articol factori psihocognitivi

of 4
-
Upload
ana-maria-predoi -
Category
Documents
-
view
214 -
download
0
Transcript of articol factori psihocognitivi
-
7/25/2019 articol factori psihocognitivi
1/4
Highlights of The Society of American Gastrointestinal and
Endoscopic Surgeons 2005 Annual MeetingApril 13-16, 2005; Ft. Lauderdale, Florida
Timothy Kuwada, MD
Authors and Disclosures
Posted: 07/05/2005
Forum on Biliary Injuries
The introduction of laaroscoic cholecystectomy !"#$ in the late %&'0s ushered in the era of minimally in(asi(e )eneral
sur)ery* +ince then, it has ecome the referred aroach for cholecystectomy* Durin) the initial years of "#, when sur)eonswere in the -learnin) cur(e- of the rocedure, there was a si)nificant increase in ile duct in.uries !Ds$ comared with oen
cholecystectomy* 1owe(er, most sur)eons are now ast their learnin) cur(e, and many consider "# to e a -asic- laaroscoic
rocedure* e(ertheless, with the current incidence of Ds as hi)h as %*34,%,26these in.uries continue to e (ery moridcomlications that ha(e si)nificant le)al and financial imlications*
This year, The +ociety of American astrointestinal and 8ndoscoic +ur)eons !+A8+$ in con.unction with the American
1eato9Pancreato9iliary Association !A1PA$ and the +ociety for +ur)ery of the Alimentary Tract !++AT$ resented a -orumon iliary n.uries*- A anel of international e;erts re(iewed the a(oidance, reco)nition, and mana)ement of "#9associated
Ds* The session was moderated y athaniel +oer, MD, Professor of +ur)ery, einer) +chool of Medicine orthwesternenly
elie(e that he or she has correctly identified the cystic duct* This leads to an -acti(e mista>e,- with the sur)eon intentionallydi(idin) a duct rather than accidentally cuttin) or cauteri@in) it* Proer li)htin) and laaroscoic euiment, includin) the use of
an)led laaroscoes and minimi@in) lood in the field, hel to reduce the ris> of (isual miscues*
There is a otential for sur)eons to tal> themsel(es out of the resence of ductal in.ury, desite anormal findin)s durin) "#*
Accordin) to Dr* +tewart, less than 254 of Ds are reco)ni@ed durin) laaroscoy, and e(en after con(ersion to an oen
rocedure, 204 of in.uries are missed* urthermore, Dr* +tewart reorted that studies ha(e demonstrated that it ta>es at least 3anormal cues efore the intraoerati(e reco)nition of Ds aroaches %004* +he also discussed the concet of
-conformational ias,- wherey once a sur)eon has made a decision !correct or incorrect$, he or she tends to fa(or any
information that suorts this initial decision and discounts findin)s !anormal anatomy or an intraoerati(e cholan)io)ramB#6$ that may indicate a D*?6+ur)eons must e aware of these sycholo)ical issues and e esecially (i)ilant durin) the >ey
stes of "#* Any anormal findin)s or anatomy must e clarified rior to di(idin) any ductal structure durin) "#*
$%e 'ole o( %olan!io!rams in 'edu#in! B&Is
=illiam Tra(erso, MD, Professor of +ur)ery, Cir)inia Mason Medical #enter, +eattle, =ashin)ton, discussed the role of an B#
in re(entin) Ds, and he re(iewed the critical stes of intreretin) an B#* Bn an AP (iew, the ductal structures found on an
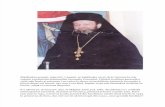
B# form a -si)moid cur(e*- The uer ortion of the cur(e is the left heatic duct the midortion is the common heatic duct!#1D$ and the ottom or distal art of the cur(e is the common ile duct !#D$* These structures are hi)hly constant and should
e identified on all B#s !see i)ure %$*
(Enlarge Image)
Figure 1.
Intraoperative cholangiogram showing the "sigmoid curve."
1owe(er, the insertion and osition of the cystic duct and ri)ht heatic duct!s$ are (ariale, with a %24 incidence of anomalies*This may e;lain why a disroortionate numer of ma.or in.uries occur on the ri)ht (s the left ductal system* Bn a standard AP
(iew, the cystic duct usually enters the ri)ht side of the distal #1D !left side of monitor$ at an an)le of aro;imately 35E*
-
7/25/2019 articol factori psihocognitivi
2/4
1owe(er, the cystic duct may enter the anterior or left side !ri)ht side of monitor$ of the e;traheatic ducts* The cystic duct mayalso arallel the e;traheatic ducts rior to insertion* This laces the mid9 and ro;imal re)ions of the cystic duct closer to the
e;traheatic ducts, increasin) the ris> of D durin) dissection of the cystic duct* n aro;imately 24 of atients, the cystic
duct .oins an aerrant ri)ht heatic duct, which may aear to e a continuation of the distal cystic duct, thus lacin) it at ris> ofin.ury* This aerrant ri)ht duct may e a se)mental ranch or the main ri)ht duct* f a se)mental ranch is di(ided and clied
!+traser) tye in.ury$, it will atrohy and the atient may remain asymtomatic* Bn the other hand, if the main ri)ht duct isdi(ided and clied !+traser) tye 8 in.ury$, the draina)e from the ri)ht loe is ostructed and .aundice, cholan)itis, or oth is
more li>ely to occur*
#omlete e(aluation of the ductal anatomy with B# reuires (isuali@ation of the entire e;traheatic ductal system andifurcation of the ri)ht and left intraheatic ducts* f the #1D and ifurcation are not (isuali@ed, the ti of the cholan)iocatheter
may e ositioned in the #D* Pullin) the catheter ac> should remedy this rolem* f this maneu(er fails to identify the #1Dand ifurcation, the sur)eon should con(ert to an oen aroach*
The contro(ersial issue of routine (s selecti(e B# was also raised* Dr* Tra(erso noted that the aility of B# to re(ent and
identify Ds is deendent on the sur)eonFs caacity to correctly interret the B#* 1e re(iewed se(eral studies that concludedthat routine B# reduces oth the incidence of Ds and time to dia)nosis* 3,56t was ar)ued that routine B# may imro(e
interreti(e s>ills and increase the sensiti(ity of detectin) sutle ductal anomalies*
)perati"e $e#%ni*ues to 'edu#e t%e 'is+ o( B&Is
Mar> #allery, MD, Associate Professor of +ur)ery, factors for Ds, and oerati(e techniues for reducin) Ds*G6
1e echoed Dr* +tewartFs oint that most ma.or Ds are a result of misidentification of ductal structures* Technicalcomlications, such as thermal in.ury, tentin) of the ducts, and dissectin) too deely, are less freuent causes of Ds* +ur)eon
ine;erience, acute inflammation, cystic duct imaction, e;cessi(e leedin), and aerrant anatomy are all ris> factors for Ds*
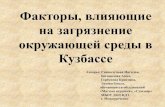
(Enlarge Image)
Figure 2.
Strasberg classification of laparoscopic injuries to the biliary tract. Type injuries originate fromsmall bile ducts that are entered in the liver bed or from the cystic duct. Type ! and Type injuries are fre#uently involved in the aberrant right hepatic duct. Type $ $ %$ and some E
injuries may cause bilomas or fistulas. Type ! and other Type E injuries occlude the biliary treeand bilomas do not occur.
Dr* #allery stressed the imortance of se(eral oerati(e techniues to reduce the ris> of Ds* Proer )allladder retraction
durin) "# is critical in achie(in) e;osure to the cystic duct* This retraction consists of cehalad and sli)ht lateral retraction of
the )allladder fundus and lateral retraction of the )allladder infundiulum* This maneu(er laces the cystic duct in a more
erendicular osition relati(e to the #1D/#D and mo(es the ro;imal and mid9cystic duct farther from these criticalstructures, therey reducin) the chance of misidentification and accidental in.ury* #on(ersely, cehalad retraction of theinfundiulum laces the cystic duct and )allladder arallel, and closer, to the main e;traheatic ducts, which increases the ris>
of in.ury*
The concet of the critical (iew of safety was also emhasi@ed* =ith the )allladder retracted !as descried ao(e$, the -critical(iew- is achie(ed y dissectin) alon) the inferior and medial asect of the )allladder etween the li(er ed and
)allladder/cystic duct .unction* Dissectin) alon) the )allladder ed)e of #alotFs trian)le reduces the ris> of driftin) mediallytoward the main ducts*
-
7/25/2019 articol factori psihocognitivi
3/4
f an in.ury is reco)ni@ed intraoerati(ely, it is (ital to stay calm and see> aroriate hel* A comlete transaction of a ma.orduct should e reaired with a Hou;9en9I heatico.e.unostomy* A rimary duct9to9duct anastomosis in this settin) has an
unaccetaly hi)h lea> and stricture rate* 1owe(er, a small lateral ductal laceration can sometimes e closed rimarily o(er a T9
tue* f a sur)eon is not comfortale with iliary reconstruction, he or she should minimi@e the dissection, lace drains, andtransfer the atient to an aroriate center*
Mi)uel An)el Mercado, MD, ational nstitute of Medical +ciences and utrition, Me;ico #ity, Me;ico, re(iewed the otimaltimin) and techniue of ile duct reair* The ad(anta)es of delayin) !J ? months$ the reair of a D include the followin):
Hesolution of inflammation
Demarcation of ductal ischemia
A otentially lar)er duct to sew to and
The aility to reoerati(ely define ductal anatomy with a (ariety of ima)in) techniues*
#on(ersely, early reair ! ? months$ of a ductal in.ury offers the followin) ad(anta)es:
Potentially uic>er reco(ery
"ower o(erall costs and
"ess moridity from lon)9term drains and catheters*
He)ardless of the timin) of reair, redictors of a -)ood- outcome include a tension9free anastomosis to a healthy duct and
reser(ation of the ifurcation* Dr* Mercado re(iewed data from his series of D reairs and made se(eral conclusions* irst,
enteric anastomosis to hi)her, more ro;imal re)ions of the e;traheatic duct ha(e a lower stricture rate* +econd, when -allthin)s are eual,- Ds should e reaired early* inally, success rates for reair of Ds can e;ceed &04*
The forum concluded with 8duardo de +antianes, MD, PhD, of uenos Aires, Ar)entina* Dr* de +antianes discussed themana)ement of iliary9enteric stenosis followin) ile duct reair* Anastomotic stenosis leadin) to loar atrohy can e
asymtomatic* 1owe(er, it can yield ma.or moridity in the form of .aundice, cholan)itis, ortal hyertension, secondary iliary
cirrhosis, and end9sta)e li(er failure* The first line of theray for anastomotic stenosis is ercutaneous iliary dilatation* n a lar)eseries reorted from The Lohns 1o>ins
-
7/25/2019 articol factori psihocognitivi
4/4
?* =ay "=, +tewart ", antert =, et al* #auses and re(ention of laaroscoic ile duct in.uries: analysis of 252 casesfrom a human factors and co)niti(e sycholo)y ersecti(e* Ann +ur)* 200?2?7:3G093G&*Astract
3* letcher DH, 1os M+, Tan P, et al* #omlications of cholecystectomy: ris>s of the laaroscoic aroach androtecti(e effects of oerati(e cholan)io)rahy: a oulation9ased study* Ann +ur)* %&&&:22&:33&9357*Astract
5* lum DH, Koesell T, 1ea)erty P, +inanan M, Dellin)er 8P* #ommon ile duct in.ury durin) laaroscoic
cholecystectomy and the use of intraoerati(e cholan)io)rahy* Arch +ur)* 200%%?G:%2'79%2&2* Astract
G* +traser) +M, 1ertl M, +oer L* An analysis of the rolem of iliary in.ury durin) laaroscoic cholecystectomy* LAm #oll +ur)* %&&5%'0:%0%9%25* Astract
7* Misra +, Melton , eschwind L, Cenru; A#, #ameron L", "illemoe KD* Percutaneous mana)ement of ile ductstrictures and in.uries associated with laaroscoic cholecystectomy: a decade of e;erience* L Am #oll +ur)*
2003%&':2%'922G*Astract
http://intapp.medscape.com/px/medlineapp/getdoc?pmi=12677139&cid=medhttp://intapp.medscape.com/px/medlineapp/getdoc?pmi=12677139&cid=medhttp://intapp.medscape.com/px/medlineapp/getdoc?pmi=10203075&cid=medhttp://intapp.medscape.com/px/medlineapp/getdoc?pmi=10203075&cid=medhttp://intapp.medscape.com/px/medlineapp/getdoc?pmi=11695975&cid=medhttp://intapp.medscape.com/px/medlineapp/getdoc?pmi=11695975&cid=medhttp://intapp.medscape.com/px/medlineapp/getdoc?pmi=8000648&cid=medhttp://intapp.medscape.com/px/medlineapp/getdoc?pmi=8000648&cid=medhttp://intapp.medscape.com/px/medlineapp/getdoc?pmi=14759778&cid=medhttp://intapp.medscape.com/px/medlineapp/getdoc?pmi=14759778&cid=medhttp://intapp.medscape.com/px/medlineapp/getdoc?pmi=12677139&cid=medhttp://intapp.medscape.com/px/medlineapp/getdoc?pmi=10203075&cid=medhttp://intapp.medscape.com/px/medlineapp/getdoc?pmi=11695975&cid=medhttp://intapp.medscape.com/px/medlineapp/getdoc?pmi=8000648&cid=medhttp://intapp.medscape.com/px/medlineapp/getdoc?pmi=14759778&cid=med