BULETINUL ASOCIAŢIEI BALINT DIN ROMÂNIA file1 BULETINUL ASOCIAŢIEI BALINT, VOL. 11., NR. 42,...
28
1 BULETINUL ASOCIAŢIEI BALINT, VOL. 11., NR. 42, IUNIE 2009 Iunie, 2009, Volumul 11, Nr. 42 Periodic trimestrial, apare în ultima decadă a lunii a treia din trimestru. Fondat - 1999 Redactor şef - Albert VERESS M.D. Sc.D. Lector - Almoş Bela TRIF M.D., Sc.D., J.D., M.A. Tehnoredactor - István PARA Coperta - Botond Miklós FORRÓ Adresa redacţiei: 530.111 – MIERCUREA CIUC, Str. Gábor Áron 10. tel./fax 0266-371.136 0744-812.900, (Dr. Veress) E-mail: [email protected], [email protected], www.balint.xhost.ro Adresa lectorului: E-mail: [email protected] Comitetul de redacţie: Tünde BAKA, Doina COZMAN, Dan Lucian DUMITRAŞCU, Evelyn FARKAS, Liana FODORANU, Ioan-Bradu IAMANDESCU, Cristian KERNETZKY (D), Mircea LĂZĂRESCU Holger Ortwin LUX, Dragoş MARINESCU Ioana MICLUŢIA, Csilla MOLDOVAN, Aurel NIREŞTEAN, Iuliu OLTEAN Gheorghe PAINA, Ovidiu POPA-VELEA, Almos Bela TRIF (USA) Ionel ŢUBUCANU, Éva RERESS, Nicolae VLAD. Editat de Asociaţia Balint din România Tipărit la Tipografia Alutus, Miercurea-Ciuc Manuscrisele sunt lecturate de un comitet de referenţi, care primeşte manuscrisele cu parolă, fără să cunoască numele autorilor şi propune eventualele modificări care sunt apoi transmise autorului prin intermediul redacţiei. Decizia lor este necontestabilă. Toate drepturile de multiplicare sau reeditare, chiar şi numai a unor păr ţi din materiale apar ţin Asociaţiei Balint. Plata abonamentului şi a cotizaţiei se face în cont CEC Miercurea Ciuc, nr. RO26CECEHR0143RON0029733, titular Asociaţia Balint, cod fiscal: 5023579 (virament) sau 25.11.01.03.19.19 (depunere în numerar). Preţ ul unui număr la vânzare liberă este de 2 EURO/număr la cursul BNR din ziua respectivă. Abonamentele pentru ţările occidentale costă 50 EURO/an, incluzând taxele poştale şi comisionul de ridicare a sumei din bancă. INDEX: ISSN – 1454-6051 BULETINUL ASOCIAŢIEI BALINT DIN ROMÂNIA CUPRINS RELAŢIA TERAPEUTICĂ ÎN REACTIA DE DOLIU INDUSĂ DE PIERDERILE MULTIPLE ........................................ 3 Oana Cornelia Dobrescu, Voichiţa Dumitru, Dana Cristina Herţa A SPECIAL FIELD FOR THE BALINTIAN GROUP - HELPLINE SERVICE ........ 7 Istvan Varadi RELAŢIA MEDIC-PACIENT ÎN CADRUL UNEI COMUNITĂŢI TERAPEUTICE ............................. 10 Lux Holger Ortwin THE IMPORTANCE OF STRONG WORKING ALLIANCES IN BALINT GROUP DEVELOPMENT ....................................... 13 Richard B. Addison, U.S.A PIERDEREA ŞI DOLIUL LA PACIENŢII ONCOLOGICI ŞI FAMILIILE ACESTORA .......... 17 Ioana OMER, Onica Ilisei RECLAIMING THE UNCONSCIOUS IN BALINT GROUP WORK .................................... 21 Alan H Johnson, USA ŞTIRI DIN VIAŢA ASOCIAŢIEI ............................ 28
Transcript of BULETINUL ASOCIAŢIEI BALINT DIN ROMÂNIA file1 BULETINUL ASOCIAŢIEI BALINT, VOL. 11., NR. 42,...
1
BULETINUL ASOCIAŢIEI BALINT, VOL. 11., NR. 42, IUNIE 2009
Iunie, 2009, Volumul 11, Nr. 42
Periodic trimestrial, apare în ultima decadă a lunii a treia din trimestru.
Fondat - 1999
Redactor şef - Albert VERESS M.D. Sc.D.
Lector - Almoş Bela TRIF M.D., Sc.D., J.D., M.A.
Tehnoredactor - István PARA
Coperta - Botond Miklós FORRÓ
Adresa redacţiei:
530.111 – MIERCUREA CIUC, Str. Gábor Áron 10.tel./fax 0266-371.1360744-812.900, (Dr. Veress)E-mail: [email protected], [email protected], www.balint.xhost.ro
Adresa lectorului:E-mail: [email protected]
Comitetul de redacţie:
Tünde BAKA, Doina COZMAN, Dan Lucian DUMITRAŞCU, Evelyn FARKAS, Liana FODORANU,
Ioan-Bradu IAMANDESCU, Cristian KERNETZKY (D), Mircea LĂZĂRESCU
Holger Ortwin LUX, Dragoş MARINESCUIoana MICLUŢIA, Csilla MOLDOVAN,
Aurel NIREŞTEAN, Iuliu OLTEANGheorghe PAINA, Ovidiu POPA-VELEA,
Almos Bela TRIF (USA)Ionel ŢUBUCANU, Éva RERESS, Nicolae VLAD.
Editat de Asociaţia Balint din RomâniaTipărit la Tipografia Alutus, Miercurea-Ciuc
Manuscrisele sunt lecturate de un comitet de referenţi, care primeşte manuscrisele cu parolă, fără să cunoască numele autorilor şi propune eventualele modificări care
sunt apoi transmise autorului prin intermediul redacţiei. Decizia lor este necontestabilă.
Toate drepturile de multiplicare sau reeditare, chiar şi numai a unor părţi din materiale aparţin Asociaţiei Balint.
Plata abonamentului şi a cotizaţiei se face în cont CEC Miercurea Ciuc, nr. RO26CECEHR0143RON0029733,
titular Asociaţia Balint, cod fiscal: 5023579 (virament) sau 25.11.01.03.19.19 (depunere în numerar). Preţul unui număr la
vânzare liberă este de 2 EURO/număr la cursul BNRdin ziua respectivă.
Abonamentele pentru ţările occidentale costă 50 EURO/an, incluzând taxele poştale şi comisionul de ridicare a sumei din
bancă.
INDEX: ISSN – 1454-6051
BULETINUL ASOCIAŢIEI BALINT DIN ROMÂNIA
CUPRINS
RELAŢIA TERAPEUTICĂ ÎN REACTIADE DOLIU INDUSĂ DEPIERDERILE MULTIPLE ........................................ 3Oana Cornelia Dobrescu, Voichiţa Dumitru,Dana Cristina Herţa
A SPECIAL FIELD FOR THEBALINTIAN GROUP - HELPLINE SERVICE ........ 7Istvan Varadi
RELAŢIA MEDIC-PACIENT ÎN CADRUL UNEICOMUNITĂŢI TERAPEUTICE ............................. 10Lux Holger Ortwin
THE IMPORTANCE OF STRONG WORKING ALLIANCES IN BALINTGROUP DEVELOPMENT ....................................... 13Richard B. Addison, U.S.A
PIERDEREA ŞI DOLIUL LA PACIENŢIIONCOLOGICI ŞI FAMILIILE ACESTORA .......... 17Ioana OMER, Onica Ilisei
RECLAIMING THE UNCONSCIOUSIN BALINT GROUP WORK .................................... 21Alan H Johnson, USA
ŞTIRI DIN VIAŢA ASOCIAŢIEI ............................ 28
2
BULETINUL ASOCIAŢIEI BALINT, VOL. 11., NR. 42, IUNIE 2009
Prezentarea ASOCIAŢIEI BALINT DIN ROMÂNIA
Data înfiinţării: 25 iulie 1993
Michael BALINT: Psihanalist englez de origine maghiară
Grupul BALINT: Grup specific alcătuit din cei care se ocupă de bolnavi şi care se reunesc sub conducerea a unui sau a doi lideri, având ca obiect de studiu relaţia medic-bolnav prin analiza transferului şi contra-transferului între subiecţi.
Activitatea Asociaţiei:grupuri Balint,editarea Buletinului,formarea şi supervizarea liderilor,colaborare la scară internaţională.
Specificul Asociaţiei: apolitică, nereligioasă, inter-universitară, multi-disciplinară, de formaţie polivalentă.
Obiective: Formarea psihologică continuă a partici-panţilor. Încercarea de a îmbunătăţi prin cuvânt calitatea relaţiei terapeutice medic-pacient şi a comunicării dintre membrii diferitelor categorii profesionale. Rol de “punte” între etnii, confesiuni, categorii sociale, regiuni, ţări.
•••••
BIROUL ASOCIAŢIEI:Preşedinte: Tünde BAKA – [email protected]şedinte: István VÁRADI – istvanvaradi1inbox.comSecretar: Csilla HEGYI – [email protected]: Albert VERESS – [email protected]: Rita-Lenke FERENCZ, Holger Ortwin LUX, Attila MUNZLINGER, Ovidiu Popa-Velea, Éva VERESS.
Cotizaţia se achită până la 31 martie a.c. Cvantumul ei se hotărăşte anual de către Biroul Asociaţiei. În cazul când ambii soţi dintr-o familie sunt membrii Asociaţiei, unul din ei poate cere scutirea de la plata abonamentului la Buletinul Asociaţiei, al cărui cost se stabileşte anual.
Cei care nu achită cotizaţia până la data de 31 martie a anului în curs nu vor mai primi Buletinul din luna iunie, iar cei care nu vor plăti cotizaţia nici până la data de 31 martie a anului următor vor fi penalizaţi cu o majorare de 50%!!! Cei cu o restanţă de doi ani vor fi excluşi disciplinar din Asociaţie.
Studenţii şi pensionarii sunt scutiţi de plata cotizaţiei, fiind necesară doar abonarea la Buletinul Asociaţiei.
Cotizaţia pentru anul 2009 este de 20 EURO (la cursul oficial BNR din ziua în care se face plata), în care se include şi abonamentul la Buletin.
Taxa de înscriere în Asociaţie este de 20 EURO (nu se face reducere nici unei categorii socio-profesionale). Abonamentul costă 6 EURO.
Se primesc articole cu tematică legată de activitatea grupurilor Balint din România şi din străinătate, de orice fel de terapie de grup, de psihoterapie, de psihologie aplicată şi de alte abordări de ordin psihologic al relaţiei medic - pacient (medicină socială, responsabilitate medicală, bioetică, psihosomatică, tanatologie).
Materialele scrise la solicitarea redacţiei vor fi remunerate.
Buletinul este creditat de către CMR ca prestator de EMC, deci orice articol publicat se creditează cu 25 de credite EMC. Abonamentul la Buletin se creditează cu 5 credite.
Redactorul şef şi / sau lectorul au dreptul de a face cuvenitele corecturi de formă, iar în cazul neconcordanţelor de fond vor retrimite articolele autorilor cu sugestiile pentru corectare.
Deoarece revista se difuzează şi în alte ţări, articolele care nu se limitează doar la descrierea evenimentelor balintiene, trebuie să aibă un rezumat în limba română şi engleză, de maximum 10 rânduri dactilografiate. Lectorul îşi asumă responsabilitatea de a face corectura rezumatului
Pentru rigoarea ştiinţifică apreciem menţionarea bibliografiei cât mai complet şi mai corect, conform normelor Vancouver, atât pentru articolele din periodice cât şi pentru monografii (citarea în text se notează cu cifre în paranteză, iar în bibliografie se înşiră autorii în ordinea
citării nu cea alfabetică şi doar acei autori care au fost citaţi în lucrare).
Recenziile cărţilor trebuie să cuprindă datele de identificare a cărţii în cauză - autorii, titlul, toate subtitlurile, anul apariţiei, editura, oraşul, numărul de pagini şi ISBN-ul. Se trimite în fişier separat imaginea scanată a copertei.
Se primesc doar materiale trimise pe diskete floppy de 3,5”, CD room, memory-stick sau prin e-mail ca fişier ataşat. Se vor folosi numai caractere româneşti din fontul Times New Roman, culese la mărimea 12, în WORD 6.0 sau 7.0 din WINDOWS.
Imaginile - fotografii, desene, caricaturi, grafice - vor fi trimise ca fişiere separate, cu specificarea locului unde trebuie inserate în text pentru justa lor lectură. Pentru grafice este important să se specifice programul în care au fost realizate.
Articolele trimise vor fi însoţite de numele autorului, cu precizarea gradului ştiinţific, a funcţiei şi a adresei de contact, pentru a li se putea solicita extrase. Autorii vor scana o fotografie tip paşaport sau eseu pe care o vor trimite ca fişier ataşat sau pe o disketă la adresa redacţiei.
CĂTRE AUTORI

3
BULETINUL ASOCIAŢIEI BALINT, VOL. 11., NR. 42, IUNIE 2009
RE
FER
ATE
Asociaţia Balint are un site. Adresa: www.balint.xhost.ro
Autorii sunt rugaţi să se conformeze regulilor de redactare a articolelor.
RELAŢIA TERAPEUTICĂ ÎN REACTIA DE DOLIU INDUSĂDE PIERDERILE MULTIPLE
Dr. Oana Cornelia Dobrescu*, psiholog Voichiţa Dumitru**,Dr. Dana Cristina Herţa*
* UMF Cluj-Napoca, ** Clinica Psihiatrie III Cluj-Napoca
ANUNŢURI IMPORTANTE
Rezumat: Pierderea unei fiinţe dragi, a sănătăţii, a unei slujbe,
a unui vis sau speranţe, sunt evenimente nefericite prin care trecem cu toţii mai devreme sau mai târziu în această viaţă. Reacţia de doliu se referă la acele emoţii negative, stări fizice şi manifestări de ordin social, care însoţesc aceste pierderi. Pierderile suprapuse sau cumulate cresc riscul apariţiei unor reacţii de doliu complicate, sau patologice, care necesită o intervenţie terapeutică susţinută. În literatura de specialitate se vorbeşte despre o stadializare a reacţiei de doliu, considerată însă arbitrară, iar medicalizarea excesivă a unor reacţii normale la pierdere sunt aspru criticate. Pentru a evita apariţia doliului complicat, consilierea facilitează exprimarea emoţiilor, construirea unor noi tipuri de relaţii fără cei pierduţi, deci reconstruirea lumii interioare a fiecărui individ aflat în doliu.
Cuvinte cheie: pierderi, reactie de doliu, stadializare doliu, doliu patologic
Abstract: The loss of a loved one, of health, a job, of a dream or
a hope are unfortunate events we all pass through sooner or later in this life. Grief refers to those negative emotions, physical states and social behaviors that accompany this loss. Cumulative losses increase the risk of complicated, pathological grief reactions, necessitating a sustained therapeutic intervention. In the literature are presented some grief stages, but these are considered arbitrary, and the excessive medicalization of some normal reactions to loss is fiercely criticized. In order to avoid complicated grief, the counseling offered to bereaved persons facilitates the completion of the relationship with the lost person or object, by expressing the emotions connected, the construction of new types of relationships, without the lost ones, by reconstructing so the inner world of every bereaved person.
Key words: loss, grief, grief stages, pathologic grief
Reacţia de doliu reprezintă totalitatea emoţiilor, de obicei negative, dureroase, apărute în urma unei pierderi majore [1, 2]. Deşi în mod curent, reacţia de doliu ne duce cu gândul la suferinţa cauzată de moartea sau dispariţia unei persoane dragi, sau a unui animal de companie,
specialiştii vorbesc de reacţie de doliu ca răspuns specific oricărei pierderi, fie că este vorba de pierderea unei fiinţe dragi, sau de pierderea unei relaţii, cum este cazul divorţului, a stării de sănătate, a unui membru sau organ, sau a unei funcţii, pierderea controlului, cum se întâmplă în cazul dezastrelor naturale sau produse de oameni, a accidentelor, pierderi sociale, pierderea slujbei, a casei, etc [3]. Autori precum Kissane (2000) [4], definesc pierderea ca fiind deprivarea de ceva investit cu semnificaţie emoţională de către individ. În limba română termenul de doliu include atât pierderea prin moarte a unei persoane iubite, având ca echivalent în limba engleză termenul de bereavement, cât şi procesul de adaptare la o astfel de pierdere, incluzând ritualurile sociale şi culturale ce acompaniază decesul unei persoane, şi care în limba engleză sunt circumscrise termenului de mourning [4]. Reacţia de doliu s-ar suprapune peste termenul englez grief, care include sentimentele şi emoţiile care însoţesc procesul de adaptare la o pierdere, deci acel mourning. Reacţia de doliu include pe lângă reacţiile emoţionale tip tristeţe, disperare, anxietate, mânie, vinovăţie, şi reacţii somatice, precum tulburări de somn, de apetit alimentar, hipersensibilitate la zgomote, dificultăţi de concentrare a atenţiei, agitaţie şi nelinişte, precum şi reacţii sociale, dintre care cea mai frecvent întâlnită este izolarea [5].
Pornind de la studiile efectuate de Lindemann cu ocazia catastrofei produse în urma incediului unei discoteci din Boston, Cocoagrovenut, în 1944, soldată cu nenumărate victime, au fost descrise o serie de caracteristici ale supravieţuitorilor. Printre acestea se numără o stare de amorţire emoţională, preocupări cu amintirea celui decedat, stări confuze de mânie, vinovăţie, tulburări ale patternului comportamental obişnuit, chiar identificarea cu simptomatologia persoanei decedate.
Interesul crescând pentru intervenţia în cazul doliului complicat a făcut ca stadializarea reacţiilor emoţionale prin care poate trece o persoană având o boală în stadiul terminal, descrisă de Elisabeth Kubler-Ross în cartea sa On death and dying, să fie transferată şi în cazul reacţiilor de doliu. Acest lucru a stârnit nenumărate confuzii şi controverse. Autori precum Friedman şi James [6] consideră în primul rând că nu putem vorbi de reacţii universale de doliu, că acestea depind de nenumăraţi factori şi că sunt reacţii foarte personale, individuale.

4
BULETINUL ASOCIAŢIEI BALINT, VOL. 11., NR. 42, IUNIE 2009
RE
FER
ATE
Plecând de la analiza aprofundată a cărţii lui Kubler-Ross, dar şi de la experienţa personală şi profesională cu reacţia de doliu, aceşti autori consideră că negarea, primul stadiu propus de autoarea cărţii On death and dying n-ar fi de fapt decât o figură de stil, şi nu o credinţă întemeiată printre persoanele îndoliate,
Totodată, aceeaşi autori atenţionează că mânia nu este neapărat o reacţie universală de doliu, ea putând apare în legătură mai ales cu anumite tipuri de pierderi, că negocierea se întâlneşte mult mai rar în situaţiile de doliu şi mai frecvent printre pacienţii în fazele terminale ale bolilor, şi că ideea de vinovăţie poate fi adesea indusă iatrogenic, cauzând mai mult rău decât ajutând persoana îndoliată.
Mai mult, starea de amorţire emoţională (numbness) ar fi doar o reacţie ce durează de obicei prea puţin pentru a putea fi catalogată ca şi stadiu. De fapt, pentru aceşti autori, noţiunea de stadiu presupune un cadru temporal, care poate induce ideea, falsă şi adeseori periculoasă, că dacă aştepţi suficient timp, acea stare va trece de la sine. Această atenţionare este valabilă în special pentru stadiul depresiei, când reacţiile comune de doliu, de tipul tulburări ale atenţiei, somnului, apetitului alimentar, lipsa energiei şi labilitatea emoţională, se pot confunda cu simptomatologia unei depresii clinice. Aceasta poate conduce fie la o falsă etichetare ca depresivi a unor indivizi aflaţi într-o stare normală de tristeţe, cauzată de o pierdere importantă, fie, poate mai grav chiar, la etichetarea ca stadiu normal al reacţiei de doliu a unei depresii clinice, şi la aşteptarea ca acest stadiu să fie depăşit, pierzându-se astfel un timp preţios pentru persoana în cauză. De altfel, atât Friedman şi James1 [7] cât şi Carol Crandall2 [8] consideră că nu timpul vindecă prin el însuşi, ci ceea ce faci în tot acest timp, sensul pe care îl dai pierderii suferite, şi modul cum această pierdere este integrată vieţii individului.
Dată fiind universalitatea reacţiei de doliu la pierderile importante, dar şi modul individual, personal în care fiecare din noi răspundem la diferite pierderi, cercetătorii în domeniu s-au arătat foarte preocupaţi de diferiţii factori care ar putea explica de ce unele persoane trec mai uşor prin reacţiile de doliu, în timp ce altele vor dezvolta diferite patologii somatice sau psihologice, ţinând de aşa numita reacţie de doliu complicată sau patologică. Deşi însăşi noţiunea de doliu complicat sau patologic este destul de criticată în literatura de specialitate, totuşi au fost descrise încă din 1965 de Parkes [9] diferite forme de doliu patologic: cronic, întârziat şi inhibat care ulterior au fost reformulate de Volkan, 1970, Parkes, Weiss, 1983 şi Stroebe and Stroebe, 1987 [9], ca şi sindrom de doliu neaşteptat, ambivalent şi cronic. Aceste tipuri de reacţii patologice, asociate mai frecvent cu tulburări de anxietate, depresie, suicid, reacţii psiho somatice sau sindromul de stress posttraumatic [4] au fost asociate unor factori de risc dintre care amintim: relaţiile pre existente cu persoana decedată,
în care ambivalenţa şi relaţiile nerezolvate joacă un rol esenţial, tipul morţii, răspunsul familiei şi reţelei de suport social, alte situaţii de criză sau stress concurente, vârsta la care apare pierderea, sexul, clasa socio-economică, gradul de religiozitate, personalitatea individului [9, 10], şi nu în ultimul existenţa unei patologii anterioare pierderii, a unei depresii [6].
Şi dacă pentru situaţiile de doliu patologic specialiştii sunt unanim de acord cu necesitatea unei intervenţii terapeutice ferme, atât farmacologice cât şi psihoterapeutice, în ceea ce priveşte oportunitatea şi beneficiul unei consilieri în situaţiile de doliu necomplicat, părerile sunt net împărţite, unii considerând chiar că astfel de intervenţii, departe de a aduce un beneficiu clientului, mai rău îl împing în braţele unei iatrogenii, prin medicalizarea forţată a unor stări normale de doliu. Pentru a preveni apariţia unui blocaj în derularea normală a unei reacţii de doliu, şi apariţia unor complicaţii patologice, Friedman şi James, membri fondatori ai The Grief Recovery Institute consideră ca esenţială terminarea, completarea relaţiei cu persoana dispărută sau cu partenerul divorţat, prin comunicarea prin diferite tehnici, a tuturor emoţiilor, gândurilor legate de acea relaţie, chiar şi atunci când celălalt nu mai poate răspunde sau nu se poate schimba [11]. Aceasta în ideea în care o astfel de relaţie neterminată poate conduce la credinţa nefondată a necesităţii unei suferinţe perpetue şi a imposibilităţii schimbării şi a regăsirii fericirii pierdute [12]. O altă metodă predicată de cei doi autori este împărtăşirea amintirilor, a sentimentelor legate de persoana şi de relaţia pierdută [13], precum şi admiterea, recunoaşterea suferinţei, a emoţiilor negative de mânie, teamă, durere, tristeţe legate de aceste pierderi, şi nu negarea şi represia lor, ceea ce s-ar solda cu efecte negative pe termen lung [14].
Vom prezenta în continuare cazul doamnei V. internată în Clinica de Psihiatrie III cu o complicaţie de tip depresiv a unor reacţii de doliu suprapuse, rezultate în urma unui avort indus şi a pierderii unui organ, respectiv în urma unei histerectomii cauzată de infecţia produsă de un sterilet introdus post abortum. Doamna V., în vârstă de 43 ani, mama unui băiat de 21 ani, recăsătorită de 19 ani, în urma decesului primului soţ, se prezintă la internare cu o simptomatologie polimorfă, de tip depresiv, cu idei de incurabilitate, de inutilitate, ideaţie suicidară pasageră fără plan organizat, tristeţe, anhedonie, apatie, scăderea randamentului activităţilor cotidiene, izolare socială şi în cadrul familiei, însoţită de numeroase simptome somatice tip cefalee, senzaţii de arsuri în corp şi mai ales abdominale, transpiraţii atât diurne cât şi nocturne, valuri de căldură, tulburări de somn şi inapetenţă. Simptomatologia actuală a debutat insidios de cca. 2 ani, în urma unei histerectomii totale cauzate de complicaţiile induse de un sterilet. Pacienta a primit după operaţie tratament substitutiv hormonal,
1 ‘Time does not heal. Time goes by. It is the actions that you take within time that can help you grieve and complete relationships that have ended or changed’. Timpul nu vindecă. Timpul doar trece. Acţiunile pe care le faci în acel timp te pot ajuta să te desparţi şi să termini relaţiile care s-au încheiat sau care s-au schimbat (nt.)2 ‘You don’t heal from the loss of a loved one because time pases; you heal because of what you do with the time’. Nu te vindeci de pierderea unei persoane iubite pentru că timpul trece; te vindeci datorită a ceea ce faci cu acel timp.(nt.)

5
BULETINUL ASOCIAŢIEI BALINT, VOL. 11., NR. 42, IUNIE 2009
RE
FER
ATE
pe care însă nu l-a urmat decât câteva luni, precum şi tratament antidepresiv, la care însă s-a dovedit total non compliantă, fiindu-i teamă să nu devină dependentă de această medicaţie. Aceste idei au fost introduse şi menţinute de anturajul apropiat al pacientei, în special de mama sa, foarte intrusivă, critică la adresa pacientei şi autoritară. Din antecedentele pacientei reţinem o serie de evenimente traumatice: moartea timpurie a primului soţ, foarte iubit, după care a rămas cu un copil mic de crescut; acesta este momentul când doamna V. se apropie foarte mult de părinţii săi care o ajută din punct de vedere profesional, deschizând împreună cu mama o afacere comercială a cărei şef este mama pacientei. Urmează apoi o căsătorie cu un bărbat obişnuit să comande şi să hotărască totul în casă, ceea ce face din doamna V. o persoană obedientă, care din când în când îşi permite să mai hotărască şi singură, însă numai în ceea ce o priveşte pe ea personal, şi niciodată în ceea ce priveşte relaţia lor sau în problemele legate de gospodărie. În urmă cu cca. 3 ani pacienta rămâne însărcinată cu cel de al doilea soţ, însă hotărăşte, de una singură, că soţul nu este pregătit să accepte rolul de părinte, fiind centrat prea mult pe reuşita în afaceri, şi face o întrerupere voluntară de sarcină despre care nu vorbeşte nimănui. Ulterior, decide să utilizeze ca şi metodă contraceptivă un sterilet, care însă va fi cauza unei infecţii uterine, care va conduce, după multe peregrinări pe la diferiţi medici ginecologi din diferite oraşe, la o histerectomie totală. În timpul internării pacienta se plânge la început zilnic de cefalee, senzaţii neplăcute de arsuri corporale, valuri de căldură şi transpiraţii, precum şi de o senzaţie de gol abdominal, acolo unde îşi imagina ea ca a fost uterul ce i-a fost scos. Gândurile sale erau centrate în totalitate pe pierderea uterului şi odată cu el a feminităţii sale, pe pierderea sănătăţii şi a volumului său anterior de muncă, în momentul internării pacienta nemairecunoscându-se în ceea ce a fost odată. Impresia pe
care doamna V. o dădea personalului medical era a unei femei ce se “agăţa” cu disperare de durerea şi nefericirea sa, care parcă îi procurau singura plăcere posibilă încă pentru ea. Complianţa la tratamentul antidepresiv a fost marcată de o evoluţie ondulantă, în sensul în care atunci când se simţea foarte demoralizată şi neputincioasă îl accepta, pentru ca în momentul în care se simţea ceva mai bine, să renunţe la el, de teama unei dependenţe. Astfel, în momentul internării sale, pacienta încercase deja mai multe tipuri de antidepresive de care se plângea că nu au avut nici un efect benefic. În timpul spitalizării, pacienta primeşte un nou tratament antidepresiv, Coaxil, la care s-au adaugat o serie de şedinţe de narcoanaliză, ce au permis accesarea unui nucleu de nemulţumiri şi frustrări personale, atât pe plan sexual, marital, cât şi pe planul relaţiilor interpersonale dominate de mama şi de soţul său, emoţii care au constituit ulterior baza discuţiilor terapeutice. De asemenea, a fost abordată tema avortului şi a trăirilor generate de acesta, precum şi de pierderea uterului, legată în reprezentările pacientei de pierderea feminităţii sale şi a interesului soţului pentru ea, dar şi de pierderea interesului său pentru actul sexual, ca şi pentru apariţia sa fizică. Totodată, s-au folosit câteva şedinţe de expresie grafică, tip artterapie, care a facilitat mobilizarea, conştientizarea şi numirea diferitelor emoţii negative. Expresia grafică urmăreşte să dea posibilitatea pacientului să se exprime şi să se reprezinte prin intermediul formelor, simbolurilor şi culorilor, să utilizeze suporturile de exprimare non verbală şi verbală, cu o puternică notă de personalizare.
La acestea, s-a adăugat o şedinţă de consiliere de cuplu, în care celor doi soţi li s-a facilitat deschiderea către comunicarea referitor la dificultăţile din cuplu, la aşteptările fiecăruia de la partenerul de cuplu, precum şi despre pierderea funcţiei reproductive. Prin toate aceste tehnici psihoterapeutice au fost vizate schematele cognitive fixate,
„Cerc magic”

6
BULETINUL ASOCIAŢIEI BALINT, VOL. 11., NR. 42, IUNIE 2009
RE
FER
ATE
precum faptul că “pierderea uterului înseamnă că nu mai sunt femeie”, “am un gol în abdomen”, etc, ajungându-se în final la atenuarea acestor gânduri şi modificarea imaginii de sine. Evoluţia cazului a fost lentă dar favorabilă, în sensul în care simptomatologia fizică şi psihologică cu care s-a internat a diminuat în mod semnificativ, iar pacienta a reuşit să depăşească blocajul centrat pe pierderi şi să-şi privească viitorul ca pe ceva plăcut şi realizabil.
Ceea ce s-a întâmplat cu doamna V. în timpul spitalizării poartă în literatura de specialitate numele de grief work şi presupune reorientarea gândirii către pierderea suferită şi către emoţiile dureroase implicate de această pierdere, exprimarea acestor emoţii în cuvinte, ceea ce permite în timp reorganizarea lumii interne a individului, adaptarea la o nouă etapă de dezvoltare în absenţa fiinţei, situaţiei sau organului pierdut [10]. În cazul doamnei V. putem vorbi de o serie de pierderi semnificative de-a lungul vieţii sale, urmate de reacţii de doliu mai mult sau mai puţin rezolvate, dar care s-au acumulat în timp, conducând la credinţa falsă că ea nu va mai fi niciodată ceea ce a fost cândva, că nu se va mai face bine niciodată şi că nu va mai fi niciodată fericită, de unde contemplarea destul de frecventă a morţii.
Histerectomia, ca şi procedură chirurgicală invalidantă, se însoţeşte adesea de o serie de reacţii emoţionale negative de tipul anxietăţii şi depresiei, de reacţia de doliu secundară pierderii funcţiei reproductive, precum şi de teama de raporturi sexuale nesatisfăcătoare, legate uneori de modificările fiziologice induse de extirparea ovarelor [15]. Mai mult decât atât, o întrerupere voluntară de sarcină se însoţeşte adesea de o reacţie de doliu mai profundă şi mai întârziată decât în cazul unei pierderi perinatale, întrucât această pierdere este cel mai adesea nemărturisită, ascunsă şi încărcată de un sentiment de ruşine şi vinovăţie real şi obiectiv [16]. Emoţiile negative pot să se perpetueze şi să se complice, ca şi în cazul doamnei V., iar cererea de ajutor pentru o depresie sau o altă complicaţie a unui doliu nerezolvat poate apare după ani de zile, când legătura cu evenimentul traumatizant cauzal este mult mai greu de stabilit.
În astfel de cazuri, chiar dacă farmacoterapia induce o anumită ameliorare a stării psihice a subiectului, psihoterapia este cea care va permite accesul la aceste evenimente traumatice profund reprimate, parcurgerea paşilor dureroşi ai panicii, repulsiei şi urii pentru a ajunge la acceptarea realităţii şi a responsabilităţii pentru cele întâmplate [16]. Din nefericire, atât societatea, în general, cât şi secţiile de ginecologie, în particular, sunt prea puţin, sau deloc pregătite pentru a facilita exprimarea tuturor emoţiilor negative asociate diferitelor pierderi (de organe înalt investite emoţional, precum uterul şi ovarele, dar şi a embrionilor, fetuşilor, sau nou-născuţilor morţi la naştere).
Sensibilizarea echipei terapeutice la astfel de subiecte, şi apoi a pacientelor, prin educaţie sanitară, ar putea constitui nu doar un deziderat medical ci şi o metodă de prevenţie a diferitelor complicaţii induse de pierderile nerezolvate.
Bibliografie:
1. Gale Encyclopedia Of Psychology 2Nd Ed, pp. 397-399, 2001 2. Stedman’s Medical Dictionary, 28th Edition. 2006. Lippincott
Williams & Wilkins 3. http://www.helpguide.org/mental/grief_loss.htm4. D. Kissane. Loss, Grief and Bereavement. http://www.ipos-
society.org/professionals/meetings-ed/core-curriculum/bereavement/en/player.html
5. http://en.wikipedia.org/wiki/Grief 6. Russell Friedman & John W. James. The myth of the stages
of dying, death and grief. http://www.grief.net/Articles/Myth%20of%20Stages.pdf
7. Russell Friedman & John W. James, Right or Happy...Pick One http://www.grief.net/Articles/Right_or_Happy_Pick_One.htm
8. Grief Counseling And Therapy http://www.deathreference.com/Gi-Ho/Grief-Counseling-and-Therapy.html
9. M. Bradbury. Representations of death. A social psychological perspective, Routledge, London, 1999
10. M. Allen, S. Marks. Understanding grief. ht tp://www.obgyn.net/pregnacy-bir th/pregnacy-bir th/
articles/grief_allen_1115 11. Russell Friedman & John W. James Less Than Loved Ones-
Hopes and Dreams, http://www.grief.net/Articles/Less_Than_Loved_Ones.htm
12. Russell Friedman & John W. James. Am I Equipped for Happiness? http://www.grief.net/Articles/Am_I_Equipped_for_Happiness.htm
13. Russell Friedman & John W. James. Am I Paranoid, or are People Avoiding Me ?, http://www.grief.net/Articles/Am_I_Paranoid.htm
14. Russell Friedman & John W. James. I’m Fine... and Other Lies!!! http://www.grief.net/Articles/I’m_Fine_and_Other_Lies.htm
15. Emotional reactions to hysterectomy. http://www.svcmc.org/18680.cfm
16. E. J. Angelo. Psychiatric sequelae of abortion: The many faces of Post-Abortion grief. Linacre Quaterly, vol 59, no2, 1992. http://www.hopeafterabortion.com/aftermath/index.cfm?page=angelo
„Vârste”

7
BULETINUL ASOCIAŢIEI BALINT, VOL. 11., NR. 42, IUNIE 2009
RE
FER
ATE
Abstract:In our-days globalized and postmodern world East-
European human professionals can face newer, unexplored social demands. Balintians can give a great contribution in several ways to those initiatives that reach for answers and solutions for these demands. A special field of balintian work is the Balint group for Helpline Service team. In this paper the Author underlines some of the typical aspects of this work, concerning particularities of the HL service, of this kind of Balint group and the difficulties of the group leader.
Key words: globalization, helpline, concerning parti-cularities
“We must continue to offer the experience to everyone so that is available for those who need it. We must continue our research so that we can demonstrate some of the beneficial effects. We must go on training group leaders. We will never change all the light bulbs but we must keep on enough lights to enable people to know we are still here: enough light for everyone who needs to read our message.”
- John Salinsky -
I. The ChallengeIt sounds like a common place but it’s true: we live
today in a postmodern and globalized world. Without trying to do a deeper analysis of these terms we can state that they have a specific meaning in East-Europe. It is well known and described in meteorology that the natural phenomena are the most unstable, noisy, confusing and dramatic at the frontline of cyclones and anticyclones. We can consider East-Europe as a frontline of globalization and postmodern way of thinking. Examination, description and analysis of social changes are subject of sociology; the matters of politics are to develop appropriate answers, attitudes and strategies. The question is: what the doctor or human professional can – or has – to do at the frontline of changes. The need for crossing over the biomedical paradigm and taking the psychosocial aspects into consideration has never been as emphatic as it is today. In my opinion the doctor has only two options: to ignore the reality if he/she prefers the self-isolation in the professional (in a way, very protective) ivory tower, or he/she to recognize the new challenge and to assume a new, broader social mission.
For balintian doctors it is obvious that discussing exclusively on the doctor-patient relationship we can only touch the top of the iceberg. Without the doctor’s high social sensitivity the whole underwater world can remain mysterious and mostly unexplored, hidden for him/her. That could be the reason why several Romanian Balint
groups instinctively involve non-medical professionals into their work: psychologists, social workers, teachers, family therapists and even lawyers, engineers and economists.
I would like to point out – from the group leader’s point of view – some particular aspects of balintian work in a very special field: the helpline service.
Even if it has a more than fifty years history, the helpline does appear as an essentially globalized and postmodern answer to the globalized and postmodern demands of society.
Our HL service started in 2005 in Harghita County, a quite isolated mountain area with the highest prevalence of suicidal events, depression, alcohol abuse and violence all around Romania.
The team of our Service consists of specially trained helper professionals and volunteers. Primordial goals of the Service are suicide- prevention, crisis intervention, supportive assistance and data base function. Our Statement is based on IFOTES (International Federation of Telephonic Emergency Service) principles and ethic codes regarding the goals, privacy, neutrality, professional standards, and voluntaries and so on.
Below I would like to underline some particular difficulties a group leader might face in a Balint group for HL team.
II. Relationship particularities, the helper’s special problems
1. Problems of controlling, initializing♦ The caller is the one who establishes the theme and the
orientation of the conversation ♦ the caller is the one deciding when to place the call, the
helper cannot interfere♦ the caller decides when the conversation ends♦ the conversation depends on the caller. He is the one
deciding the speed and rhythm of the conversation (there can be more minutes of silence, rhythm changes because of the emotional changes/swing. The helper can only follow this imposed rhythm and speed.
♦ It depends on the caller whether he speaks at all ♦ It depends on the caller whether he introduces him-self
or not♦ The tonality, vocabulary, manner depends on the caller
2. Problems of intimacy and privacy♦ The helper does not know the caller (and probably will
never know)♦ The caller does not know the helper (and he may not!)♦ If the caller recognizes the helper or the other way,
the helper must manage the situation to sustain the anonymous relationship.
A SPECIAL FIELD FOR THEBALINTIAN GROUP- HELPLINE SERVICE
Dr. Istvan Varadi, MD., General practitioner, Romania
8
BULETINUL ASOCIAŢIEI BALINT, VOL. 11., NR. 42, IUNIE 2009
RE
FER
ATE
3. Lack of stable frames ♦ The relationship is occasional; the helper must help only
during this one “meeting”. ♦ It cannot be planed: the helper does not know in advance
what the problem might be, how much the caller tells about that particular problem, how much time do they have to discuss about the problem, when the caller will end the conversation.
♦ There is no contract between them; the caller has no moral responsibility.
♦ Because of the factors discussed, the frame is very loose; the helper must handle the conversation without any stable base, just improvising.
4. Lack of visual/personal contact ♦ the helper cannot evaluate the body language of the
caller ♦ the helper cannot give feedback through body
language♦ there are only vocal meta-communication possibilities,
these being the most important: ○ vocal volume ○ tonality ○ communication manners ○ rhythm, intermission, fastness ○ does the caller speak immediately or keeps
silence for a while ○ how many silent calls were before he spoke ○ background noises, voices
5. Lack of feedback, case follow-up • the helper usually does not know the result of the
conversation (especially in a case of suicidal crisis) • if still there is an appointment for a date-fixed call: ○ What happens if the caller does not call?
○ What happens if the caller calls too many times, becoming an addicted, chronicle caller?
III. The nature of the group (particular problems of the group)♦ the members are not necessarily trained helpers (mostly
without any previous experience in group work or supervision )
♦ there are always more cases than the group could handle at a time
♦ The time limits are flexible: we know when we start, but we don’t know when we are going to close the group
♦ The narrative of the case holder has a great importance – every detail is important because of the minimal information.
♦ the questions point the dynamic of the caller-helper discussion:○ What was the first sentence?○ Why did he call now?○ How did he get there to call?○ What was like the tonality, speaking manner?○ Rhythm? Fastness? Intermissions?○ What was the declared expectance of the caller?○ What was the hidden expectance of the caller?○ What were the expressed emotions?○ What were the expressed emotions towards the helper?○ What were the emotions of the helper?○ The phantom portrait of the caller ■ the fantasy and non proven hypothesis
have a great role in the group discussion ■ great emotional intensity ■ the emotional transfer is fast and very intensive ■ the group members experience a great emotional saturation even after the group work.
„Forţa vitală”
9
BULETINUL ASOCIAŢIEI BALINT, VOL. 11., NR. 42, IUNIE 2009
RE
FER
ATE
IV. The particular problems of the group leader (resulted from the situation described before)
1. In the group structure♦ big group number, usually over 15-16 members♦ Enlarged small group?♦ Fishbowl with external group working as a reflecting team?♦ The diversity of professionals and volunteers from
different working areas, usually without any or little balintian experience.
♦ More helper “generations” in the group, the problem of integration of the new members ( how to motivate new generations or members for an active, participative presence).
2. In the time structure♦ The group always needs more than 60-90 minutes to finish a case.
♦ There can be new members in the group who need to come to know the balintian work procedure. There is no need to present the psychodynamic depths; it is enough to present the group working method. It can be presented by the group leader or by an older member.
♦ The time frame of the different sections (case introduction – questioning – discussion) may be changing, according to the particular situation/case. Every part can be longer than the usual balintian group work. The group leader can interfere but cannot be intrusive!
♦ There is always needed time for reflection, for emotions to settle down not only for the case holder, but for the whole group.3. In the group dynamic structureSelecting the case: usually there are more cases than
the group could handle in one group; In our experience the group can work properly only with one case. It is difficult and delicate job for the group leader to lead the group to choose a case. The decision is made by the group with the constant supervision of the leader.
The narrative of the case holder: little information, many emotions, ♦ it is the most important not to settle time limits, the
presentation will be anyway „self-limited”, ♦ the case holder can be encouraged to talk about his/her
feelings, fantasies and anxieties ♦ The phantom-portrait of the unknown caller and the map
of relationships which develops from this information. Questioning: (as a general rule): no time pressure on
the group! having a great emotional substance, it needs time to ask and answer a question. The silent moments are very important.
Discussions:♦ The leader can help the group not to orientate towards
the solution of the problem, but let the emotions, fantasies, doubts, anxiety to flow.
♦ The group members usually recall their own caller problems, they incline to emphasize with the case holder.
♦ At the end of the discussion it usually helps if the group members can formulate a good-bye sentence in the name of the caller.
Ending the group♦ It is very important to ask the group feedback after the
case holders’ intervention.♦ It is particularly important to ask about the emotions of
those group members who renounced to their own case. They can ask for personal supervision or just wait for the next balintian group to come.4. Regarding personality of the group leader:
♦ an accurate experience as a Balintian group leader♦ good experience in Help Line work♦ to be avoided if possible a permanent Help Line worker,
it is advisable to be an “external” group leader.♦ continuous self- development and supervision
Final conclusionsAbove I summarized our three year experience in Help
Line work. It would be very useful and constructive if these thoughts would be completed, enriched, overdeveloped by the balintians working in similar fields.
Our work confirms the use and efficiency and efficacy of the balintian method not only for medical structured groups, but also for all those individuals, groups, communities who are working – voluntarily or not – in the social care system and who have to deal with the difficult, complex, heavy and twisted present world.
Dare de seamă, septembrie 2008

10
BULETINUL ASOCIAŢIEI BALINT, VOL. 11., NR. 42, IUNIE 2009
RE
FER
ATE
„Trebuie să fim conştienţi că dorinţacea mai mare a fiecărui client,
respectiv pacient, este aceea de a fi înţeles.”Michael Balint (1)
Rezumat:Comunitatea terapeutică, deşi este un model consacrat
pe plan mondial şi chiar veriga principală în cadrul lanţului terapeutic al unor tulburări precum dependenţele de droguri legale şi ilegale, în ţara noastră încă reprezintă un pionierat. În acest câmp terapeutic special şi relaţia medic-pacient este una particulară, procesul terapeutic fiind influenţat mai ales de situaţia şi dinamica grupului. Abordarea este una holistică, incluzând pe lângă medicina clasică psihoterapia de grup şi cea individuală, consilierea familiei, ergoterapia şi dezvoltarea unor aptitudini sociale.
Cuvinte cheie: comunitate terapeutică, adicţie, medi-cină holistică
Abstract:The Therapeutic Community, even if established
from many decades and recognized in many countries as the main link in the therapeutical chain of disorders as the addiction to legal and illegal drugs, is still a pioneer model in Romania. In its special therapeutic field the doctor-patient relationship has certain particularities, the therapeutical process being influenced mainly by the group dynamic. The approach is a holistic one, including beneath the classical medicine the group and individual therapy, family counselling, ergotherapy and the training of social skills.
Key words: therapeutic community, addiction, holistic medicine
Concepţia de comunitate terapeutică a fost dezvoltată de către psihiatrul britanic Wilfred R. Bion, asociat „grupului Tavistock”, care a început să trateze, în aşa numitul experiment Northfield, veterani suferind de nevroze în urma experienţelor din război, în cadrul unor şedinţe de grup în loc de psihanaliză individuală, pentru a putea beneficia de metodele psihanalizei un număr mai mare de pacienţi.
Termenul „comunitate terapeutică“ a fost consacrat în 1946 de către Tom Main, care a aplicat această concepţie la Cassel-Hospital lângă Londra. Este vorba de o restructurare a situaţiei clinice, astfel încât aceasta, sub forma comunităţii terapeutice să poată sprijini procesul terapeutic, spre deosebire de mediul patogen în care persoana respectivă a trăit anterior. În această concepţie toţi oamenii care trăiesc şi muncesc împreună într-un centru psihiatric, respectiv pacienţii, surorile, infirmierii, medicii
şi personalul auxiliar, fiind legaţi de relaţii bazate pe o încredere reciprocă autentică, formează o unitate organică cu ţelul de a crea cele mai bune premize pentru vindecarea şi reintegrarea în viaţa socială.
În acest model pacienţii nu mai au rolul unui membru pasiv, care doar primeşte o asistenţă şi este dependent de instituţie, ci devine un participant activ şi partener în aplicarea planului terapeutic şi chiar un membru deplin şi un colaborator în comunitatea clinicii.
Pacienţii participă la toate activităţile din cadrul centrului, primesc mai multă responsabilitate şi mai multe posibilităţi de a participa la luarea deciziilor, sunt trataţi ca parteneri. Pot primi diferite sarcini în cadrul clinicii. De exemplu, unii se ocupă de flori, alţii de programul pentru timpul liber, alţii primesc sectoare unde răspund de ordine şi curăţenie, sau răspund de respectarea programului de către toţi pacienţii. Pot deveni “naşi” pentru pacienţii noi, îi familarizează cu regulile casei, îi ajută să se integreze. Pot fi aleşi responsabili de casă sau de echipe. Se pot ocupa de distribuirea corespondenţei.
Câteva principii fundamentale ale unei comunităţi terapeutice sunt:
1. Clinica este un câmp terapeuticÎn clinică devine activ un câmp terapeutic iar procesul
terapeutic este influenţat mai ales de situaţia şi dinamica grupului. Relaţia duală medic-pacient, respectiv terapeut-client, trece pe un plan secundar. Psihoterapia nu este limitată la terapia individuală efectuată cu medicul sau psihologul.
2.Terapia este asigurată printr-un grup de persoane active în terapie
Câmpul terapeutic poate fi menţinut doar printr-o colaborare strânsă şi o bună coordonare în cadrul grupului. Asta presupune o comunicare cât mai deschisă între toţi participanţii şi o mare toleranţă faţă de toţi membrii. Este importantă continuitatea echipei de terapeuţi. Este valabil principiul stimulării optimale a funcţiilor şi capacităţilor fiecărui membru pornind de la premiza egalităţii tuturor membrilor.
3. Potenţialul terapeutic al pacienţilor este susţinut în mod optimal
Pacienţii participă în mod activ şi responsabil la procesul terapeutic, pentru a-şi creşte autonomia. Fiecare este încurajat să se prezinte în cadrul comunităţii, pentru a putea profita de feedbackul celorlalţi şi a-şi putea corecta tiparele necorespunzătoare. Sunt încurajate acţiunile concrete, pentru a facilita accesul diagnostic şi terapeutic. Tot ce se întâmplă în cadrul comunităţii terapeutice poate fi inclus în reflectări şi evaluari. Chiar şi realitatea pacientului din afara clinicii (de exemplu profesie, familie) sunt incluse în terapie.
RELAŢIA MEDIC-PACIENT ÎN CADRUL UNEICOMUNITĂŢI TERAPEUTICE
Dr. Lux Holger Ortwin, Sibiu-Şura Mică

11
BULETINUL ASOCIAŢIEI BALINT, VOL. 11., NR. 42, IUNIE 2009
RE
FER
ATE
Trecând acum la experienţa directă dobândită în peste zece ani de activitate în cadrul Comunităţii Terapeutice „Nazaret” din Şura Mică (pentru bărbaţi) şi fiind implicat în unele perioade şi în acordarea asistenţei la Comunitatea Terapeutică „Insula Speranţei” din Vurpăr (pentru femei), ambele patronate de Asociaţia umanitară „Crucea Albastră din România”, doresc să punctez câteva aspecte esenţiale ale procesului terapeutic într-o comunitate terapeutică pentru persoane dependente de alcool sau alte droguri, aflate în recuperare.
Foarte important este momentul stabilirii primului contact, care se poate realiza pe cele mai diverse căi. De multe ori este pe cale telefonică, alteori prin scrisori sau vizite. Uneori suntem solicitaţi direct de către persoana dependentă, dar în cele mai multe cazuri cei care sună sunt membrii de familie, rude, prieteni etc. . Se pune deci problema transmiterii unor informaţii corecte într-o formă succintă şi totuşi amabilă. De multe ori sunt pacienţi care răspund prima dată la telefon şi intermediază legătura cu terapeuţii. Deci şi ei sunt incluşi în acest proces, fiind instruiţi în privinţa informaţiilor pe care le pot transmite. Persoanele care ne caută au informaţii sau reprezentări foarte diferite despre o comunitate terapeutică Uneori au informaţii din mass-media, alteori de la medici, psihologi, asistenţi sociali sau preoţi cu care colaborăm. În ultimii doi ani mulţi au aflat de existenţa noastră prin internet.
Pasul următor este o consiliere cu persoana dependentă sau cu aparţinătorii care doresc să ia legătura cu noi. Ideal este ca această consiliere să se realizeze atât împreună cât şi separat, pentru a permite o evaluare cât mai complexă a situaţiei. Dacă distanţele sunt mari şi persoanele în cauză nu au posibilitatea să se deplaseze, uneori această consiliere se rezumă la o convorbire telefonică. Acolo unde este posibil consilierea familiei va continua şi pe perioada terapiei persoanei dependente şi chiar şi după aceea, pentru a reduce comportamentele co-dependente şi a prelucra greşelile care se fac frecvent din partea familiei: reproşuri inutile, neîncredere exagerată, teama de a-i transfera responsabilitatea, dezinteres faţă de noile preocupări, aşteptarea unei atitudini servile din partea celui dependent etc.
Evaluând datele obţinute, stabilim dacă este vorba şi de o dependenţă fizică, respectiv dacă există riscul de apariţie a sevrajului la întreruperea consumului. Dacă este cazul, recomandăm o internare de 1-2 săptămâni la un spital de psihiatrie pentru dezintoxicare. Dar ne întâlnim şi cu cazuri care refuză internarea la psihiatrie. Atunci eventual îi internăm cu declaraţie pe proprie răspundere vizavi de posibilele complicaţii ale sevrajului. Ştiu însă şi de comunităţi terapeutice în alte ţări unde chiar şi dependenţii de heroină sunt primiţi direct, trecând prin sevraj „pe viu” (cold turkey), fără medicamente. La pacienţii care prezintă doar o dependenţă psihică nu se pune problema internării prealabile la psihiatrie, decât eventual pentru o comorbiditate (depresii severe, tulburări anxioase).
Terapia propriu-zisă începe când persoana este lucidă şi respectă regula abstinenţei, dealtfel condiţia sine qua non a reabilitării psiho-sociale.
Metoda principală este terapia de grup. Ea are multe avantaje în cazul persoanelor dependente. Stimulează
solidaritatea între persoane care au trecut prin experienţa aceleiaşi boli. Grupul reduce din responsabilitatea terapeuţilor pentru schimbările care urmează să aibe loc şi stimulează capacitatea de autovindecare (autoreglare organismică) a membrilor grupului. De asemenea în cadrul terapiei de grup se depăşeşte mai uşor tendinţa de negare sau minimalizare a problemei din partea pacientului, care la început este adesea ruşinat de comportamentul său anterior legat de dependenţă, sau care poate încă speră ca poate redeveni „băutor normal”.
Omul poate afla în grup că nu este singur cu suferinţa sa. Poate câştiga încredere în sine, aflând cum şi-au rezolvat alţii problemele pas cu pas, alţii care poate au avut o situaţie la plecare şi mai grea. Primeşte feedback la modul cum este perceput în cadrul grupului şi poate experimenta, în acest cadru, noi modele de comportament. Adesea este perceput în mod pozitiv sentimentul apartenenţei la un grup, uneori după perioade lungi de (auto)izolare. Şi prin observarea celorlalţi şi rezonanţă cu emoţiile lor poate să înţeleagă mai bine cum funcţionează propriul psihic şi poate învăţa şi din experienţa celorlalţi. Poate să-şi crească încrederea de sine, observând că este important pentru ceilalţi şi că poate să-i ajute. Câteodată se formează în grup relaţii aşa cum existau ele in familia în care a crescut. Atunci acestea pot fi prelucrate în grup. Prin exprimarea şi trăirea sentimentelor în grup poate câştiga mai multă încredere în propriile sentimente. Şi, în sfârşit, poate ajunge la concluzia că el este răspunzător pentru viaţa sa şi pentru sensul pe care i-l dă. Însă toţi aceşti factori de interacţiune din cadrul grupului nu-şi pot exercita efectul pozitiv decât cu condiţia ca persoana respectivă să devină activă. (2)
Desigur că şi în cadrul comunităţii terapeutice terapia individuală îşi păstrează valoarea ei. Mai ales pentru abordarea anumitor probleme pe care pacientul le consideră prea intime pentru a le aduce în faţa grupului. Am remarcat că solicitările de terapie individuală sunt foarte diferite, ceea ce ţine în mare parte de personalitatea fiecărui pacient.
Foarte importantă în cadrul comunităţii terapeutice este şi ergoterapia, sub diversele ei forme, de la muncă comunitară la art-terapie. Reţin o expresie a unor ergoterapeuţi francezi care ne-au vizitat în urmă cu câţiva ani: „În ergoterapie munca este pretext pentru terapie.”
Andre Moreau o formulează în modul următor: „Munca nu este un scop în sine, ci un mijloc de a-şi dezvolta conduita în faţa celorlalţi, de a observa, de a sublinia în ce măsură un participant repetă, aici şi acum, tulburările de comportament pe care le regretă sau la ignoră în exterior. (...) Pentru a creşte eficienţa, caut să găsesc activităţi reale şi nu imitaţii cum ar fi împletitul, macrameul sau pictura decorativă. Dimpotrivă, caut sarcini cât mai obişnuite posibil, simple, puţin primitive ca să le fac accesibile tuturor, fără operaţiuni tehnice complexe, fiind totuşi atent în special la utilitatea lor şi la posibilitatea de a aprecia eficacitatea reală a persoanelor: restaurarea unei case, activităţi de terasare, zidărie, foraj, grădinărit, tăierea lemnelor...” (3)
Şi în comunitatea noastră terapeutică pacienţii sunt implicaţi mai ales în activităţi cu utilitate practică: grădinărit, îngrijirea unor animale, lucrări de întreţinere şi

12
BULETINUL ASOCIAŢIEI BALINT, VOL. 11., NR. 42, IUNIE 2009
RE
FER
ATE
amenajare a clădirilor, repararea de biciclete second-hand, producţia de suc natural de mere, bucătărie etc.
Ţelul terapiei pentru pacienţii aflaţi într-o terapie de reabilitare pentru o adicţie poate fi formulat în cuvintele: O viaţă responsabilă, împlinită, fără drog.
Fritz Perls, părintele Gestalt-terapiei, şi-a formulat ţelul în modul următor: „Omul modern a pierdut atât de mult din potenţialul său, încât capacitatea sa de a face faţă existenţei este mult diminuată. Ţelul meu este următorul: Pacientul să-şi recapete potenţialul pierdut. Să integreze polarităţile aflate în opoziţie, să recunoască diferenţa între jocurile sale – mai ales verbale – şi comportamentul său autentic (...). În criza desfăşurată într-un mediu sigur, al situaţiei terapeutice, pacientul începe să-şi asume riscuri şi să-şi transforme energiile. În loc să-şi manipuleze mediul pentru a obţine sprijin se urmăreşte obţinerea unui autosuport cât mai mare, deci încrederea în propriile resurse. Acest proces este numit maturizare. Când pacientul a învăţat să stea pe propriile picioare din punct de vedere emoţional, intelectual, şi economic, va dispărea nevoia sa de terapie. Se va trezi din coşmarul existenţei sale. Tehnica de bază este nu să explicăm pacientului cum stau lucrurile, ci să-i punem la dispoziţie posibilităţile să se înţeleagă singur şi să se descopere. În acest sens, influenţez şi frustrez pacientul încât se vede pus faţă în faţă cu sine însuşi. În acest proces se identifică cu potenţialul său pierdut, de exemplu asimilându-şi proiecţiile sau eliminând părţile străine.” (4)
Mai ales în ultima parte a terapiei, în comunitatea noastră terapeutică, punem accentul pe însuşirea unor tehnici şi metode pentru prevenirea recidivei (păstrarea distanţei de siguranţă, fixarea de ţeluri pozitive, autoevaluare realistă, trecerea la acţiune, creşterea toleranţei la frustrare, exersarea „pe uscat” a situaţiilor cu risc de recădere), ţinând cont de situaţia specifică a fiecărui client.
Pentru mulţi dintre clienţii noştri primul an de abstinenţă este greu de suportat. Poate că pe plan raţional sunt convinşi de avantajele noului stil de viaţă, bazat pe
abstinenţă. Dar pe plan afectiv încă nu simt un echilibru. Şi poate încă nu au învăţat foarte bine să se bucure de alte plăceri ale vieţii.
Un prieten american, abstinent de alcool de peste 20 de ani, mi-a spus odată: „Nu ştiu dacă am avut cinci zile bune în primul meu an de abstinenţă. Dar în ultimul an nu ştiu dacă am avut cinci zile proaste.”
Doresc să închei cu nişte cuvinte care în opinia mea se potrivesc deopotrivă atât comunităţii terapeutice cât şi grupului Balint:
„Ne aflăm aici pentru că nu putem scăpa de noi înşine. Atât timp cât omul nu se poate privi pe el însuşi în ochii şi inimile semenilor săi, el se află într-o continuă evadare.
Câtă vreme nu acceptă ca cei din jur să fie părtaşi ai interiorului său, el nu are parte de adăpost.
Câtă vreme se teme sa fie înţeles, el nu se poate recunoaşte– va rămâne singur.
Unde putem afla o asemenea oglindă dacă nu în aproapele nostru?
Aici, în comunitate, omul poate să îşi clarifice anumite lucruri despre sine şi nu se va mai vedea uriaşul viselor sale sau piticul temerilor sale, ci omul – parte a unui întreg – care îşi aduce contribuţia la propria prosperitate. Pe un astfel de teren poate prinde rădăcini şi poate creşte, nu singur – ca în moarte, ci viu ca om între oameni.”
Richard Beauvais (1964)
BIBLIOGRAFIE
1. Franz Sedlack, Gisela Gerber: Beziehung als Therapie, Therapie als Beziehung. Michael Balints Beitrag zur heilenden Begegnung, München, 1992
2. Ralf Schneider, Ingrid Lux, Holger Lux – „Alcoolul şi medicamentele – droguri?“ Editura hora, Sibiu, 1999
3. Andre Moreau – “Viaţa mea aici şi acum – Gestalt-terapia, drumul vieţii”Editura Trei, Bucureşti, 2005
4. Stefan Blankertz, Erhard Doubrawa – „Lexikon der Gestalttherapie“, Peter Hammer Verlag, Wuppertal, 2005
Grupul din Şura Mică

13
BULETINUL ASOCIAŢIEI BALINT, VOL. 11., NR. 42, IUNIE 2009
RE
FER
ATE
THE IMPORTANCE OF STRONG WORKING ALLIANCES IN BALINTGROUP DEVELOPMENT*
Richard B. Addison, PhD. U.S.A
Abstract:In order for Balint work to flourish, leaders need to
actively develop new groups and sustain those groups over time. It is not enough to be an accomplished Balint leader. Balint leaders must attend to the development and maintenance of good working alliances. These must include relationships with individuals, groups, and the organizations within which these groups take place. This paper examines the working alliances in three Balint groups: for physicians in training, faculty physicians, and physicians in a large medical practice. The future of Balint work depends on developing and maintaining solid, dynamic and successful multilevel working alliances.
Key words: group leader, relationship, future of Balint work
One of the passions in my professional life since I’ve been at the Santa Rosa Family Medicine Residency over the last 27 years has been leading Balint groups and other reflective group experiences. One of the main reasons we have created the ABS, IBF, and other Balint societies, is the promotion and furtherance of Balint work. This includes both the expansion of Balint work to those not currently participating in groups, as well as the care and maintenance of those already existing groups. Unless we pay attention to how best to maintain the quality of the groups we are currently leading, develop new groups, Balint will not grow and flourish. This is a problem that we’ve been grappling with for a while.
The first part of my argument is that it is not enough to be an accomplished Balint leader; not only do we need to be excellent leaders, we need to actively work to develop new groups, and sustain those groups over time. (I won’t continue on this point, as I’m fairly confident I would only be preaching to the choir.)
And here is the second, and most central part of my argument and the one I’ll be focusing on today – the crucial importance of the working alliance for the future of Balint work.
There is a great deal of very good research coming out of psychotherapy that is quite germane to the purpose of promoting and sustaining productive groups. This body of research looks at the working alliance. A good strong working alliance is defined as “the degree to which the therapy dyad is engaged in collaborative, purposive work.” 1They find that the quality of the working alliance is by far the most predictive of a successful outcome in psychotherapy --more important than patient characteristics, psychotherapist characteristics, psychotherapist technique, attitudes or theoretical orientation. I believe that this is also the case in primary care medicine. And I believe it is also
the case in Balint groups. Therefore, what I’m going to focus on today is an expansion of the definition of the working alliance to include not only physician and patient, not only leader and group, but also, and perhaps most importantly, leader and organization. I am arguing that the development and maintenance of a good working alliance must include relationships with individuals, groups, and the organizations within which these groups take place, in order to optimize the possibilities of successful, long-standing Balint groups.
To this end, I’m briefly going to trace the developmental process and challenges of the three Balint groups I currently lead, highlighting the problems that arose, threats to the formation and continuance of the groups, and how I am addressing those problems, all with an eye to the importance of creating and maintaining good working alliances so that Balint group work can continue to grow.
FIRST I WILL TALK ABOUT RESIDENT BALINT GROUPS.
How did the Santa Rosa Resident Balint group experience come to its current form? We had resident groups about 25 years ago when FD came for an 8-year tenure as our residency director. When he left, the groups disappeared. The subsequent director (whose tenure was about 12 years) couldn’t understand Balint (he stormed out of the room during one demonstration Balint). All this time, we had P&PD groups, which addressed many of the residents’ needs for support and group affiliation and were very popular. However, I kept looking for an opportunity to reinstitute resident Balint. It turned out the director of our outpatient family medicine center had participated in a previous Balint group and was willing to excuse R2s from clinic for one hour twice a month for a Balint experience. I remember attending a harvest party at his home after he told me that almost no faculty member ever attended any of his functions outside the residency. I think this helped our working alliance. He later told me that he had noticed that patient complaints decreased dramatically when residents began doing Balint. I told him how much I appreciated his creative problem solving that freed the R2s to form a Balint group. The group was well-liked and got very positive feedback on the year-end evaluation. This allowed me to think about expanding from a one-year experience for just R2s to a two-year experience that included R2s and R3s; In order to get the support from other faculty members to expand the group, I knew I had to rebuild the entire Balint infrastructure at the residency. By this time, I had the Faculty Balint Group going again. We also had the ABS credentialing initiative going strong. I encouraged a few other faculty members to attend Leadership Training Intensives and to become credentialed leaders. I also had

14
BULETINUL ASOCIAŢIEI BALINT, VOL. 11., NR. 42, IUNIE 2009
RE
FER
ATE
been at the residency for 20 years and had developed good working relationships with most of the faculty. With this support among the faculty, I proposed taking over a precious dedicated conference hour twice a month, where residents got credit for attendance and did not have competing clinic pressures. Even though the residency director couldn’t stand the Balint process and didn’t understand it, we had a good enough relationship that he trusted my judgment that it would be a worthwhile educational experience for the residents. I had a similar relationship with the residency administrator, who, at a critical meeting, in the face of opposition to Balint, came up with the compromise idea of trying the Balint groups for a two-year trial. That was about 4 years ago.
Residents spend two years in Balint now, a year with each of two leader pairs, Two of the non-faculty leaders volunteer their time without pay, and one of whom drives over an hour twice a month to co-lead his group. In terms of maintaining the group, all leaders (including one trainee) meet after the groups for 30-45 minutes where we present our groups, and discuss group development, leadership, and threats to the group, co-leader relationships and other such issues.
The group takes place at the end of the day on Thursday, a time when most residents would rather be going home to their families or going out to exercise. The residents are required to sign in for Balint, just as they are required to sign in for all the other Thursday afternoon conferences.
As a member of the faculty who tries to attend to their well-being and long-term development, I hope the residents know I am there for them, that I try to understand how their lives as residents are not easy. I cut them slack if they are late for the start of group. I try to end on time, believing it is more likely that they will attend if they are confident
that we will be done on time. I try to understand when they use the group to complain about how difficult they have it with patients. I try to make the atmosphere of the group stimulating and energizing, especially since it takes place at the end of the day. I try to come to the group with a generous, optimistic attitude. I honestly look forward to spending time with the residents and their cases. (They love to hear updates on the cases previously presented, since many of them know the patients being presented by other residents.) I try to understand the stress they hold as residents at different developmental levels of their training.
(The beauty of a vertical group that contains residents who have never experienced Balint as well as residents who have a year of experience, is that the experienced residents help train up the inexperienced ones. The inexperienced ones look forward to being with the class ahead of them in the Balint group.) In other contexts, I mention that their difficult cases might be possible Balint presentations. I want them to graduate knowing what the Balint process is and to feel it as familiar, to miss it, and band together with their colleagues to request a Balint group from their employer. (More about this later….)
To summarize, in order to develop and maintain a successful Balint experience during Residency, I had and have to attend to my working alliances with the residency director, the family practice center director, the residency administrator, my co-leaders, the individual residents, and the organizational needs of the residency curriculum.
AND NOW THE FACULTY BALINT GROUP:
This is a group that began over 25 years ago, although only two of us were members back in the day. It had a long hiatus during very dark financial times. I reconstituted
Curs lideri

15
BULETINUL ASOCIAŢIEI BALINT, VOL. 11., NR. 42, IUNIE 2009
RE
FER
ATE
the group about 8 years ago. In its current form, we meet twice a month. It is led by myself and another credentialed physician co-leader. The largest challenge for Faculty Balint is numbers; this group is always on the edge in terms of having enough members to make it feel like it is a solid group. It currently has five or six participant-members, plus the two leaders. Competing demands for faculty time always threaten having enough bodies in group to make for a lively discussion. I send the members reminders about a week in advance of the group, requesting regrets only, assuming they will attend. I also ask them to block their schedule for the second and fourth Thursday of each month from 3-4 PM. I invite them to invite new faculty, as I do; I emphasize the team building and connective benefits of group – that they not only come for themselves, but they come to support each other as well. I try to look forward out loud at being able to spend reflective time with them at the group. We joke and have fun with each other, most of us believing that education, at best, should also be an enjoyable experience.
Cases come from either the members’ (or occasionally the leaders’) patient or teaching population. Most everyone looks forward to presenting cases. The members are very considerate and tend to take turns doing so; it is rare that one person will dominate with frequent presentations. My co-leader and I meet briefly at the end of the day to check in about anything we need to attend to. I write up the case at the end of the day. I occasionally remind them of the patients and residents they have presented over the years.
My role is far less traditional in this group. Again, I struggle against scheduling threats to member attendance, such as faculty presentations at the resident conferences. (I have even asked the conference coordinator to try not to schedule faculty who are Faculty Balint participants to present during the time that Faculty Balint is held. Since he happens to be a member of Faculty Balint, this sometimes works.)
Unfortunately, the group is sometimes quite small: only three or four members plus two leaders on occasion. At these times, when the presenter pushes back, one or both of the leaders will participate more with the group in speculating about the case. Also, on occasion, both of the leaders have presented their own cases.
Most of the participants are my colleagues, some were my residents whom I’ve recruited to be faculty, and recruited to be in the Faculty Balint group. They each take an hour out of their administrative time to attend. One is a former interim residency director who saved my job during dire financial cutbacks. So my relationship to the members of this group is much more complex and multidimensional than in the resident group; instead of being just a leader to the group members, I am also a colleague, former teacher, friend, and consultant to the members at various times.
The most striking difference in my leadership of the Faculty group is my (and my co-leader’s) availability to fluidly participate in a member-like role, while still maintaining ultimate responsibility for the group.
Because of the size, the leaders move back and forth between member-like and leader-like interventions. This is sometime referred to as “leading from within.” 2 To not do so, would not fit with our Faculty Balint group. Over the years, I’ve evolved to this style of leading the group, and it seems to work. Now if we can just secure the funds to hire additional faculty who want to part of the group…
So again to summarize, for the ongoing success of the Faculty Balint group, I again have to attend to my working alliances with the residency director, my volunteer co-leader, the conference coordinator, the faculty members, and other faculty, who might become members at some time in the future.
BALINT FOR PRACTICING PHYSICIANS
I have just begun a group for physicians practicing in a local HMO. I co-lead this group with another credentialed leader, an MD, who also co-leads the other resident Balint group. The HMO group has about 9 possible attendees, five of whom usually can attend at any one group. The participants are primary care physicians, either family physicians or internists, who expressed interest in this group after I was invited to give a talk on burnout, meaning in medicine and sustainability of practice. I was invited by a graduate of the program who missed having a group reflective experience and wanted the HMO to institute one.
Primary care physicians in this organization were under tremendous stress. Some had left, many were depressed. They decided something was needed. The department planned a day off-site, part of which was my talk. At the end of the talk, I suggested possible actions both individuals and organizations might take to address the problem. I recommended Balint and P&PD groups as two important organizational interventions to address burnout and promote sustainability of practice. From that talk and their fear of an impending shortage of primary care physicians and concern for others becoming burned out, the HMO committed to three groups for a year, each meeting twice a month. Some physicians chose to attend the Balint Group, others chose the P&PD group, and a few are choosing both.
The participants include: newly hired physicians having difficulty acclimating to the HMO, since they receive the most difficult patients for the first two years until they have established their own, familiar patient panel; physicians who know me from another context – either they were former residents I taught, or physicians who had been at one of my talks or workshops; physicians who had previous Balint experience; physicians who desperately needed to talk about troubling cases in a non-judgmental format; physicians who were isolated and wanted to connect with their colleagues; or physicians who were on the edge of quitting or falling apart.
I still think it an unbelievably propitious opportunity to run such a group for such a productivity-driven organization. At a time when physicians in such an organization come under scrutiny for ordering more tests and lab work than

16
BULETINUL ASOCIAŢIEI BALINT, VOL. 11., NR. 42, IUNIE 2009
their peers, when physicians are asked to see more and more patients, for physicians who are inundated with charting and other desk medicine requirements, I think it somewhat extraordinary that the organization is willing to pay for two leaders to hold a Balint group for interested physicians, and, that physicians are willing to take an hour out of their busy day (which will likely result in them working an hour later that evening). It seems in this local context a type of “tipping point” was reached allowing everything to come together so that the group could begin and people could experience the benefits.
Because of the relationship many of them have had with me over the years when they were residents, they trust that a confidential group reflective experience might again be helpful to them. One of them missed his group experience so much that he asked me to give the talk, and asked the HMO to institute the groups for the physicians. Without the good working alliance he and I had developed during his residency, I’m not sure either the opportunity to speak to the department or the opportunity to lead groups for the HMO would have occurred.
The largest difference in my leadership of this group is probably my intense efforts at establishing the safety of the group in the face of constant threats to that safety: For example, the group felt threatened that the department chair wanted to participate, since he evaluated them and granted them their end of year bonuses. Also, there is no dedicated room for this group, except for one that contains the refrigerator and microwave that other staff use for their lunches. Even though I place a sign on the door asking them to wait until the group is over (a somewhat unrealistic request on my part), we are often interrupted by someone needing something from the refrigerator. Also the room is separated from the health educator’s office by
an accordion divider, which is unsatisfactory in terms of confidentiality. For the small price of a sandwich and soft drink, the health educator has offered to lunch elsewhere and try to schedule appointments around our group time. I want the members to feel safe presenting cases of great vulnerability in a confidential format. The tremendously painful cases they present (e.g., a frustrated physician presented his relationship with an eating disordered patient refusing all entreaties to eat; a shocked and surprised physician presented one of his patients, who worked at the medical center, who carefully and privately planned her own successful suicide; and others) These are evidence that they can allow themselves to share very vulnerable feelings and situations with each other.
I promised to supply the HMO with a group evaluation by the group members in the late fall. I don’t know if the HMO will be able to afford or choose to continue the group past the end of the year (or even to the end of the year, considering the current economic challenges). So far the participants have been incredibly enthusiastic and appreciative of the opportunity. I hope the organization will find the resources so that the group can continue.
To summarize for the practicing physician group, I had and have to attend to nurturing strong working alliances with former residents, the department chief (and his administrative assistant who arranges the rooms and the lunches), as well as the individual physicians in the group. As the year comes to a close, I imagine my working alliances with others will also become important in regard to the potential continuation of the group.
In conclusion, I am convinced that without the good relationships or working alliances that I developed over the years, with individuals, with the groups, and with organizations, the continued existence and the ongoing viability of all of these groups would not be possible.
I hope that these three tales will stimulate you to go out and examine the nature and quality of the working alliances you have now; I also hope you will look at potential alliances that may either positively affect the longevity of your existing groups or open up the possibilities of new groups. I hope that attention to the quality and strength of working alliances at all levels will only help us to further promote Balint work, work that we all have experienced as invaluable in improving the physician-patient relationship, the health and well-being of patients, and the satisfaction, sustainability and meaning of medical practice.
References:1. Baldwin S, Wampld B, Imel Z. Untangling the Alliance-
Outcome Correlation: Exploring the Relative Importance of Therapist and Patient Variability in the Alliance. Journal of Consulting and Clinical Psychology 2007;75:842-52.
2. Kerfoot K. Leadership: Social Identity and Guiding from Within. Nursing Economic$ 2007;25:296-8.
* This paper was presented on April 18, 2009, International Balint Weekend, Chicago,
RE
FER
ATE
Real Dance

17
BULETINUL ASOCIAŢIEI BALINT, VOL. 11., NR. 42, IUNIE 2009
RE
FER
ATE
PIERDEREA ŞI DOLIUL LA PACIENŢII ONCOLOGICIŞI FAMILIILE ACESTORA
Dr. M Psih. clinician specialist dr. Ioana OMER,Spitalul de bolnavi cronici şi geriatrie «Sf. Luca», Bucureşti
Rezumat:Pierderea şi doliul sunt etape pe care pacienţii
oncologici şi familiile lor le parcurg de la debutul bolii. În cazul pacienţilor adaptarea la pierdere este condiţionată de vârsta pacienţilor, stadiul bolii, structura de personalitate a acestora, copingul la boală. Reacţiile la pierdere ale pacienţilor pot fi de tipul: negare, furie, dezorganizare, acceptare, reorganizare, prelucrarea durerii şi emoţiilor, reorientarea către alte aspecte ale vieţii. În cazul familiilor reacţiile pot fi asemănătoare cu cele ale pacienţilor şi ele sunt influenţate de: natura relaţiei cu persoana dispărută; (persoană apropiată sau nu, relaţii armonioase/conflictuale, etc.), personalitatea supravieţuitorului. Atât în cazul pacienţilor cât şi în cazul familiilor se poate recurge la consiliere, psihoterapie, grupuri de suport, etc.
Cuvinte cheie: modalităţi de ajutor reacţii, psihoterapie.
Abstract:The bereavement and the mourning are two important
stages for the oncological patients and their families since the beginning of the disease. In the case of the patients the adjustment to bereavement it depends from the age, stage of the disease, their personality, coping with the disease. There can be different reactions to loss of the patients: negation, anger, and despair, and disorganization, acceptance, processing of the pain and emotions, reorientation to other life aspects. The reactions can be similar in the case of the
patient’s families and are influenced by different aspects: the nature of the relationship with the patient (good or bad relationships), the personality of the survivor. There can be used different modalities of help like counseling, psychotherapy, support groups, etc.
Key words: Modalities of help, reactions, psycho-terapy:
Pierderea (engleză = loss) defineşte situaţia unei persoane care a suferit o despărţire de o altă persoană de care era ataşată (1). Pierderile pot fi însă în cazul bolnavilor neoplazici de mai multe tipuri după cum vom vedea în continuare.
Dupǎ debutul bolii, pacienţii cu cancer se pot confrunta cu mai multe tipuri de pierderi care pot avea consecinţe negative asupra evoluţiei lor ulterioare cu răsunet în plan psihic sau fizic. Acestea pot fi (2):
1. Pierderea sănătăţii (în sensul de «a fi bine», «a se simţi bine»);
2. Pierderea independenţei: de multe ori pacienţii oncologici devin dependenţi de îngrijirile care li se acordă de către cei din jur, mai ales, în cazurile complicate sau stadiile terminale;
3. Pierderea unor părţi din propriul trup (mastectomii sau extirpări chirurgicale ale anumitor zone afectate de cancer);
4. Pierderea sexualităţii: se leagă de credinţa pacienţilor că nu mai pot funcţiona sexual la fel ca înainte
Primul strigăt
18
BULETINUL ASOCIAŢIEI BALINT, VOL. 11., NR. 42, IUNIE 2009
deşi cercetările au arătat că în multe cazuri extirpările tumorilor din zonele genitale nu afectează dorinţa sexuală şi nici buna desfăşurare a actului sexual;
5. «Pierderea viitorului»: în cazul bolnavilor de cancer o serie de planuri de viitor şi de speranţe sunt distruse. Pacienţii sunt confruntaţi cu conştiinţa faptului că viitorul este anulat.
6. Pierderea speranţei: este cea mai chinuitoare dintre multiplele şi zdrobitoarele pierderi. G.N. Shrader (1992, apud (2)) observǎ sentimentele de disperare, neputinţǎ şi dispariţie la cei atinşi de boli incurabile, iar L. Dean şi colab. (1998, apud (2)) noteazǎ faptul cǎ ei exprimǎ dezamǎgire şi demoralizare. Privind cǎtre viitor rareori pacienţii viseazǎ la remediu şi la vindecare, întrucât îşi pierd motivaţia pentru viaţă şi capacitatea de a face planuri;
7. Pierderea securitǎţii psihosociale: bolnavii de cancer resimt insatisfacţie,
nesiguranţă, insecuritate, dezamăgire şi constrângere în redefinirea valorilor pe care încă le mai au (K.A.Coburn, D.Malena, 1998, apud (2));
8. Pierderea interesului pentru viaţǎ;9. Pierderea statutului social şi a rolurilor sociale:
atât a celor profesionale, cât şi a celor social-cetăţeneşti sau familiale;
10. Pierderi materiale: pierderea locului de muncă şi implicit a venitului rezultat din aceasta pentru unii dintre ei;
11. Pierderea stimei şi a respectului de sine: respectul de sine se leagă de imaginea de sine pe care o are pacientul. În formarea imaginii de sine intervin o serie de factori precum aspectul fizic, inteligenţa, caracterul, capacitatea de a munci, de a fi productiv, capacitatea de a găsi mijloace compensatorii pentru o deficienţă reală etc. şi care, de multe ori, în afecţiunile oncologice sunt alteraţi provocând apariţia unor stări de deprimare şi dezamăgire.
Reacţiile de doliu la pacienţii oncologici consecutiv acestor pierderi sunt descrise de către E. Kubler-Ross (1969) care a identificat 5 etape/stadii pe care le parcurge pacientul din momentul conştientizării bolii:
I. Prima etapǎ este numită de autoare «Şocul şi negarea»: etapa «Nu, nu eu/ Nu e posibil/ Nu mi se poate întâmpla tocmai mie». Negarea este considerată un mecanism psihologic-tampon, un mijloc de a face faţă unor veşti şocante prin amânarea realităţii.
În această etapă, terapeutul trebuie: să nu insiste ca pacientul să accepte realitatea diagnosticului, să evite să-i dea speranţe false, să-i acorde timp şi sprijin emoţional pentru a accepta situaţia şi să facă mici sugestii în direcţia adevărului. Negarea poate fi acceptată însă doar atâta timp cât nu afectează pe de o parte deciziile medicului în diversele etape ale bolii, înţelegerea obiectivelor tratamentului de către pacient şi discernerea între diversele opţiuni terapeutice, iar pe de altă parte, demnitatea şi respectul de sine al pacientului.
II. A doua etapǎ este «Mânia/ furia» (etapa «De ce tocmai eu?/ De ce tocmai mie?»)
Mânia poate fi îndreptată spre sine, spre supravieţuitori sau spre Dumnezeu (pierderea credinţei). De aceea, în această etapă terapeutul trebuie: să dea posibilitatea
pacientului să-şi exprime mânia şi revolta; să nu fie critic şi defensiv dacă furia este îndreptată împotriva lui; să descopere sentimentele reale, mascate de mânie ale pacientului.
III. A treia etapǎ «Negocierea» (etapa «Da, eu, dar…») exprimă acceptarea ideii morţii dar negocierea pentru a mai trăi puţin. Această etapă apare în momentul în care bolnavul incurabil renunţă la reacţiile sale de furie în favoarea adoptării unei conduite care ar putea prelungi cât mai mult perioada de timp rămasă până în momentul morţii.
În această etapă, terapeutul trebuie să accepte negocierea ca pe o reacţie firească şi să aibă o atitudine de aşteptare pentru a vedea ce se va întâmpla în continuare.
IV. A patra etapǎ «Depresia»: (etapa «Da, eu») este o reacţie obişnuită şi de înţeles, şi este însoţitǎ de recunoaşterea faptului că urmeazǎ actul final al morţii. Pacienţii sunt cuprinşi de sentimente de deznădejde şi disperare, şi devin adesea retraşi şi izolaţi.
V. Ultima etapǎ «Acceptarea/ resemnarea» (etapa «Da») este o etapă în care terapeutul şi pacientul trebuie să găsească împreună soluţii la diferitele probleme ce apar pe parcursul evoluţiei bolii.
Emoţiile pacientului pot fi privite şi ca un mozaic personal, prin intermediul căruia el răspunde într-un mod care îi este caracteristic la situaţia de boală, putând manifesta -spre deosebire de modelul anterior- unele emoţii simultan, astfel (4):
1. stadiul iniţial: «Faţă în faţă cu ameninţarea»În acest stadiu pacientul poate trece printr-o serie de emoţii
cum ar fi: frica, şocul, negarea, umorul, mânia, vinovăţia, anxietatea, îndoiala, negocierea, speranţa, disperarea. Acestea pot fi prezente în totalitate sau doar unele dintre ele.
2. stadiul cronic: «Conştientizarea şi recunoaşterea prezenţei bolii».
În stadiul cronic are loc diminuarea în intensitate a tuturor emoţiilor din stadiul iniţial şi poate apărea frecvent depresia ca urmare a conştientizării şi acceptării situaţiei în care se află pacientul.
3. stadiul final: «Acceptarea» este definit prin acceptarea morţii de către pacient.
După alţi autori durerea consecutivă pierderii implică câteva faze: stupoare; dor şi furie; dezorganizare; disperare; reorganizare (1,5).
J. W. Worden (1992) se referă la «scopurile jelirii» identificând: acceptarea realităţii pierderii; trecerea prin durere; adaptarea la noua realitate fără persoana decedată; reaşezarea emoţională a persoanei decedate în universul interior al supravieţuitorului şi reinvestirea în alte relaţii.
J. Culberg (1978) identifică următoarele faze: şocul, reacţiile la şoc (depresie, anxietate, disperare), prelucrarea durerii şi emoţiilor, reorientarea către alte aspecte ale vieţii.
Din experienţa clinică pot afirma că doar o parte dintre pacienţi traversează toate aceste stadii, marea majoritate devin depresivi într-o primă fază, ulterior acceptând realitatea diagnosticului şi implicându-se în tratament. O mică parte dintre pacienţi intră într-o fază de negare şi caută alţi terapeuţi care să le infirme acest diagnostic sau
RE
FER
ATE
19
BULETINUL ASOCIAŢIEI BALINT, VOL. 11., NR. 42, IUNIE 2009
RE
FER
ATE
acestora întrucât solicitările cărora trebuie să le facă faţă familiile pot fi uneori la fel de mari ca ale pacienţilor.
Membrii familiei bolnavului pot trece prin faze de evoluţie similare celor trăite de pacient în cursul bolii: şocul şi negarea, furia/mânia, negocierea, depresia, acceptarea şi resemnarea (8). Rudele apropiate suferă adesea de sentimente de vinovăţie şi de eşec, stadiile prin care trece familia după aflarea diagnosticului fiind: stare de şoc cu sentimente de culpabilitate, dezolare, disperare după care urmează o fază de căutare de soluţii şi o stare durabilă de echilibru (9).
Din experienţa mea clinică de până acum familiile dezvoltă mai des tulburări depresive cu manifestări clinice (tristeţe, plâns facil, inapetenţă, insomnii, sentimente de culpabilitate, etc.) sau mascate sub forma somatizărilor (modificări de ritm cardiac, crize de hipertensiune arterială, probleme de tranzit intestinal, probleme digestive, etc.).
Reacţia de doliu reprezintă de fapt reacţia psihologică şi emoţională faţă de pierdere, ecoul subiectiv al acesteia, ea depinzând atât de natura pierderii, de trăsăturile de personalitate şi copingul celui care suferă pierderea dar şi de reţeaua de suport social de care acesta dispune.
Reacţia normală de doliu se manifestă prin conştientizarea dureroasă a pierderii definitive, accese de disperare, plâns, suspin, căutarea persoanei pierdute, rememorări ale unor momente din trecut, idealizarea persoanei şi relaţiei (9). Simptomele care pot apare în perioada următoare sunt: tristeţe, apatie, gânduri obsesive, iluzii, halucinaţii hipnagogice, vise semnificative, tulburarea «în facsimil» (copierea acuzelor somatice ale decedatului) (5).Ulterior are loc o revizuire a concepţiilor, modelelor interioare şi rolurilor. Are loc o remaniere a personalităţii prin adoptarea unor noi roluri, reorganizarea planurilor de viitor, modificarea statutului, a raporturilor de putere şi control în familie.
apelează la terapeuţi specialişti în medicină complementară care le promit vindecarea.
În cazul pacienţilor oncologici pierderile pot fi permanente (amputaţii de sân, de colon, etc.) sau temporare (căderea părului, retragerea temporară din viaţă socială şi profesională pe parcursul tratamentelor, etc.). Reacţiile la pierderi variază în funcţie de vârsta pacienţilor, stadiul bolii, structura de personalitate a acestora, capacitatea de coping la boală. Astfel, pacienţii tineri acceptă mai greu pierderile mai ales dacă au familii, sunt activi social şi fac parte dintr-o reţea densă de statute şi roluri sociale. De asemenea, în stadiile curabile pierderile sunt mai uşor acceptate dacă pacienţii conştientizează faptul că aceste pierderi sunt esenţiale pentru supravieţuire. La pacienţii terminali atunci când aceştia îşi dau seama de ireversbilitatea bolii pierderile sunt de regulă însoţite de disperare, depresie şi deprimare. Pacienţii cu personalităţi echilibrate îşi mobilizează mai facil resursele interioare pentru a face faţă bolii, în schimb cei cu structuri de personalitate labile, anxioase, hipocondriace pot dezvolta tulburări psihopatologice care necesită tratament psihiatric.
În fazele terminale la pacienţi poate apărea frica (ce se va întâmpla după, frica de a merge în iad, teama de a fi îngropat într-un loc întunecos, etc.), retragerea şi izolarea (mai ales în cazul pacienţilor cu tonus fizic şi psihic foarte scăzut pentru care vizitele familiei şi prietenilor pot fi obositoare, în acest caz respectându-se dorinţa pacientului de a fi însoţit în aceste momente doar de persoanele pe care le vrea alături) sau poate exista o perioadă de profundă luciditate în care pacientul este conştient de ceea ce se întâmplă în jur, vorbeşte cu scop şi înţeles, îşi ia la revedere de la persoanele dragi.
În ceea ce priveşte problematica psihologică a familiilor pacienţilor oncologici, studiile efectuate au relevat aspecte interesante din punctul de vedere al evoluţiei psihologice a
Dans din Oaş
20
BULETINUL ASOCIAŢIEI BALINT, VOL. 11., NR. 42, IUNIE 2009
RE
FER
ATE
Există însă şi posibilitatea prelucrării necorespunzătoare a pierderii cu apariţia consecutivă a doliului complicat care se manifestă prin: tulburări psihosomatice (cefalee, acuze cardiace, tulburări gastro-intestinale, etc), tulburări disociative sau episod depresiv major. Reacţiile de doliu complicat pot apare în următoarele situaţii: morţi subite, traumatice; moartea unei persoane tinere; vulnerabilitatea premorbidă a persoanei care suferă pierderea; lipsa suportului social; anumite maladii (tulburări anxioase, depresii, alcoolism) (10).
Cele mai frecvente reacţii de doliu complicat sunt(1):1. Suferinţa întârziată defineşte situaţia în care persoana
care a suferit pierderea se implică în activităţi care să nu-i permită confruntarea cu realitatea, comportându-se ca şi când nimic nu s-ar fi întâmplat; suferinţa de pierdere are loc după o perioadă de latenţă de luni sau ani;
2. Suferinţa absentă se manifestă printr-o detaşare nefirească faţă de traumă şi consecinţele acesteia;
3. Suferinţa oscilantă se caracterizază prin exteriorizări periodice ale travaliului de doliu, după o aparentă acalmie;
4. Suferinţa cronică reprezintă o prelungire a travaliului de doliu peste perioada de un an manifestată prin: distimii, tulburări cronice de adaptare, tulburări somatoforme;
5. Suferinţa explodantă în care există o perioadă de latenţă în manifestarea durerii după care are loc o explozie de intensitate mare şi devastatoare a acesteia.
Există o serie de factori psihologici şi sociali care vor modela exprimarea durerii: cine a fost persoana (partener sau o rudă îndepărtată); natura relaţiei (armonioasă sau conflictuală); tipul morţii (aşteptată, suicidară, circumstanţe tragice); experienţe trecute ale pierderilor; personalitatea supravieţuitorului; existenţa altor stresuri asociate (6). S-au descris zece principii pentru a ajuta o persoană aflată în suferinţă să depăşească durerea (6):♦ actualizarea durerii (descrierea morţii, a circum-
stanţelor ei);♦ identificarea şi exprimarea sentimentelor (furie,
culpabilitate, etc);♦ detaşarea de cel decedat (luarea unor decizii,
schimbări);♦ înlocuirea emoţională a persoanei decedate (stabilirea
de noi relaţii);♦ stabilirea unui termen-limită pentru doliu;♦ reasigurarea normalităţii sentimentelor;♦ recunoaşterea diferenţelor individuale în procesul
durerii;♦ accesul la suport non-intensiv pe termen lung;♦ explorarea stilurilor de a face faţă, atrăgând atenţia
asupra riscurilor recurgerii la unele metode neadaptative (abuz de alcool, droguri, etc);
♦ identificarea durerii nerezolvate.Experienţa noastră clinică ne-a arătat faptul că în cazul
familiilor pacienţilor oncologici reacţia de doliu este mai intensă şi cu o exteriorizare mai mare (accese de disperare, plâns, etc.) mai ales în cazul pacienţilor tineri sau foarte tineri cu familii şi copii. Această pierdere este mai greu acceptată de familiile pacienţilor tineri deşi aceştia sunt conştienţi de suferinţele prin care trec pacienţii. Uneori
familiile privesc moartea ca pe o eliberare de suferinţă şi de aceea trec mai uşor peste momentul morţii.
În acest context, unii autori atrag atenţia asupra faptului că familiile pacienţilor oncologici necesită o conduită de suport din partea medicului, de a nu fi abandonate şi de a li se facilita un catharsis emoţional având rolul de a diminua reacţiile de doliu, de nelinişte şi culpabilitate (12). Discuţiile cu familia pot astfel oferi o eliberare şi preveni ca stările menţionate anterior să devină cronice.
Obiectivele sprijinului oferit persoanelor îndoliate (13):1. reducerea sentimentului de singurătate, preveni-
rea izolării;2. atenuarea suferinţei şi a sentimentelor negative;3. restabilirea echilibrului psihic şi a încrederii în sine.Sprijinul psihoemoţional contribuie la atenuarea
suferinţei şi recâştigarea autocontrolului prin (13):1. evocarea, verbalizarea experienţei dureroase;2. exprimarea sentimentelor;3. acceptarea realităţii;4. investigarea, identificarea resurselor şi alternativelor.În concluzie, atât în cazul pacienţilor cât şi în cazul
familiilor acestora se poate recurge la:1. Consiliere: este necesară în perioadele intens
stresante pentru pacient şi familie, pe tot parcursul tratamentului, având ca obiectiv adaptarea la noua situaţie prin învăţarea unor tehnici de rezolvare a problemelor care apar pe parcursul evoluţiei bolii.
2. Psihoterapie cognitiv-comportamentalăTerapia cognitiv-comportamentalǎ porneşte de la
premisa că tulburările emoţionale nu sunt cauzate de evenimentele în sine, ci de interpretările distorsionate pe care oamenii le dau acestora. Terapeutul, prin intermediul comunicării cu pacientul, îl ajută să-şi clarifice aceste distorsiuni şi să înveţe modalităţi mai realiste şi mai raţionale pentru trăirile sale. La pacienţii oncologici, terapia cognitiv-comportamentală este centrată pe terapia durerii cronice, controlul apetitului, efectele secundare asociate chimioterapiei (greaţa, voma), simptomele de anxietate şi depresie, ideile existente în societate asociate bolii. Tehnicile se pot aplica şi în cazul familiilor pacienţilor pentru a le învăţa să descopere gândurile negative şi interpretările eronate asociate bolii şi să le restructureze în mod adecvat pornind de la realităţile obiective.
3. Terapie de grup Grupurile suportive oferǎ pacienţilor informaţii care
sǎ-i ajute sǎ obţinǎ sentimentul capacitǎţii de control în legǎturǎ cu boala lor: informaţii privind boala, impactul tratamentului, dieta, exerciţii pentru recuperare, relaxare şi diminuare a stresului. Beneficiile participării la un grup de suport sunt: catharsis, reasigurare emoţională, contacte sociale, acces la informaţii, similaritatea problemei. Atmosfera protectoare a acestor grupuri stimulează încrederea participanţilor şi le oferă oportunitatea de a împartăşi experienţe dureroase cu alţii care au trecut prin experienţe similare. Interacţiunile şi interrelaţionarea cu alţi supravieţuitori facilitează trăirea reintegrării şi a universalităţii problemei cu care se confruntă. Participarea la grupurile de suport scade sentimentele de izolare şi

21
BULETINUL ASOCIAŢIEI BALINT, VOL. 11., NR. 42, IUNIE 2009
RE
FER
ATE
Rezumat:Articolul subliniază că de-alungul istoriei
intelectuale occidentale, intelectuali de seamă au admis că reprezentarile, gândurile, sentimentele, imaginile, arta şi ştiinţa au purces dintr-un teritoriu necunoscut, inconştient. O sumedenie de speculaţii au fost emise despre acest „domeniu” şi despre calitaţile sale”vii”. Chiar si inainte de Freud, dar mai ales după aceea, medici, psihologi şi chiar vindecători, care tratau bolnavi cu diverse suferinţe, au încercat să înţeleagă natura domeniului inconştientului.Privind munca de grup Balint prin fereastra Johari, o putem percepe ca pe un proces unde atât medicul cât şi pacientul fac cunoştinţă cu domeniul inconştientului, îl explorează şi incearcă să-l aprofundeze ideatic. Această incorporare a gandirii clinice speculative îmbunătăţeşte evaluarea şi tratamentul pacientului, permiţând medicului să îşi însuşească o identitate creativă nouă. In mod epistemologic, explorarea inconştientului în munca de grup Balint, creează cadrul gândirii clinice speculative, printr-un proces de muncă de grup care îmbunătăţeşte nu numai nivelul de îngrijire medicală, ci şi bună-starea psihologică a medicului.
Cuvinte cheie: inconştient, stare de bine a medicului
Summary:Throughout Western intellectual history, as
briefly outlined in the article, wise individuals have admitted that insights, thoughts, feelings, images, art and science emerged from an unknown, unconscious territory. Much speculation about that territory and its living qualities has been formulated. Both before and after Freud, physicians, psychologists, and healers have attempted to understand the nature of that unconscious territory in treating the sick and suffering. Balint group work, as seen through the Johari window, has been described as a process wherein that unconscious territory in both doctor and patient is acknowledged, explored and imaginatively entertained. This incorporation of speculative, clinical reasoning enhances assessment and treatment of the patient, and allows a creative, evolving identity of the physician to emerge. Reclaiming the unconscious in Balint group work, epistemological frames clinical reasoning and speculation in a working group process that improves medical care and physician well-being.
Key words: unconscious territory, physician well-being
INTRODUCTION
Given our most systematic, professional and attentive efforts, the world around us and within always seem unexpectedly to open before us to
RECLAIMING THE UNCONSCIOUS IN BALINT GROUP WORK
Alan H Johnson PhD Medical University of South Carolina,Charleston, SC, USA
alienare, contribuie la conştientizarea şi acceptarea pierderii şi durerii, exprimarea emoţiilor negative de culpabilitate şi neajutorare, interiorizarea şi prelucrarea psihică a experienţei dureroase (13). Se poate apela şi la psihoterapie individualizată sau în cazuri mai grave la consult psihiatric specializat şi medicaţie psihotropă.
Bibliografie: 1. Parkes C. M., Bereavement în D. Doyle, G. Hanks, N. Mac
Donald, (eds.) Oxford textbook of palliative medicine, Oxford, Oxford Medical Publications, 1993
2. Mitrofan I., Buzducea D. 1999, Psihologia pierderii şi terapia durerii, Bucureşti, Ed. Albedo
3. Kübler-Ross E. 1969, On death and dying, New York, MacMillan
4. Buckman R., How to break bad news: a guide for health-care proffesionals, London, Pan Books, 1994
5. J. Bowlby J., Attachment and loss: loss, sadness and depression, New York, Basic Books, 1980
6. Worden J. W., Weisman M., Grief counselling and grief
therapy. A handbook for mental health practitioner, London, Tavistock Routledge, 1992
7. Culberg J., Krisen und Krisentherapie, Psychiatrische Praxis, 5/1978, p. 25-34
8. Kübler-Ross, Les derniers instants de la vie, Geneve, Ed. Labors et Fides, 1975
9. Athanasiu A. 1998, Elemente de psihologie medicală, Bucureşti, Ed. Medicală
10. Micluţia I., Perju-Dumbravă L., Florea M., Pierderea, doliul normal şi patologic din perspectiva medicinei paliative, «Revista Română de Sănătate Mintală, 14, nr. 2/2000, p. 8-10
11. Stroebe M. S., Stroebe W., Hanson R.O., 1993, Handbook of bereavement. Theory, research and intervention, Cambridge, Cambridge University Press,1993
12. Jeammet Ph.., Reynaud M., Consoli S, Psychologie médicale, Ed. Masson, 1993
13. Görög I., Asistenţa hospice a pacienţilor cu boli incurabile, în «Buletinul Asociaţiei Balint» (Miercurea-Ciuc, Tipografia Alutus), 6, nr. 24/ decembrie 2004, p. 3-10

22
BULETINUL ASOCIAŢIEI BALINT, VOL. 11., NR. 42, IUNIE 2009
RE
FER
ATE
something new, something unknown. Abhorring not knowing, we fashion a hypothesis, a belief, a myth or a silent refusal to declare our response to the novel and continue to chop wood and carry water, or in the case of medicine, to see the next patient. However, that not knowing or not being conscious catches up with us, and its shadow falls across our practice when, despite our best professional efforts, care for the patient just doesn’t seem to be effective or satisfying. It is just such a case that bubbles up in the Balint group. Then, many small lights begin to flash into the darkness of patient, doctor and their relationship What has been left unspoken, unfelt, unthought-of, and unimagined, this shadow crossing the doctor’s path, is brought into the light. What has been unconscious is, in part, reclaimed.
This paper is not an attempt to revive a psycho-analytic metaphysics of the unconscious, or in a more general sense, an attempt to propose some particular theoretical structure of the unconscious. Rather, this paper is an attempt to honor how the unconscious of the physician and that of the patient are explored in Balint group work in order to create a broader field of consciousness for improved patient care and enhanced physician satisfaction. The paper will begin with a brief review of how the unconscious entered Western thought, and next move to illuminate the particular way in which the unconscious is dealt with in the Balint group process. The Johari awareness model will be used to illustrate how the unconscious is illuminated within the Balint group.
THE UNCONSCIOUS
All learning presupposes an unknown. When that unknown centers on the person who is assumed to have the capacity of consciousness, the unknown is called the unconscious. It is this subjective field of learning on which Balint work focuses. I will begin with the historical research of Whyte: ‘words expressing awareness and self-awareness first emerged in the English and German languages during the 17th century.’1 Whyte further notes that it is interesting to observe that ‘conscious’, from its Latin source, meant ‘to know with’. It came, however, to mean ‘to know in oneself, alone’.
By 1670–1730 Whyte found that no fewer than eight writers in the English, German, French and Italian languages had ‘... published ideas overlapping in some degree with our contemporary conception of unconscious mental processes’.1 These historical findings are cited to alert the reader to the far-reaching dimensions of the unconscious in science, philosophy, religion, medicine and art. What influences illness, memory, moods, sleep, dreams, intentions, imaginations, beliefs, perceptions and reason itself has long been noted as having its origins within and beyond consciousness.
Some of the more discriminating ways in which the unconscious mind has been interpreted are concisely summarized by Whyte in Table I. It would be helpful in reviewing Table 1 to analyze in what way(s) the physician and patient are oriented to the unconscious, and to appreciate how this orientation is manifest in forming what each of them considered to

23
BULETINUL ASOCIAŢIEI BALINT, VOL. 11., NR. 42, IUNIE 2009
be their normal (rational) way of communicating and behaving.
The mystic believes in an unknown God, the thinker and scientist in an unknown order; it is hard to say which surpasses the other in non-rational devotion.
It is such ‘devotion’ that may put a doctor and patient on very different channels of communication. Until this non-rational devotion, this unconscious orientation, is made conscious the physician will find change in thinking, feeling and behavior impossible.
For a far more expansive, personalized and culturally contextualized history of the unconscious from ancient times to the mid-20th-century the reader would benefit greatly from a study of the Swiss medical historian, Henri F. Ellenberger’s magnum opus, The Discovery of the Unconscious: The History and Evolution of Dynamic Psychiatry, published in 1970.2 A second book of his collected essays, Beyond the Unconscious followed in 1993.
ENGLISH PHYSICIANS AND THE UNCONSCIOUS
A group or ‘school’ of English physicians beginning with Sir W. Hamilton (1788–1856) and W. B. Carpenter (1813-1885) developed a doctrine of the unconscious as part of their professional responsibility in understanding the patient as a ‘body-mind unity’. To these pragmatic monists there was nothing strange or challenging in the idea of unconscious factors; whether one chooses to call them physiological or mental, they were indubitably at work.1
Hamilton and Carpenter were succeeded by many, the most important of whom were: J. D. Morel, J. C. Brodie, H. Maudsley, T. Lavcock and D. H. Tuke. Maudsley (1835–1918) summarized the ideas of the English school in his Physiology and Pathology of the Mind, 1867. He said:
The most important part of mental action, the essential process on which thinking depends, is unconscious mental activity.
Whyte points out that it is interesting that in 1874, the year Freud entered the University; Brentano published in Vienna a thorough examination of Maudsley’s views. Freud attended Brentano’s lectures for two years.
At this point it should be clear that the unconscious was a concept interwoven in the intellectual and medical culture of Europe and England. The social diffusion of study of the unconscious is conspicuously manifest in 1868 with the publication of von Hartmann’s The Philosophy of the Unconscious. By 1882 it was in its ninth German edition; it was translated into French in 1877 and into English by 1884. This encyclopedic work, 1100 pages in the 1931 English translation, covered 26
topics some of which are: neural physiology, reflexes, curative processes, sexual love, feeling, morality, history, etc. It would seem apparent that the medical community long before the time of Freud was seriously considering both in England and on the Continent the unconscious as an important dimension of life and clinical practice.
FREUD’S LEGACY
Whyte contends that from 1752 to the present a shift in European philosophical and scientific thinking was evident. This was a movement toward ‘process concepts’ and away from ‘static concepts’. He saw Darwin and Freud as products and promoters of this transformation. Whyte felt that Darwin knew he was ‘extending the scope of reason by helping to make it less static’. With Freud the story was different.
...Freud did not realize that he was destroying rationalism by showing that reason, though essential to understanding, did not control thought or behavior.1
Whyte also noted that Freud’s conceptualization of the unconscious neglected one of its most important aspects. Freud had remained almost silent on the unconscious mental processes underlying ”the appearance of novelty in all creation, imagination and invention.” Fortunately this shortsightedness did not hamper the routine incorporation of creative, clinical speculation in the future development of Balint group work.
It is not my intention to diverge into an extensive criticism or extolment of Freud’s far-reaching influence. Many others have addressed that topic: Eric Fromm4, Bruno Bettelheim5, Calvin Hall6, Paul Ricoeur7, Paul Roazen8, and Liliane Frey-Rohn’ to name a few. Rather I should note that through his work and personality he created around himself a circle of persons, several of whom would touch the life of Michael Balint and bring him into a long and productive career as a writer, teacher, executive leader and training analyst in the psychoanalytic tradition10. Within this circle, and beyond it, an energized debate, if not overtly divisive intellectual and emotional struggle would continue over the question of the structure and dynamics of the unconscious.
JOHARI AWARENESS MODEL
The Johari window is a graphic model of interpersonal behavior ideally suited to describe and identify the dynamic behaviors of individuals and groups. It was developed in 1955 by professors Joseph Luft and Harry Ingham.11 Underlying the model are several assumptions:
1. Holistic units of behavior are more important in understanding human behavior then elemental units
RE
FER
ATE
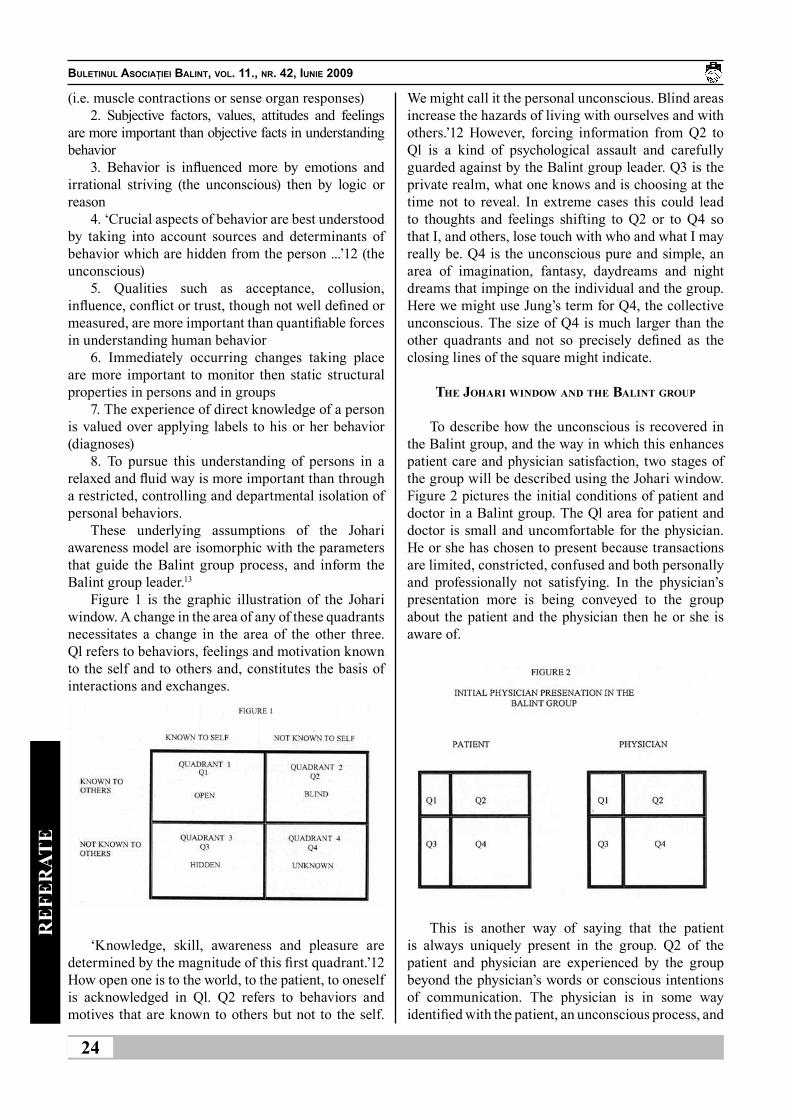
24
BULETINUL ASOCIAŢIEI BALINT, VOL. 11., NR. 42, IUNIE 2009
RE
FER
ATE
(i.e. muscle contractions or sense organ responses)2. Subjective factors, values, attitudes and feelings
are more important than objective facts in understanding behavior
3. Behavior is influenced more by emotions and irrational striving (the unconscious) then by logic or reason
4. ‘Crucial aspects of behavior are best understood by taking into account sources and determinants of behavior which are hidden from the person ...’12 (the unconscious)
5. Qualities such as acceptance, collusion, influence, conflict or trust, though not well defined or measured, are more important than quantifiable forces in understanding human behavior
6. Immediately occurring changes taking place are more important to monitor then static structural properties in persons and in groups
7. The experience of direct knowledge of a person is valued over applying labels to his or her behavior (diagnoses)
8. To pursue this understanding of persons in a relaxed and fluid way is more important than through a restricted, controlling and departmental isolation of personal behaviors.
These underlying assumptions of the Johari awareness model are isomorphic with the parameters that guide the Balint group process, and inform the Balint group leader.13
Figure 1 is the graphic illustration of the Johari window. A change in the area of any of these quadrants necessitates a change in the area of the other three. Ql refers to behaviors, feelings and motivation known to the self and to others and, constitutes the basis of interactions and exchanges.
‘Knowledge, skill, awareness and pleasure are determined by the magnitude of this first quadrant.’12 How open one is to the world, to the patient, to oneself is acknowledged in Ql. Q2 refers to behaviors and motives that are known to others but not to the self.
We might call it the personal unconscious. Blind areas increase the hazards of living with ourselves and with others.’12 However, forcing information from Q2 to Ql is a kind of psychological assault and carefully guarded against by the Balint group leader. Q3 is the private realm, what one knows and is choosing at the time not to reveal. In extreme cases this could lead to thoughts and feelings shifting to Q2 or to Q4 so that I, and others, lose touch with who and what I may really be. Q4 is the unconscious pure and simple, an area of imagination, fantasy, daydreams and night dreams that impinge on the individual and the group. Here we might use Jung’s term for Q4, the collective unconscious. The size of Q4 is much larger than the other quadrants and not so precisely defined as the closing lines of the square might indicate.
THE JOHARI WINDOW AND THE BALINT GROUP
To describe how the unconscious is recovered in the Balint group, and the way in which this enhances patient care and physician satisfaction, two stages of the group will be described using the Johari window. Figure 2 pictures the initial conditions of patient and doctor in a Balint group. The Ql area for patient and doctor is small and uncomfortable for the physician. He or she has chosen to present because transactions are limited, constricted, confused and both personally and professionally not satisfying. In the physician’s presentation more is being conveyed to the group about the patient and the physician then he or she is aware of.
This is another way of saying that the patient is always uniquely present in the group. Q2 of the patient and physician are experienced by the group beyond the physician’s words or conscious intentions of communication. The physician is in some way identified with the patient, an unconscious process, and

25
BULETINUL ASOCIAŢIEI BALINT, VOL. 11., NR. 42, IUNIE 2009
so carries this aspect of the patient, ‘undiagnosed’ and unconscious, into the group. Q3 and Q4 of patient and doctor are somewhat similar for the rest of the group, but certainly not identical. Therein lies the potential for growth: new insights, feelings and behaviors.
After the physician’s presentation, and when the presenter has sat back, allowing the group to temporarily assume care of the patient, a new picture emerges. This new configuration of the group looks like Figure 3.
The Ql area of patient and presenter greatly expands because many in the group have articulated their own unique, picture of the patient and their own unique declarations of what they would be thinking, feeling and doing for or to the patient. Some would want to discharge her or him. Others would desire to know more about past medical history, family and social history. They are drawn to the patient. What the presenter thought her or his role as a physician ought to be is now silhouetted against other alternative roles. Ql has now been enlarged by the group and potentially for the presenting physician. What the presenting physician was unconsciously thinking, feeling, or imagining, Q2, may now have been articulated by peers empathizing with his or her role. As well, what he or she has not shared about personal responses to the patient, Q3, may have been spoken by others in the group and will now have become part of Ql.
Concurrently with the expanding area Ql of the presenter, is the expanding area Ql of the patient. The group has imagined, conjectured, inferred and reasoned her or him to be more than was initially presented. What she or he was possibly hiding from the
doctor, Q3, and what she may have been unconscious of in herself, Q2, or what was impinging on her due to her circumstances, Q4, has in part been brought to consciousness in the group. Both a personal and collecting unconscious have in part been recovered.
The buoyant effect of this consciousness rising on the presenter, patient and their relationship is the power of the Balint group. How the presenter decides to swim with the rising tide of consciousness is left to his or her initiative. Often the report of the presenter in following sessions is that things just seemed better or easier on our last encounter. How the partial recovery of the unconscious affects every presenter and other group member is different on each meeting. The group’s treatment of the presenter wrestles with the same unconscious currents as the presenter’s treatment of the patient. Objective assessment of the case is the delusion; a consensual probability is a more likely reality.
DiscussionEllenberger states ‘...since time immemorial there
have been two approaches to healing: one by use of rational means and the other by mobilizing irrational forces.’3 Too frequently Balint group work which acknowledges irrational forces and invites imaginative, clinical speculation, has prejudicially been judged to conjure up irrational forces in a cult-like gathering of doctors. I believe the above presentation of the Balint group process viewed through the Johari window should clarify how an imaginative process, honoring unconscious thoughts, feelings and behaviors, can be acknowledged and incorporated into a rational assessment of doctors, patients and their relationships. Acknowledging unconscious processes as well as conscious, rational processes is essential to the well-balanced assessment and treatment of patients and the well balanced life of the physician. Every dogmatism whether of science or religion constricts the conscious meeting arena of doctor and patient, Ql, and moves medical practice toward a devitalized ritual. Treatment by protocol without the person of the physician and the patient is sterile and recovery of the unconscious is categorically excluded.
Luft asserts: ‘Intrapersonal and interpersonal affairs are inextricably united.’ He goes on to say: ‘...identity and relationships are sufficiently intertwined so that it makes sense to consider them together.’12 The most central question that is always shuttling between consciousness and the unconscious in Balint group work is: what kind of doctor am I? Medical school may teach what a doctor is to do. Where, with whom, and how does the young doctor begin to sculpt consciously what he or she is to be?
RE
FER
ATE

26
BULETINUL ASOCIAŢIEI BALINT, VOL. 11., NR. 42, IUNIE 2009
RE
FER
ATE
It is through the transactions of the secure and supporting Balint group as the Blind, Q2, and Hidden, Q3, areas of each member are thought-by-thought and feeling-by-feeling spoken aloud by a peer that some fuller image of their individualized, personal physician begins to emerge. Concurrently, thought-by-thought and feeling-by-feeling an older, idealized image of who they thought their personal physician was begins a morphogenesis.
In recovering the unconscious, both uniquely personal attributes as well as ancient, archetypal attributes of the healer, begin to crystallize for the individuals of the group. Only indirectly are the members of the group drawn to this realization when confronting the leader’s question, ‘What kind of doctor does this patient need?’ In attempting an answer to this question one’s own hand, card at a time, will be turned over. The process continues throughout one’s professional life. Q4 is a vast territory with an ever receding frontier. Recovery of the unconscious is a recovery of openness to the body-mind connection without attaching medical or psychiatric labels and hearing the symptoms speak the truth of the patient’s existential condition. Recovery of the unconscious is also the physician being open to and aware of the feelings and thoughts that arise in him or her, as well as the discriminating clinical thoughts which are an immediate part of the patient encounter.
I will close with the words of one of the earliest, medical psychologists, Carl Gustav Cams (1789–1869), privileged Dresden court physician to the king of Saxony, professor of gynecology, artist and author of many works both scientific and philosophical. From his 1846 book, Psyche, these words:
The unconscious is the primordial source of life....the understanding of the unconscious in
consciousness is everywhere the last and highest aim of science...’
References1. Whyte,L. L. The Unconscious Before Freud.
Garden City, New York: Anchor Books, 1962. 2. Ellenberger H. F. The Discovery of the Unconscious:
The History and Evolution of Dynamic Psychiatry. New York: Basic Books, Inc., 1970.
3. Ellenberger H. S. Beyond the Unconscious: Essays of Henri F. Ellenberger in the History of Psychiatry. Princeton, New Jersey: Princeton University Press, 1993.
4. Fromm E. Greatness and Limitations of Freud’s Thought. New York: A Mentor Book, New American Library, 1980. 5. Bettelheim B. Freud and Man’s Soul. New York: Vintage Books, 1984.
5. Hall CS. A Primer of Freudian Psychology. New York: A Mentor Book, 1954.
6. Ricoeur P. Freud and Philosophy: An Essay on Interpretation. New Haven: Yale University Press, 1970.
7. Roazen P. Freud and His Followers. New York: A Mentor Book, Now American Library, 1974.
8. Frey-Rohn L. From Freud to Jung: A Comparative Study of the Psychology of the Unconscious. New York: A Delta Book, 1974.
9. Johnson A. H. ‘The Balint Movement in America’. Fam Med 2001; 33(3): 174-7.
10. Luft J. Group Processes: An Introduction to Group Dynamics. Palo Alto, California: Mayfield Publishing Co., 1970.
11. Luft S. Of Human Interactions. Palo Alto, California: National Press Books, 1969.
12. Johnson A. H., Nease DE, Milberg LC, Addison RB.. ‘Essential Characteristics of Effective Balint Group Leadership’. Fam Med 2004; 36 (4):253-9.
13. Carus C. G. Psyche: On the Development of the Soul, Part One, The Unconscious, trans. Renata Welch. New York: Spring Publications, 1970.
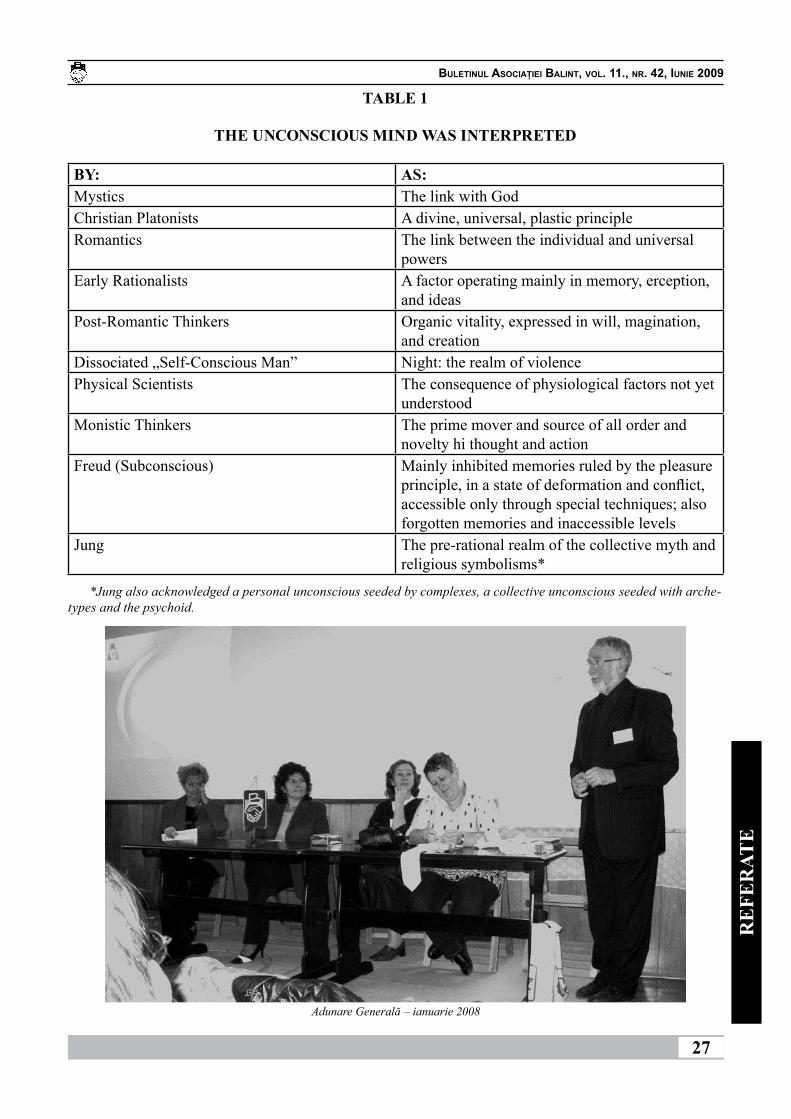
27
BULETINUL ASOCIAŢIEI BALINT, VOL. 11., NR. 42, IUNIE 2009
BY: AS:Mystics The link with GodChristian Platonists A divine, universal, plastic principleRomantics The link between the individual and universal
powersEarly Rationalists A factor operating mainly in memory, erception,
and ideasPost-Romantic Thinkers Organic vitality, expressed in will, magination,
and creationDissociated „Self-Conscious Man” Night: the realm of violencePhysical Scientists The consequence of physiological factors not yet
understoodMonistic Thinkers The prime mover and source of all order and
novelty hi thought and actionFreud (Subconscious) Mainly inhibited memories ruled by the pleasure
principle, in a state of deformation and conflict, accessible only through special techniques; also forgotten memories and inaccessible levels
Jung The pre-rational realm of the collective myth and religious symbolisms*
*Jung also acknowledged a personal unconscious seeded by complexes, a collective unconscious seeded with arche-types and the psychoid.
TABLE 1
THE UNCONSCIOUS MIND WAS INTERPRETED
RE
FER
ATE
Adunare Generală – ianuarie 2008
28
BULETINUL ASOCIAŢIEI BALINT, VOL. 11., NR. 42, IUNIE 2009
ŞTIRI DIN VIAŢA ASOCIAŢIEI
13-15 martie, Poiana Braşov: curs pentru lideri de grup Balint cu Michel Delbrouck din Belgia.
11 aprilie, Miercurea Ciuc: şedinţa extraordinară a Biroului Asociaţiei pentru pregătirea materialului solicitat de către Biroul Federaţiei la Chicago.
17-19 aprilie: am participat la şedinţa de Birou a Federaţiei Internaţionale Balint din Chicago, care a avut loc în cadrul unui Weekend al Asociaţiei Balint din SUA. Am expus etapa în care se află organizarea Congresului Internaţional din 5-9 Septembrie din Poiana Braşov şi am răspuns la multiplele întrebări ivite din partea membrilor Biroului.
8-10 mai: la Ocna Şugatag a avut loc al 6-lea Weekend Balint (al 3-lea de rang naţional) sighetean şi şedinţa ordinară a Biroului Asociaţiei. Gazdele noastre în frunte cu familia dr. Árvai György şi Zsófia au fost şi mai pricepuţi într-ale organizării ca la celălalte întâlniri anterioare. Grupul de dansatori oăşeni, copii de diferite vârste şi lungimi, muzica orchestrei din zonă ne-a delectat pe deplin. Cazurile prezentate ne-au pus pe deplin la contribuţie minţile tuturor.
PLANURI DE VIITOR:
Se anulează Weekendul Interjudeţean din Brăila, din 26-28 iunie.
5-9 septembrie 2009: al XVI-a Congres Internaţional Balint, Poiana Braşov. 28 credite EMC. După 10 ani de insistenţe în sfârşit ni s-a acordat dreptul organizării CONGRESULUI INTERNAŢIONAL BALINT din 2009. Este o recunoaştere a activităţii şi viabilităţii Asociaţiei Balint din România.
Am speranţa că veţi reuşi să participaţi într-un număr mare la acest eveniment plănuit a fi unul care să ne ducă vestea (cea bună!) în lume.
Facem eforturi ca toţi participanţii să plece plini de emoţii plăcute şi reîncărcaţi sufleteşte.
Biroul Asociaţiei a decis oferirea unei sponsorizări pentru participanţi în valoare totală de 10.000 RON. CLAUZA ÎNSCRIERII: este obligatorie prezenţa pe tot parcursul congresului, deoarece grupurile mici vor avea o componenţă fixă din care dacă lipseşte cineva, ceilalţi imediat se simt frustraţi, considerând că respectivul coleg a plecat din cauză că a fost jignit de către membrii grupului.
Taxa de participare pentru colegii din România (indiferent de categoria profesională) este de 255 Euro dacă participă la coctailul de primire sau 225 dacă nu participă. (După data de 30 iunie se aplică taxa de 340 respectiv 310 Euro). Înregistrarea se face on-line dar se
plăteşte doar taxa specificată aici nu cea arătată pe site. Cont lei: RO15CECEHR0143RON0029737, CEC MIERCUREA CIUC, Titular: Fundaţia CRY FOR HELP.
Pentru însoţitori se percepe aceeaşi taxă cu a străinilor, de 195 Euro.
Cazare mai ieftină decât cele cuprinse pe site (45 Euro camera cu 2 paturi, cu micul dejun) se poate solicita personal (managerul nu acceptă preţ negociat, deci nu am contractat serviciile hoteliere) în limita numărului de 30 de camere la motelul Căprioara, vecină cu Monterai sau la alegerea fiecăruia dintre voi la alte locaţii.
ADRESA SITE-LUI pentru alte amănunte:www.balintcongress2009.com
6-8 noiembrie 2009: a XVI-a Conferinţă Naţională Balint. Casa de Studii Jakab Antal, Şumuleu-Ciuc, 20 credite EMC.
11-13 decembrie 2009: Weekend Interjudeţean cu Prerevelion Balint, Satu-Mare. 9 credite EMC.
15-17 ianuarie 2010: Weekend Naţional cu Postrevelion Balint, Roman
În speranţa întâlnirii cu balintienii înscrişi în Asociaţie, dar NU NUMAI, vă doresc toate cele bune,
Dorim să stabilim schimburi cu alte publicaţii.On désiré établir l’échange avec d’autres
publications.We wish to establish exchange with other
publications.Wir wünschen mit anderen Herausgaben den
Austausch einzurichten.Desideriamo stabilire cambio con alte
publicazioni.Déseamos establecer intercambio con otras
publicaciones.ŞTIR
I DIN
VIAŢA
ASO
CIAŢI
EI