (14). Pentoxiphylline is a hemorrheologic agent that isa xanthine derivative. It acts by decreasing plas-ma viscosity (by decreasing fibrinogen concentra-tion), red and white cell deformability (by increas-ing ATP concentrations within cells and hence im-proving their elasticity) and inhibition of red celland platelet aggregation (by increasing prostacy-clin) (5, 15). Since flow through small cutaneousvessels (in the shin area) is dependent on the de-formability of both red and white blood cells (5),this gives pentoxiphylline an edge over otheragents. Pentoxiphylline has been used extensive-ly in the past for the treatment of ischemic leg ul-cers and peripheral vascular disease in diabeticpatients with reasonable success (5). The usualtreatment dose is 400 mg 3 times daily.Only 2 earlier reports (1 patient each) have success-fully used pentoxiphylline in the treatment of ulcerat-ed NLD lesions (6, 7). Although the ulcers were re-ported to show complete healing in the 2 patients, in1 report, the NLD lesion was still visible at 10-monthfollow-up (6), whereas in the other there was no men-tion of the description of the lesion at 3-month fol-low-up (7). To the best of our knowledge, this is thefirst report in the English literature where pentoxi-phylline was used in an asymptomatic patient withnon-ulcerative lesions with significant success.Furthermore, at 2-yr follow-up (the longest reportedto date), the lesions remained in remission and therewere no side effects as a result of therapy.Based on the positive efficacy data (though anec-dotal), low cost and relative safety of the drug, werecommend that patients presenting with NLDshould be given a trial of pentoxiphylline at thedose of 400 mg 3 times daily. The drug should becontinued for at least 6 months. A positive responsewill be gratifying for both the patient and the physi-cian. Double blind, placebo controlled trials areneeded to evaluate the efficacy of this agent in alarge group of patients.
1039

NDL therapy with pentoxiphylline
1040
REFERENCES1. Muller SA, Winkelmann RK. Necrobiosis lipoidica diabeti-
corum. A clinical and pathological investigation of 171 cas-es. Arch Dermatol 1966, 93: 272-81.
2. Oppenheim M. Eigentumlich disseminierte degenerationdes bindegewebes der haut bie einem diabetiker. Z Hautkr1929, 32: 179.
3. Quimby SR, Muller SA, Schroeter AL. The cutaneous im-munopathology of necrobiosis lipoidica diabeticorum.Arch Dermatol 1988, 124: 1364-71.
4. Lowitt MH, Dover JS. Necrobiosis lipoidica. J Am AcadDermatol 1991, 25: 735-48.
5. Campbell RK. Clinical update on pentoxiphylline therapyfor diabetes-induced peripheral vascular disease. AnnPharmacother 1993, 27: 1099-105.
6. Littler CM, Tschen EH. Pentoxiphylline for necrobiosis lipoidi-ca diabeticorum. J Am Acad Dermatol 1987, 17: 314-6.
7. Noz KC, Korstanje MJ, Vermeer BJ. Ulcerating necrobiosislipoidica effectively treated with pentoxiphylline. Clin ExpDermatol 1993, 18: 78-9.
8. Laukkanen A, Fraki JE, Vaatainen N, Korhonen T, NaukkarinenA. Necrobiosis lipoidica: clinical and immunofluorescent study.Dermatologica 1986, 172: 89-92.
9. Dubin BJ, Kaplan EN. The surgical treatment of necro-biosis lipoidica diabeticorum. Plast Reconstr Surg 1977,60: 421-8.
10. Marr TJ, Traisman HS, Griffith BH, Schafer MA.Necrobiosis lipoidica diabeticorum in a juvenile diabet-ic: treatment by excision and skin grafting. Cutis 1977,19: 348-50.
11. Rhodes EL. Necrobiosis lipoidica treated with ticlopidine.Acta Derm Venereol 1986, 66: 458.
12. Fjellner B. Treatment of diabetic necrobiosis with aspirin ordipyridamole. N Engl J Med 1978, 299: 1366.
13. Heng MC, Song MK, Heng MK. Healing of necrobiotic ul-cers with antiplatelet therapy. Correlation with plasmathromboxane levels. Int J Dermatol 1989, 28: 195-7.
14. Statham B, Finlay AY, Marks R. A randomized double blindcomparison of an aspirin dipyridamole combination ver-sus a placebo in the treatment of necrobiosis lipoidica.Acta Derm Venereol 1981, 61: 270-1.
15. Hammerschmidt DE, Kotasek D, McCarthy T, Huh PW,Freyburger G, Vercellotti GM. Pentoxiphylline inhibitsgranulocyte and platelet function, including granulocytepriming by platelet activating factor. J Lab Clin Med1988, 112: 254-63.