Microzonuloscopy
9
Click here to load reader
Transcript of Microzonuloscopy

BLOW-OUT FRACTURE OF THE ORBIT 845
rim. This was best shown on laminography (fig. 3). SUMMARY Surgical exploration was carried out six days
after the initial injury and direct visualization of the Blow-out f racture of the orb i t is dis-orbital floor was obtained. As expected the orbital cussed wi th emphas is upon the impor tance rim was intact but there was a large depressed frac- .,<· ___I,T J : ~ „ _ „ „ : „ „ „ A *U~ J - C ·*. Λ c ture of the orbital floor which had incarcerated the ° f e a r l y diagnosis and the definite need for inferior rectus and orbital fat. The orbital tissues c l ° s e collaboration between clinician and were freed without difficulty. The otolaryngologist, radiologist. Two typical case histories have utilizing the Caldwell-Luc method, evacuated a b e e n p r e Sented. In both instances freeing large amount of hemorrhagic material from the , . . . ö
antrum. A water-filled balloon was then placed in the o f t h e incarcerated inferior rectus muscle antrum via an antrostomy and the proper amount was needed, and one case required the in-of support was accurately determined by direct s e r t i o n of a water balloon in t h e a n t r u m for visualization of the fracture site. The patient had , , . c ., , ., , „ an uneventful postoperative period, the diplopia dis- a d e q u a t e suppor t of the orbi tal floor. appeared and normal muscle balance resulted. 600 West Main Street
REFERENCES 1. Erdbrink, W. L., Edwards, J. E., Cros, W. W., Johnson, H. S., Cooke, S. L., and Richmond, R. W.:
Orbital fractures. Arch. Ophth., 61:55, 1959. 2. Smith, B., and Regan, W. F., Jr.: Blow-out fractures of orbit: Mechanism and correction of internal
orbital fracture. Am. J. Ophth., 44:733, 1957. 3. Smith, B., and Converse, J. M.: Early treatment of orbital floor fractures. Tr. Am. Acad. Ophth., 61:
602, 1957. 4. Converse, J. M., and Smith, B.: Reconstruction of the floor of the orbit by bone grafts. Arch. Ophth.,
44:1, 1950. 5. Callahan, A.: Symposium: Malunited fractures of the zygoma: Bony depressions particularly depres
sion of the floor of the orbit. Tr. Am. Acad. Ophth., 57:875, 1953. 6. Erdbrink, W. L.: Blow-out fracture of the orbit. Am. Jour. Ophth., 49:1037, 1960. 7. Lewin, J. R., Rhodes, D. H., Jr., and Prosek, E. J.: Roentgenologic manifestations of fracture of the
orbit floor (blow-out fracture). Am. J. Roentgenol., 83:629, 1960. 8. Pfeiffer, R. L.: Traumatic enophthalmos. Arch. Ophth., 30:718, 1943. 9. Anthony, D. H.: Diagnosis and surgical treatment of fractures of the orbit. Tr. Am. Acad. Ophth.,
56:580, 1952. 10. McCoy, F. J.: Management of the orbit in facial fractures. Plastic & Reconst. Surg., 19:236, 1957. 11. Quereau, J. V. D., and Souders, P. F.: Teflon implant to elevate the eye in depressed fracture of the
orbit. Arch. Ophth., 55:685, 1956. 12. Rubin, W.: A note on management of recent fractures of the zygoma involving floor of the orbit.
Am. J. Ophth., 39:183, 1955. 13. Bleeker, G. M., and Ommen, B. Van: Early treatment of orbital fractures. Ophthalmologica, 138:
40, 1949. 14. Pelzer, R. H., and Garvin, W. J. : Controlled correction of diplopia and eye muscle imbalance in orbital
and zygomatic fractures. Am. J. Surg., 96:735, 1958.
MICROZONULOSCOPY ;
I N KRUKENBERG SPINDLES AND ANNULAR PIGMENT RINGS OF THE LENS
EMANUEL ROSEN, M.D. Newark, New Jersey
The combination of Krukenberg spindle nificantly to the accurate localization and and pigment ring upon the posterior lens possible source of origin of this pigmentary capsule, while not a new entity, has been de- phenomenon, the following case reports seem scribed with infrequency since its first bio- of interest as do some helpful hints which microscopic interpretation in 1924. With im- this method of examination offers. proved methods of examination adding sig- Microzonuloscopy as a biomicroscopic

846 EMANUEL ROSEN
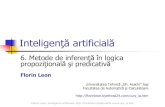
Fig. 1 (Rosen). Findings in Case 1.
KEY TO LETTERING ON ALL ILLUSTRATIONS S.P., superior plica I.P., inferior plica P.W.L., pigmented Wieger's ligament W. L., Wieger's ligament P.Z.F., posterior zonular fibers L.E., lens edge A.H., anterior hyaloid C.P., ciliary process p., pigment H., hooklet (of Busacca) Z.S.R., zone of specular reflection R.Z.C., retrozonular canal.
technique has been described in a previous paper.12 Briefly, it is an unorthodox method of biomicroscopy wherein, by tilting the patient's head and eye downward at almost a 70-degree angulation, the beam of light derived from the slitlamp is enabled to transect the perilenticular area, the zonular fibers, the hyaloid membrane, the inferior plica and the ciliary processes without the necessity of gonioscopy.
The facility and rapidity of performance of this method appears to add still another routine investigative arm to every office examination, either in children or in adults, so that rarely visualized abnormalities may now become daily observations of infinite value. The frequent employment of this procedure during the past few months has helped to uncover several cases of the syndrome of the Krukenberg spindles and annular pigment rings of the lens, the incomplete types of which would not have been suspected if this technique had not been employed.
Obviously, when the syndrome is high
lighted by a prominent Krukenberg spindle, other members of the diagnostic quintet are usually sought out but, when the Krukenberg spindle is atypical, routine observation of pigmentation upon structures seen during microzonuloscopy should stimulate one to look more carefully elsewhere for this pigmentation.
It thus would seem to follow that mild and seemingly insignificant pigmentation, insidiously deposited upon transparent structures within this perilenticular area, may become the first signs in this syndrome. It is possible that a few clusters of pigment when properly evaluated as to distribution, may predict a syndrome which could eventually result in pigmentary glaucoma. Since a significant number of patients who demonstrate various portions of the pigmentary syndrome develop glaucoma, it would appear to be an advantage to observe the syndrome in its incipiency.
While preliminary investigations have not revealed irrefutable prognostic information relevant to the end-stages of this syndrome, it appears that the microzonuloscopy technique offers not only a method of discovering the earliest possible manifestations of the syndrome but also a yardstick by which its progression may be measured.
In order to explain the method of microzonuloscopy, two well-advanced cases will be reported, as well as some examples of very early and mild involvement.
CASE REPORTS CASE 1
A 50-year-old moderately myopic school teacher presented the typical Krukenberg spindle syndrome bilaterally, characterized by corneal pigment spindles, moderate iris atrophy with transilluminable areas in the peripheral iris stroma and increased pigment deposit in the angle of the anterior chamber. The intraocular pressure has been watched carefully and has never gone above IS mm. Hg (Schätz) in either eye.
Under moderate dilatation, the patient was carefully studied by microzonuloscopy, the co-operation being excellent. Wieger's ligament was visualized at its point of attachment to the posterior

MICROZONULOSCOPY 847
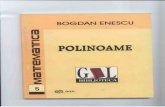
Fig. 2 (Rosen). Findings in Case 1.
capsule as is normally seen in this microsection of the lens but, interestingly, the ligament could also be readily visualized by retro-illumination in this same view (fig. 1-PWL). This was apparently due to the fact that the orange-brown pigment present in this syndrome silhouetted the normally transparent Wieger's ligament (fig. 1-WL). The edge of the lens and the free portion of the anterior hyaloid could be readily observed (fig. 1-LE, AH). Diagonal irregular clumps of pigment were present anterior to the anterior hyaloid, being deposited haphazardly (fig. 1-PZF) so that the un-pigmented portion of the posterior zonular fibers was rendered invisible. The edge of the lens was unusually transparent and, as a result, both the anterior zonular fibers and the posterior zonular fibers with their encrusting pigment could be readily seen. The inferior plica hugged the lens quite closely and then shot out obliquely (fig. 2-a). The depths of the small bays extending from the "hook" (H) showed deposits of pigment in each little valley (p).
The most interesting feature of this examination was the character and the activity of the anterior hyaloid (fig. 2-a, b, c). This structure was seen to be very loose, flopping about like a "guy-wire."
When the patient fixated at near (about six inches away), the anterior hyaloid resembled a double-curved bow, while the inferior plica seemed to run obliquely upward (fig. 2-a). The accordion-pleated folds of the inferior plica seemed to be stippled with clumps of pigment granules and the area of the lens which normally contains the white light reflex from the posterior capsule in the zone of specular reflection showed a brownish pig-mented highlight (Z.S.R., Fig. 2-a, c). When the patient was asked to look up the inferior plica moved up just a bit and the anterior hyaloid began to vibrate, a small hook maintaining fixation to the lens and the vibration occurring beyond this hook-let (fig. 2-a [h]).
When the patient was asked to direct his gaze toward the floor, the anterior hyaloid continued its vibration but finally took a bowing as seen in (fig. 2-c) with a strong anterior convexity. The pigment deposit along the inferior plica seemed to be retained on the external aspect of the membrane so that none of the pigment was on the side of the canal of Cloquet. This vibration of the anterior hyaloid, which is not uncommon in myopic individuals and which may be readily seen if the patient is well dilated and is made to look suddenly from near to far, was extremely well demonstrated in this patient.
CASE 2
This 56-year-old woman was examined on April 29, 1961. She had been operated upon in 1954 for a retinal detachment involving the left eye. The procedure was a classical retinopexy with walling off of the retinal tears. Visual acuity eventually was 20/25.
In October, 1957, she appeared at the office with symptoms of visual loss, R.E., of two weeks' duration. When examined upon this occasion there was present a detachment with three tears in the temporal periphery. Scierai resection and polyethylene tube implantation was followed by eventual visual improvement to 20/30.
The patient was re-examined at regular intervals during the next several years with no significant observations other than that Krukenberg spindles were present (right eye more advanced than left). The tension was 16.5 mm. Hg (Schijftz) in each eye. Gonioscopy showed no excessive pigmentation of the trabeculae. The iris was slightly atrophie on the right side only. Bilateral vitreous detachments were present.
When examined on April 30, 1961, tension was found to be 16.5 mm. Hg (Schätz) in each eye. The pupils were then widely dilated. Only the right eye showed a portion of a pigmented circle upon

848 EMANUEL ROSEN
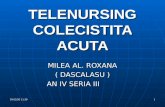
Fig. 3-a (Rosen). Findings in Case 2.
the retrolenticular structures. This was rather incomplete as shown (fig. 3-a). Studied by micro-zonuloscopy, it became evident, with the light section through the lens, that these fragments of rustlike rings were not located in the same anatomic region. When examined looking down at an angle of 70 degrees, the pigmented mass (which was orange-brown in color) was seen actually clinging to the under surface of the anterior hyaloid (fig. 3-b).
The pigment seemed to hug the anterior hyaloid and wobbled slightly with that structure when the patient was asked to change her direction of gaze from near to far (six inches to six feet). This pigment mass was much more extensive temporally than nasally (fig. 3-b, c). The pigment structure below did not extend as far as Wieger's ligament and could not be seen through the lens cut (fig. 3). This pigment was completely within the retro-zonular canal (RZC) and not within the infra-zonular canal.
This location is in marked contrast with the
Fig. 3-b and c (Rosen). Findings in Case 2.
Fig. 3-d and e (Rosen). Findings in Case 2.
anatomic location observed in the upper portion of the retrolenticular area (fig. 3-e). In this view the patient's head has been thrown well back about 45 degrees and the light section through the lens clearly depicts the superior perilenticular area. In this section of the lens, using the narrow beam of light, it becomes evident that pigment is present only at the very point of attachment of the anterior hyaloid to the lens or the very point of contact of Wieger's ligament. There is no space between pigment and lens in this upper section as there is in the lower section and a portion of the upper pigment ring can be visualized through the cut of the lens, as is not true of the same region of the lens in the microzonuloscopy position 70-degrees down (fig. 3-d, e).
CASE 3 This 52-year-old man complained primarily of
increased presbyopic symptoms of six months' duration. Intraocular pressure was 14.2 mm. Hg (Schätz) in each eye. There was no evidence of pigment upon the cornea, no atrophie areas upon the iris and no indication of depigmentation anywhere.
Fig. 4 (Rosen). Findings in Case 3.

MICROZONULOSCOPY 849
When the pupils were widely dilated and when the eye was studied by microzonuloscopy, the anterior hyaloid and Wieger's ligament were readily observed. A large fusiform brick-red deposit of pigment was seen in each hyaloideo-capsular sinus (fig. 4-p). In no other area was any pigment deposit detected. No pigment granules were seen upon the posterior zonular fibers when examined with this technique.
CASE 4 The patient, 53-year-old woman, complained only
of an increasing presbyopic symptomatology. The routine examination was normal in all respects. Intraocular pressure was measured at 16 mm. Hg (Schi^tz) each eye. The pupils were widely dilated and the eyes were then examined in the microzonuloscopy position.
On looking down at a 70-degree angulation, the edge of the lens and the zonular fibers, both anterior and posterior, could be readily visualized. The anterior hyaloid showed just a mild posterior convexity. Several small clumps of brownish pigment could be visualized upon Wieger's ligament in the 5- to 7-o'clock positions (fig. S). Viewed with a narrow optical section through the perilen-ticular area, this pigment was seen in the angle made at the point of union of the anterior hyaloid with the lens (hyaloideo-capsular sinus).
DISCUSSION
The Krukenberg spindle, an endothelial pigment deposit, was first described in 1899, but it was not until 35 years later that an accurate biomicroscopic study and report were given of the frequently associated retrolen-ticular pigment ring.1 This report included the first description of this ring, at least biomicroscopically for, according to Koby, Mauksch was the first to describe this pigment ring upon the posterior capsule in any detail. Mauksch had observed this ring in two young myopic brothers who also had Krukenberg spindles. He assumed that the pigment was lodged in the space between the anterior hyaloid and the lens (HCS) with the deposition upon the posterior zonular fibers accounting for the frayed and irregular appearance of the pigmented ring.
In 1927, Koby, at that time unaware of Mauksch's observations, published two cases of Krukenberg spindles and annular rings of the lens occurring in mother and daughter both of whom were highly myopic. These
Fig. 5 (Rosen). Findings in Case 4.
patients presented Krukenberg spindles along with deposits of pigment upon the posterior capsule of the lens especially prominent in the neighborhood of the arcif orm line of Vogt.
A pigmented circle concentric with the pupillary border was observed and described as an annular pigmented line upon the posterior surface of the lens a slight distance from the lens equator and made up of small brown brilliant granules. Koby stated, "Toward the periphery of the lens these granules appear to depart from the lens surface, for in this area they seem to reside in the vitreous upon a transparent substratum."
A few years later, Koby, in his treatise upon the "Biomicroscopy of the vitreous body,"3 expressed the opinion that pigmented deposits may form upon the posterior peripheral lens surface, frequently gathering as an incomplete circle of yellowish or brownish color. He concluded that this condition occurred primarily in high myopes. Koby believed this was the same pigment dispersion and deposit first described by Mauksch, although he emphasized the fact that Mauksch did not report the pigment around the arci-form line of Vogt.
Koby suggested that this annular pigmented epicapsular line might be present in a certain percentage of cases of Krukenberg spindle and it therefore should be anticipated in certain patients, notwithstanding the fact that a span of more than 35 years occurred

850 EMANUEL ROSEN
between the first reported case of Krukenberg spindle and the initial report of this annular pigmented ring.
In his summary, Koby stressed the acquired nature of this pigmented ring, primarily because the pigment deposition and accumulation were so much greater in the mother than in the daughter, not only as regards the annular ring but also upon the cornea and in die anterior chamber. Furthermore, Koby believed that Wieger's ligament was more melanotropic than were the posterior zonular fibers because of the distribution and deposition of the pigment granules.
My own feeling concerning Koby's report is that we have evidence here of the pigment deposit upon the posterior lens capsule at the site of Wieger's ligament and that the pigment has foilowed and been deposited upon the anterior hyaloid.
In 1929, Cavara4 reported upon the Krukenberg spindle and the annular postlenticu-lar deposit in a highly myopic 54-year-old woman, recognizing this combination as the syndrome previously described by Koby. His description of the annular pigment ring was characteristically accurate. He made no comments concerning the appearance of the vitreous in his patient.
Mann,5 about this time, described a pigmented change under the caption of "Ring-shaped markings near the periphery of the lens," indicating that this was an extremely rare postlenticular change, usually of incomplete nature, running concentric with the edge of the lens. It was her opinion that this line resulted from contact between the tips of the ciliary processes and the lens for too long a period during embryologie development. However, Busacca6 has recently pointed out that this relationship is a very common biomicroscopic observation, whereas the annular pigment line is a rarity.
Mann also referred to the fact that in many animals this relationship is normal and, moreover, in birds the lens is actually indented by these processes so that there is lit-
Fig. 6 (Rosen). Showing defects in annular band of pigment. (After Zentmayer.)
tie evidence to suspect this abnormal embryologie propinquity in the etiology of the pigmented ring. Mann has stated that "the ciliary ring increases in diameter more rapidly than the lens, with the result that the ciliary processes withdraw from the lens leaving a space between these two structures." Busacca6 denied this spatial separation, although gonioscopic studies and microzonuloscopic findings seem to support it.
In 1938, Zentmayer7 reported upon the "Association of an annular band of pigment on the posterior capsule of the lens with a Krukenberg spindle." Zentmayer's patient was a 16-year-old boy with moderate myopic astigmatism. The Krukenberg spindle was quite typical. The posterior capsule of each lens showed a characteristic annular band of brown pigment. The band was situated two mm. in front of the equator of the lens. In the right eye the circular band was broken at the 8- and 4-o'clock positions (fig. 6) . At these defects, short tags of pigment were seen running toward the tips of the ciliary processes. A similar situation was present in the left eye.
Zentmayer's descriptions (using the +20D. lens of the ophthalmoscope) seem to accentuate the value of microzonuloscopy. From his published sketches, I would assume that the typical pigment rings upon the posterior capsule actually outline Wieger's ligament. The tags at the 4- and 8-o'clock positions must represent pigment upon the anterior hyaloid membrane as that structure runs toward the ciliary processes. This is probably how the pigment on the anterior

MICROZONULOSCOPY 851
hyaloid looks when seen "head on" with the +20D. lens of the ophthalmoscope.
If a "phantom" of the lens were cut through the lens at the level of one of these pigmented tags, the picture shown in Case 2 (fig. 3-b) would be seen, in which the "cut" shows the anterior hyaloid membrane running from Wieger's ligament to the ciliary processes, with brown pigment clumps adhering to the anterior hyaloid. It is interesting to note that, in this same view, pigment is somewhat absent where the anterior hyaloid reaches Wieger's ligament and this observation would correspond to the region in Zentmayer's case where the annular pigment ring was described as being broken (or actually where no pigment was present).
Although the exact location of this pigment may seem to be of no significance at the moment, it is of interest to note the many years from the time when the ring was first observed and reported until the simple technique of microzonuloscopy suggests its anatomic position.
Cameron,8 in reporting upon a pigment ring of the posterior lens associated with the Krukenberg spindle, assumed that, because no pigment was present in the retrolental space, the pigment must be derived from the iris only. But inadequate biomicroscopic knowledge of this so-called retrolental space, which is only a potential space, illustrates how conclusions may be erroneously drawn. There is no pigment in the retrolental space because there is no retrolental space. However, pigment does occur upon the zonular fibers and outside of the plicas.
This in no way criticizes Cameron's statements but it is mentioned to show the importance and the value of the microzonuloscopy technique. In reviewing a case of megalocornea9 in which Krukenberg spindles were described, I, too, did not understand this retrolental area which only recently has been clarified by the studies of Busacca.8 The following quotation, taken from the case which I reported in 1945, demonstrates my
inability to localize the position of the pigment present in this vital area:
Lens. Both lenses were dislocated posteriorly in symmetrical fashion, exposing the zonule for a distance of one to two mm. all around. The lens measures 11 mm. in its greatest diameter. The zonular fibers appeared to be intact all around except in the lens of the left eye at the 8- and 11-o'clock positions, where corresponding notching occurred. An occasional brown pigment granule was deposited upon the zonular fibers. The anterior shagreen of the lens of the right eye was unusually prominent. This lens showed no other abnormality. The lens sutures were not remarkable. In the lower portion of the lens of the left eye, in the oldest portion of the posterior cortex, was a crescentic area of grayish-white clouding resembling congenital lenticular detritus. Just behind these lens opacities in the anterior vitreous were several orange-red opacities fused together in a thin matting and strongly resembling "brick-dust."
Vitreous. The vitreous framework showed definite degenerative features. The usual silky character of the vitreous "curtain" had been replaced by a thin fibrillar substance with many small brown granular particles enmeshed in its framework. There was no gross vitreous disturbance.
Although Bellows10 reported upon pigment on both the anterior and posterior lens capsules, I would assume that these deposits were neither similar in appearance nor in size. After dilatation in his reported case, it was stated that a dense brown pigmented ring was visible around the entire circumference of the lens, almost coinciding with the margin of the completely dilated pupil. This "peripheral" lenticular pigmentation was assumed to be the probable source of the pigment seen on the cornea, the surface of the lens, the retrolental space and the aqueous humor.
A most interesting and complete study entitled "The syndrome of idiopathic atrophy of the epithelial layers of the iris and ciliary body" was reported in 1958 by Scheie and Fleischauer.11 The syndrome included: (1) Krukenberg spindle, (2) speckling of the anterior surface of the iris with pigment, (3) pigmentation of the trabeculae, (4) annular pigment ring upon the posterior lens capsule, (5) atrophy of the epithelial layers of the iris and (6) frequent glaucomatous complication.

852 EMANUEL ROSEN
It was stated by these authors that the pigment arose from the epithelium of iris and ciliary body as an idiopathic atrophy. Pigment released from these structures was shown to be deposited throughout the anterior segment of the eye. These authors emphasized the gonioscopic findings and the iris atrophy as determined by transillumina-tion. They felt that the pigmentary glaucoma was probably only a complication of an extensive pigment disturbance within the eye.
Discussing the phenomenon of pigmentation upon the posterior aspect of the lens and zonular fibers, Scheie and Fleischauer described their gonioscopic technique along with the results they obtained. It was evident that there was some limitation in the method of examination, for they stated that under wide dilatation, the visualization of the equatorial area of the lens was possible in all cases, the zonular fibers in most and the ciliary processes in many cases.
It is interesting to note that in the micro-zonuloscopy procedure, if pupils are widely dilated, these areas may be seen in all cases without discomfort to the patient and with much better visibility. Furthermore, the "phantom" cut through the lens gives a much clearer orientation for pigment (fig. 1).
Scheie and Fleischauer also state that the deposition of pigment upon these perilenticu-lar structures offered excellent opportunity for studying this area. In the ordinary micro-zonuloscopy technique, these areas can easily be seen without the need of pigmentary delineation in so-called normal eyes. Apparently the authors used the Koeppe lens and Barkan light for this procedure, which certainly does not permit orientation nor facilitate layer-by-layer observation, as may be attained with a slitbeam of light and high powers of magnification in the microzonulo-scopic procedure. As mentioned by Scheie, the presence of pigment upon the structures of the perilenticular zone renders these transparent membranes and fibers more readily visible; however, it is the use of the thin beam in a thin section which establishes the
accurate location of the pigment. Considering that Scheie and Fleischauer did not have a slitbeam and lens section at their disposal, their observations could not be accurate as to the location of this pigment. Obviously, in my report on megalocornea and Krukenberg spindle already mentioned, I failed to observe the location of this pigment gonioscopically.
Scheie and Fleischauer interestingly described the occurrence of the pigment at two different levels upon the posterior lens: (a) at the hyaloideocapsular ligament and (b) halfway from the ligament to the equator. This is the exact position of the pigment deposition which I observed (figs. 3-b and 3-d).
The simplicity of microzonuloscopy makes it possible to examine the zonular fibers and the ciliary processes with greater ease, clarity and deliberation. It is much easier and more certain than gonioscopy and is preferred by the patient.
If pigment is within the anterior hyaloid (intravitreal) and if it is definitely uveal, derived from the ciliary processes and not hemorrhagic, there must be a break in the continuity of the anterior hyaloid, most probably at its point of attachment beyond the ciliary structures. Pigment which is deposited within the anterior hyaloid but outside the plicas must come from the ciliary processes by way of passage around the peripheral attachment of the anterior hyaloid.
From my limited observations I would think that the pigment cannot go through the anterior hyaloid—nor does the anterior hyaloid show any defect in its structure when it detaches at Wieger's ligament. Therefore, the pigment derived from the ciliary processes and present within the anterior hyaloid must come around the peripheral umbrellalike bow of the anterior hyaloid.
This pigment is more likely to be seen in myopic patients, in some of whom the elongated and arched anterior hyaloid gives the impression that it may be free at its peripheral end. In fact, in many instances the peripheral end of the anterior hyaloid may

MICROZONULOSCOPY 853
be seen to vibrate so that the "wiggle of the anterior hyaloid" has come to mean a specific biomicroscopic phenomenon.
SUMMARY
The new technique of microzonuloscopy has been applied to the syndrome of Kruken-
In reviewing the literature one can find no general agreement as to the best surgical treatment of congenital cataracts. There are several different methods available, each having its own enthusiastic advocate, which would only seem to indicate that ophthalmic surgeons are still looking for the ideal procedure. For more information on this subject, a study was made of 133 patients operated on at the Memphis Eye, Ear, Nose and Throat Hospital between 1944 and 1960. This group includes private cases as well as patients on the charity service. The follow-up period ranged from no return visits to a maximum of 15 years. There were 226 eyes operated on and the visual acuity was known in 152 of the cases. Several patients were too young to check the vision but the results were perfect from a surgical standpoint.
It is well known that surgery of con-
* From the Department of Ophthalmology, University of Tennessee School of Medicine and the Memphis Eye, Ear, Nose and Throat Hospital.
berg spindle associated with lenticular pig-mented rings. The pigment may be localized biomicroscopically by using a narrow beam of light with high magnification. Pigment deposits in the hyaloideo-capsular sinus may be the earliest sign of this syndrome.
692 High Street (2).
genital cataracts does not offer as good a prognosis as surgery of cataracts in adults. Falls,1 in reporting 233 eyes operated on for congenital cataracts, noted that only 53 percent obtained a vision of 20/100 or better, while 25.6 percent had a vision of 20/200 or less and at least 6.4 percent of these eyes were blind. Owens and Hughes,2
as well as Bagley,3 have reported similar results. In this survey of 152 eyes with known visual acuity, only 36 percent had better than 20/70 vision while 31 percent had a vision of less than 20/200 and 11 percent of these eyes were blind. This percentage of blindness is somewhat higher than that reported by Falls.1
ASSOCIATED OCULAR DEFECTS.
The first and most important factor in determining the final visual acuity was the presence or absence of associated ocular defects (table 1). In this series 42 percent of the cases had associated ocular defects. This is somewhat less than the 55.8 percent
REFERENCES
1. Mauksch, H.: Ztschr. f. Augenh. 57:262, 1925. 2. Rosen, E.: Microzonuloscopy. Am. J. Ophth., 53:345-351 (Feb.) 1962. 3. Koby, F.: Biomicroscopy of the Vitreous. Paris, Masson, 1932, p. 63. 4. Cavara, V.: Boll, ocul., 1929, p. 1161. 5. Mann, I.: Developmental Anomalies of the Eye. London, Cambridge, 1937, pp. 360-362. 6. Busacca, A.: Bull. Soc. Franc, d'ophtal., 68:295-305, 1955. 7. Zentmayer, W.: Arch. Ophth., 20:52-57,1938. 8. Cameron, W.: Am. J. Ophth., 25:687-689, 1941. 9. Rosen, E.: Megalocornea. Am. J. Ophth., 28:1352-1359, 1945. 10. Bellows, J.: Arch. Ophth., 32:480482, 1944. 11. Scheie, H., and Fleischauer: Arch. Ophth., 59:216-228, 1958.
A SURVEY OF T H E SURGICAL T R E A T M E N T OF CONGENITAL CATARACTS*
MELVIN W. DEWEESE, M.D. Memphis, Tennessee