Rom J Morphol Embryol 2011, 52(3):947–949 R J M E CASE … · 1.5 cm postero-lateral to the...
3
Rom J Morphol Embryol 2011, 52(3):947–949 CASE REPORTS The lateral incisive canals of the adult hard palate – aberrant anatomy of a minor form of clefting? M. VÂLCU 1) , M. C. RUSU 2) , VIVIAN MIHAELA ŞENDROIU 3) , ANDREEA CRISTIANA DIDILESCU 4) 1) Clinic of Plastic Surgery and Reconstructive Microsurgery, Bucharest Emergency Hospital 2) Discipline of Anatomy, Faculty of Dental Medicine “Carol Davila” University of Medicine and Pharmacy, Bucharest 3) Vivclinique, Bucharest 4) Discipline of Embryology, Faculty of Dental Medicine, “Carol Davila” University of Medicine and Pharmacy, Bucharest Abstract Except the oral clefts and their associated dental development disturbances, no other discrete morphologies are reported in the literature as related to altered fusions of the fetal maxilla and premaxilla. We report here two cases related by the persistence in adult of an aberrant canal at the fusion site of the fetal premaxilla and maxilla. The first case presents an anastomosis of the superior anterior alveolar and greater palatine nerves, encountered during the dissection of a human adult male cadaver; that anastomosis, bilaterally present, projected on the aforementioned fusion site and traversed the hard palate to continue within the maxillary sinus wall. The second case evidenced on CT the unilateral presence of aberrant lateral incisive canals (LIC) at the level of the fetal premaxilla and maxilla fusion site; those canals, external (1.5 mm diameter) and internal (1.07 mm diameter), were corresponding as location to that one traversed by the aberrant anastomosis in the first case. Both LIC opened inferiorly but not superiorly, rather seeming to communicate with the bony canals within the nasal fossa floor at that level. We consider that such aberrant canals and nerves may represent very rare forms of clefting, previously undescribed; the possible anastomoses of the superior anterior alveolar and greater palatine nerves can be altered during a Le Fort I fracture and may be the morphology that can explain aberrant clinical nervous distributions at the level of the upper dentoalveolar arch and hard palate. Keywords: palate, cleft, alveolar nerve, palatine nerve. Introduction The external human face develops between the 4 th and 10 th weeks of embryonic development. The primary palate, formed in this period by fusion/merging of the medial nasal prominences, is the primordium of the premaxillary bone (anterior to the incisive fossa). Subsequently, between 6 th and 12 th embryonic/fetal weeks the secondary palate (primordium of the hard and soft parts of the palate) is formed as the result of fusion between the nasal septum and the palatal processes growing from the internal aspects of the maxillary prominences [1]. Each merging and fusion site may be a potential place for development of a partial/complete cleft. In the development of the human craniofacial morphology, a special part of the palate maxilla nose region – the premaxillary bone (os incisivum, os intermaxillare, os Goethei, Zwischenkiefer) – plays an essential role [2]. The distal landmarks of the premaxillary bone at palatal level are the incisive foramen and suture, the later being first described by Goethe [3]. Except the oral clefts and the associated dental development disturbances [4], no other aberrant discrete morphologies are reported in the literature as related to altered fusions of the fetal maxilla and premaxilla. Abbreviations LIC – lateral incisive canal; IF – incisive fossa; OC – oral cavity; NF – nasal fossa; AC – alveolar crest; SAAN – superior anterior alveolar nerve; GPN – greater palatine nerve. Materials, Methods and Results Case No. 1 At a routine dissection during the teaching process, a human adult male cadaver dissection of the oral cavity was initiated, with an anterior approach. On each side (bilateral symmetry), at the level of the anterior palatine region, at an average distance of 1.5 cm postero-lateral to the incisive foramen, two nerves were found entering the hard palate, projected each at the level of the interval between the upper canine and upper lateral incisor teeth (Figure 1A). R J M E Romanian Journal of Morphology & Embryology http://www.rjme.ro/
-
Upload
nguyendieu -
Category
Documents
-
view
219 -
download
0
Transcript of Rom J Morphol Embryol 2011, 52(3):947–949 R J M E CASE … · 1.5 cm postero-lateral to the...

Rom J Morphol Embryol 2011, 52(3):947–949
CCAASSEE RREEPPOORRTTSS
The lateral incisive canals of the adult hard palate – aberrant anatomy of
a minor form of clefting? M. VÂLCU1), M. C. RUSU2), VIVIAN MIHAELA ŞENDROIU3),
ANDREEA CRISTIANA DIDILESCU4)
1)Clinic of Plastic Surgery and Reconstructive Microsurgery, Bucharest Emergency Hospital
2)Discipline of Anatomy, Faculty of Dental Medicine “Carol Davila” University of Medicine and Pharmacy, Bucharest
3)Vivclinique, Bucharest 4)Discipline of Embryology, Faculty of Dental Medicine,
“Carol Davila” University of Medicine and Pharmacy, Bucharest
Abstract Except the oral clefts and their associated dental development disturbances, no other discrete morphologies are reported in the literature as related to altered fusions of the fetal maxilla and premaxilla. We report here two cases related by the persistence in adult of an aberrant canal at the fusion site of the fetal premaxilla and maxilla. The first case presents an anastomosis of the superior anterior alveolar and greater palatine nerves, encountered during the dissection of a human adult male cadaver; that anastomosis, bilaterally present, projected on the aforementioned fusion site and traversed the hard palate to continue within the maxillary sinus wall. The second case evidenced on CT the unilateral presence of aberrant lateral incisive canals (LIC) at the level of the fetal premaxilla and maxilla fusion site; those canals, external (1.5 mm diameter) and internal (1.07 mm diameter), were corresponding as location to that one traversed by the aberrant anastomosis in the first case. Both LIC opened inferiorly but not superiorly, rather seeming to communicate with the bony canals within the nasal fossa floor at that level. We consider that such aberrant canals and nerves may represent very rare forms of clefting, previously undescribed; the possible anastomoses of the superior anterior alveolar and greater palatine nerves can be altered during a Le Fort I fracture and may be the morphology that can explain aberrant clinical nervous distributions at the level of the upper dentoalveolar arch and hard palate. Keywords: palate, cleft, alveolar nerve, palatine nerve.
Introduction
The external human face develops between the 4th and 10th weeks of embryonic development. The primary palate, formed in this period by fusion/merging of the medial nasal prominences, is the primordium of the premaxillary bone (anterior to the incisive fossa). Subsequently, between 6th and 12th embryonic/fetal weeks the secondary palate (primordium of the hard and soft parts of the palate) is formed as the result of fusion between the nasal septum and the palatal processes growing from the internal aspects of the maxillary prominences [1]. Each merging and fusion site may be a potential place for development of a partial/complete cleft.
In the development of the human craniofacial morphology, a special part of the palate maxilla nose region – the premaxillary bone (os incisivum, os intermaxillare, os Goethei, Zwischenkiefer) – plays an essential role [2]. The distal landmarks of the premaxillary bone at palatal level are the incisive foramen and suture, the later being first described by Goethe [3].
Except the oral clefts and the associated dental development disturbances [4], no other aberrant discrete
morphologies are reported in the literature as related to altered fusions of the fetal maxilla and premaxilla.
Abbreviations
LIC – lateral incisive canal; IF – incisive fossa; OC – oral cavity; NF – nasal fossa; AC – alveolar crest; SAAN – superior anterior alveolar nerve; GPN – greater palatine nerve.
Materials, Methods and Results
Case No. 1 At a routine dissection during the teaching process, a
human adult male cadaver dissection of the oral cavity was initiated, with an anterior approach.
On each side (bilateral symmetry), at the level of the anterior palatine region, at an average distance of 1.5 cm postero-lateral to the incisive foramen, two nerves were found entering the hard palate, projected each at the level of the interval between the upper canine and upper lateral incisor teeth (Figure 1A).
R J M ERomanian Journal of
Morphology & Embryologyhttp://www.rjme.ro/

M. Vâlcu et al.
948
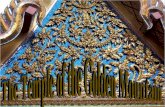
After the certain evidence of the SAAN and GPN, direct anastomoses of these nerves have been observed. The respective anastomoses traversed the hard palate and further arched superior and posterior within the anterior wall of the maxillary sinus, to reach the SAAN lodged within the sinuous canal of Wood Jones (Figure 1B).
Figure 1 – A. Dissection of the anterior palatine region at a human adult cadaver, formalized; anterior view. While detaching the palatal mucosa (forcepses), the incisive foramen (arrowhead) was evidenced. Bilaterally symmetrical, at the level of the incisive suture projection line, nerves were entering the hard palate (arrows). B. The dissection was continued and an anastomosis was demonstrated (thick arrows) between the superior anterior alveolar nerve and the greater palatine nerve (antero-lateral view). 1. Infraorbital foramen; 2. Right nostril; 3. Nasopalatine nerve; 4. First upper premolar; 5. Greater palatine nerve; 6. Anterior palatine mucosa.
Case No. 2
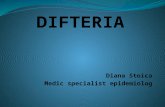
At a human female adult patient, CT scans of the maxilla were performed in order to evaluate the parameters of the available bone for the dental medical approach. As we had in mind the results of the previously reported case, we looked for, and identified on the left side, the presence in the hard palate at the level of the interval between the upper lateral incisor and canine teeth of two aberrant canals, external and
internal, that we named lateral incisive canals (LIC) (Figure 2). These canals were located within a bony wall of 8.5 mm thickness and were only opened inferiorly, in the palatine region. Superior, towards the nasal fossa, the LIC were closed by the cortical nasal plate. The external LIC, as demonstrated on the oblique slices (Figure 2A), was divided superiorly to communicate with canals passing sagittally within the nasal fossa floor and could only correspond to those canals for the branches of the infraorbital nerve, well known in anatomy. The internal LIC was narrower than the external one (Figure 2B). Measurements were performed and the results are presented in Figure 2C. As it can be observed from Figure 2D, on coronal slices, the true incisive canal and the external LIA can be easily distinguished. Unfortunately, the imagistic method could not evaluate the contents of those canals.
Figure 2 – Computer tomographs of the maxilla at an adult female patient, demonstrating aberrant lateral incisive canals projecting in the interval between the upper lateral incisor and canine locations. A. Serial oblique slices first identified an outer lateral incisive canal (1) that superiorly divided to communicate with two distinctive canals (*) running beneath the cortical plate of the nasal fossa (NF) floor. B. Further oblique slicing led to the evidence of both lateral incisive canals, external (1) and internal (2), both opened inferiorly and closed superiorly, to the nasal fossa. C. Diagram of the axial CT that identified three distinctive incisive canals opened at the level of the incisive fossa (IF) of the hard palate, left, right and posterior, but also the two aberrant lateral incisive canals, external (1) and internal (2); the measurements are in millimeters. D. Coronal slice evidencing the incisive canal proper opened at the level of the incisive fossa (IF) and the aberrant external lateral incisive canal (1). OC: Oral cavity; AC: Alveolar crest.
Discussion
To date, the textbooks of embryology illustrate the premaxillary bone in relation to the facial and palatine development in a lingual view. Unfortunately, the

The lateral incisive canals of the adult hard palate – aberrant anatomy of a minor form of clefting?
949
frontal, as well as the nasal processes of premaxilla are ignored [2] and so, the projection of the incisive suture into the facial side of the adult maxilla is ignored. That suture projects in the interval between the upper lateral incisor and canine teeth and continues towards the frontal process of the maxillary bone, dividing it into two parts, an anterior one, premaxilla-derived, and a posterior one, maxilla-derived.
The course of the direct anastomosis of the SAAN and GPN reported here (Case No. 1) corresponds to the fusion line of the maxillary and medial nasal prominences that evolve during development [5] and further, to the fusion line of the fetal maxilla and premaxilla. The respective topography and the bilateral symmetry of the anastomosis are strongly suggestive for an uncommon event that allowed its presence; the location of that anastomosis at a fusion site gives a developmental sense to the aberration.
The second case reported here depicts aberrant palatal canals – lateral incisive canals, also located in adult at the level of the fetal premaxilla – maxilla junction, strongly corresponding topographically to that canal traversed by the anastomosis of the SAAN and GPN.
Both cases have in common the topographical location at the junction of two developmentally distinctive parts of the adult maxilla and led us to consider these aberrations although rare, as being possible minor forms of clefting, similar to the supernumerary lateral incisors [2].
Both cases presented here relate to a morphological junctional area. The primordial craniofacial structures undergo complex morphogenetic processes as they merge and fuse in a time and space dependent fashion, and it was recently suggested a dual embryonic origin of the incisors in minipigs with the first and second incisors originating from the frontonasal prominence but the third incisor forming from tissues derived from the maxillary prominence [6]. It was also shown that cleft lip-liable strains of mice have a narrower window in development in which a robust mesenchymal bridge between the facial prominences must form, thus increasing the liability to cleft lip [7]. However, there are studies describing a single ossification center for the maxilla and claiming that the anterior part of the maxilla in man is very limited during growth and thus cannot justify the term of premaxilla [8, 9]. It is so reasonable to consider such minor defects as those reported here have a limited developmental period of establishment.
With its topography, the aberrant anastomosis of the SAAN and GPN may be intercepted by a Le Fort I fracture that crosses the floor of the nose, pyriform
aperture, canine fossa, and lateral wall of the maxilla, resulting in separation of the palate from the maxilla [10].
Conclusions
The anastomosis of the anterior superior alveolar and greater palatine nerves can be the rare anatomical substrate that supports the crossed distribution of these nerves and the aberrant effects of their anesthesia. Further clinical studies should be conducted to evidence such crossed distribution that from now on has a first time evidenced morphological substrate.
Acknowledgements Researches were supported by: (1) Sectoral Operational Programme Human
Resources Development (SOP HRD), financed from the European Social Fund and by the Romanian Government under the contract number POSDRU/89/ 1.5/S/60782 (author #1).
(2) CNCSIS–UEFISCDI (Executive Unit for Financing University Higher Education, Research, Development and Innovation) Grant 317/2007 (author #2).
References [1] Moore KL, Persaud TVN, The developing human: clinically
oriented embryology, 8th edition, Saunders Elsevier, Philadelphia, 2008, 179–187.
[2] Barteczko K, Jacob M, A re-evaluation of the premaxillary bone in humans, Anat Embryol (Berl), 2004, 207(6):417–437.
[3] Jordan RE, Kraus BS, Neptune CM, Dental abnormalities associated with cleft lip and/or palate, Cleft Palate J, 1966, 3:22–55.
[4] Menezes R, Vieira AR, Dental anomalies as part of the cleft spectrum, Cleft Palate Craniofac J, 2008, 45(4):414–419.
[5] Sadler TW, Langman’s medical embryology, 7th edition, Williams & Wilkins, Baltimore, 1995, 333–335.
[6] Putnová I, Odehnalová S, Horák V, Stehlík L, Míšek I, Lozanoff S, Buchtová M, Comparative morphology of normal and cleft minipigs demonstrates dual origin of incisors, Arch Oral Biol, 2011 Jul 11. [Epub ahead of print]
[7] Wang KY, Juriloff DM, Diewert VM, Deficient and delayed primary palatal fusion and mesenchymal bridge formation in cleft lip-liable strains of mice, J Craniofac Genet Dev Biol, 1995, 15(3):99–116.
[8] Vacher C, Onolfo JP, Lézy JP, Copin H, The growth of the maxilla in humans. What place for the premaxilla? Rev Stomatol Chir Maxillofac, 2001, 102(3–4):153–158.
[9] Vacher C, Copin H, Sakka M, Maxillary ossification in a series of six human embryos and fetuses aged from 9 to 12 weeks of amenorrhea: clinical implications, Surg Radiol Anat, 1999, 21(4):261–266.
[10] Shah AR, Valvasorri GE, Roure RM, Le Fort fractures. eMedicine: Radiology: Head and Neck Section, 2006, http:// www.emedicine.com/radio/TOPIC385.HTM.
Corresponding author Mugurel Constantin Rusu, Senior Lecturer, MD, PhD, Discipline of Anatomy and Embryology, Faculty of Dental Medicine, “Carol Davila” University of Medicine and Pharmacy, 8 Eroilor Sanitari Avenue, 050474 Bucharest, Romania; Phone +40722–363 705, e-mail: [email protected]
Received: June 1st, 2011
Accepted: August 10th, 2011