ORIGINAL ARTICLES - tmj.ro · PDF fileORIGINAL ARTICLES ORTHOPAEDIC NON-SURGICAL TREATMENT IN...
8
Narcis F. Tepeneu et al 215 ORIGINAL ARTICLES ORTHOPAEDIC NON-SURGICAL TREATMENT IN CHRONIC HAEMOPHILIC JOINT CONTRACTURES OF THE KNEE Narcis F. Tepeneu 1 , Pavel Tepeneu 1 , Margit Serban 2 , Carmen Petrescu 2 , Laura Pop 2 , Barbara Popescu 1 , Rodica Badeti 1 REZUMAT Introducere: Artropatiile cronice hemofilice, în special localizate la nivelul articulaţiei genunchiului , uni- sau bilateral, generează redori în flexie cu severă afectare locomotorie. Indiferent de tipul hemofiliei, severitatea bolii, modificările artrozice, gradul de atrofie şi retracţie musculo-tendinoasă pot fi selectate cazuri cu indicaţie de tratament ortopedic – nesângerand. Material și metodă: Se prezinta un lot de 11 pacienţi cu hemofilie A, cu o medie de vârstă de 18 ani, trataţi în intervalul 2000-2009. Toti pacienţii au prezentat forma severă de hemofilie tip A, 2 pacienţi prezentând titru ridicat de inhibitori pentru factor VIII. Gradul de flexie a fost intre 30 si 90°, localizarea artropatiei la genunchi, la 5 pacienţi unilateral si la 6 pacienţi bilateral. Lucrarea prezintă detailat modalitatea şi secvenţialitatea procedurilor terapeutice ortopedice instituite sub protecţie de medicaţie substitutivă specifică. Rezultate și discuţii: Obiectivele tratamentului au fost repoziţionarea genunchiului în extensie sau flexie de maxim 10°, obiectiv atins prin redresări succesive , de regulă in 2-3 şedinţe . Ulterior rezultatele au fost consolidate prin ortezare şi proceduri de fiziokinetoterapie. Nu am înregistrat complicaţii locale sau generale. Apreciem rezultatele la distanţa ca fiind foarte bune la 3 cazuri, bune la 7 cazuri si satisfacătoare la 1 caz. Concluzii: Tratamentul ortopedic nesângerând este o alternativă valoroasă de management al redorilor articulare în flexie la pacienţii cu artropatie hemofilică. Tratamentul este bine suportat, nu antrenează complicaţii majore, aduce un incontestabil beneficiu funcţional şi este incomparabil superior sub raport preţ/eficienţă faţă de tratamentul sângerând. Cuvinte cheie: hemofilie, artropatie hemofilică, contractura in flexie a genunchiului, tratament ortopedic-nesângerând ABSTRACT Background: Chronic haemophilic arthropathies , especially those affecting the knee , uni - or bilateral, generate severe mobility loss with flexum immobilisation. Regardless of the type of haemophilia , the degree of severity , the arthrotic modifications and the degree of musculo-tendinous retraction there are patients which can be selected for orthopaedic – non-surgical treatment. Material and methods: We present a group of 11 patients with haemophilia type A, with a mean age of 18 years, treated in our Clinic between 2000 and 2009. All patients had a severe form of haemophilia type A , 2 patients presenting high level of inhibitors. The degree of flexum was between 30-90°, and the arthropathy affected one knee in 5 patients and both knees in 6 patients. The paper presents in detail the methods and secventiality of therapeutic orthopedic procedures performed under specific substitutive therapy. Results and discussions: The objective of treatment was repositioning of the knee in extension or flexum of maximum 10°, which was done by repeated reduction and splinting, usually in 2-3 sessions. The results were consolidated by special orthosis and physiokinetotherapy. We did not encounter any local or general complications. We appreciate the results as being very good in 3 cases, good in 7 cases and satisfactory in 1 case. Conclusions: The orthopaedic non-surgical treatment is a valuable alternative in the management of chronic haemophilic arthropathy. The treatment is usually well tolerated, without major complications, has a great functional benefit and has a very good cost/efficiency rate compared to the surgical treatment. Key Words: hemophilia, chronic hemophilic arthropathy, flexum contracture of the knee, orthopaedic – nonsurgical treatment Received for publication: Nov. 30, 2009. Revised: Jul. 30, 2010. 1 Clinic of Pediatric Surgery and Orthopaedics, 2 III rd Pediatric Clinic, Louis Turcanu Emergency Children’s Hospital, Timisoara Correspondence to: Dr. Narcis F. Tepeneu, Clinic of Pediatric Surgery and Orthopaedics, Louis Turcanu Emergency Children’s Hospital, Timisoara, Tel. +40- 256-203373. Email: [email protected] INTRODUCTION Joint contractures in patients with haemophilia are the result of recurrent intra-articular and intramuscular bleeding episodes. Approximately 50% of people with severe haemophilia (factor VIII or IX level <1 IU/ dL) have articular contractures >10º, which can be disabling, causing decreased mobility and functional impairment. Fernández-Palazzi and Batistella reported having found a knee contracture in every patient they assessed in hemophilia centers. 1 Atkins et al reported a
Transcript of ORIGINAL ARTICLES - tmj.ro · PDF fileORIGINAL ARTICLES ORTHOPAEDIC NON-SURGICAL TREATMENT IN...

Narcis F. Tepeneu et al 215
ORIGINAL ARTICLES
ORTHOPAEDIC NON-SURGICAL TREATMENT IN CHRONIC HAEMOPHILIC JOINT CONTRACTURES OF THE KNEE
Narcis F. Tepeneu1, Pavel Tepeneu1, Margit Serban2, Carmen Petrescu2,Laura Pop2, Barbara Popescu1, Rodica Badeti1
REZUMATIntroducere: Artropatiile cronice hemofilice, în special localizate la nivelul articulaţiei genunchiului , uni- sau bilateral, generează redori în flexie cu severă afectare locomotorie. Indiferent de tipul hemofiliei, severitatea bolii, modificările artrozice, gradul de atrofie şi retracţie musculo-tendinoasă pot fi selectate cazuri cu indicaţie de tratament ortopedic – nesângerand. Material și metodă: Se prezinta un lot de 11 pacienţi cu hemofilie A, cu o medie de vârstă de 18 ani, trataţi în intervalul 2000-2009. Toti pacienţii au prezentat forma severă de hemofilie tip A, 2 pacienţi prezentând titru ridicat de inhibitori pentru factor VIII. Gradul de flexie a fost intre 30 si 90°, localizarea artropatiei la genunchi, la 5 pacienţi unilateral si la 6 pacienţi bilateral. Lucrarea prezintă detailat modalitatea şi secvenţialitatea procedurilor terapeutice ortopedice instituite sub protecţie de medicaţie substitutivă specifică. Rezultate și discuţii: Obiectivele tratamentului au fost repoziţionarea genunchiului în extensie sau flexie de maxim 10°, obiectiv atins prin redresări succesive , de regulă in 2-3 şedinţe . Ulterior rezultatele au fost consolidate prin ortezare şi proceduri de fiziokinetoterapie. Nu am înregistrat complicaţii locale sau generale. Apreciem rezultatele la distanţa ca fiind foarte bune la 3 cazuri, bune la 7 cazuri si satisfacătoare la 1 caz. Concluzii: Tratamentul ortopedic nesângerând este o alternativă valoroasă de management al redorilor articulare în flexie la pacienţii cu artropatie hemofilică. Tratamentul este bine suportat, nu antrenează complicaţii majore, aduce un incontestabil beneficiu funcţional şi este incomparabil superior sub raport preţ/eficienţă faţă de tratamentul sângerând.Cuvinte cheie: hemofilie, artropatie hemofilică, contractura in flexie a genunchiului, tratament ortopedic-nesângerând
ABSTRACTBackground: Chronic haemophilic arthropathies , especially those affecting the knee , uni - or bilateral, generate severe mobility loss with flexum immobilisation. Regardless of the type of haemophilia , the degree of severity , the arthrotic modifications and the degree of musculo-tendinous retraction there are patients which can be selected for orthopaedic – non-surgical treatment. Material and methods: We present a group of 11 patients with haemophilia type A, with a mean age of 18 years, treated in our Clinic between 2000 and 2009. All patients had a severe form of haemophilia type A , 2 patients presenting high level of inhibitors. The degree of flexum was between 30-90°, and the arthropathy affected one knee in 5 patients and both knees in 6 patients. The paper presents in detail the methods and secventiality of therapeutic orthopedic procedures performed under specific substitutive therapy. Results and discussions: The objective of treatment was repositioning of the knee in extension or flexum of maximum 10°, which was done by repeated reduction and splinting, usually in 2-3 sessions. The results were consolidated by special orthosis and physiokinetotherapy. We did not encounter any local or general complications. We appreciate the results as being very good in 3 cases, good in 7 cases and satisfactory in 1 case. Conclusions: The orthopaedic non-surgical treatment is a valuable alternative in the management of chronic haemophilic arthropathy. The treatment is usually well tolerated, without major complications, has a great functional benefit and has a very good cost/efficiency rate compared to the surgical treatment.Key Words: hemophilia, chronic hemophilic arthropathy, flexum contracture of the knee, orthopaedic – nonsurgical treatment
Received for publication: Nov. 30, 2009. Revised: Jul. 30, 2010.
1 Clinic of Pediatric Surgery and Orthopaedics, 2 IIIrd Pediatric Clinic, Louis Turcanu Emergency Children’s Hospital, Timisoara
Correspondence to:Dr. Narcis F. Tepeneu, Clinic of Pediatric Surgery and Orthopaedics, Louis Turcanu Emergency Children’s Hospital, Timisoara, Tel. +40-256-203373.Email: [email protected]
INTRODUCTION
Joint contractures in patients with haemophilia are the result of recurrent intra-articular and intramuscular bleeding episodes. Approximately 50% of people with severe haemophilia (factor VIII or IX level <1 IU/dL) have articular contractures >10º, which can be disabling, causing decreased mobility and functional impairment.
Fernández-Palazzi and Batistella reported having found a knee contracture in every patient they assessed in hemophilia centers.1 Atkins et al reported a
216 TMJ 2010, Vol. 60, No. 2 - 3
prevalence of joint contractures in severe hemophiliacs between 50 and 95 %.2
This condition changes the gait pattern and sports ability of patients with severe hemophilia, adversely affecting their psychological wellbeing, social life, and work performance, and impairing their quality of life. The deformity pro duces an obvious shortening of the limb, requiring the patient to use external support devices, which induce both articular bleeding and impairment of the elbows and shoulders.2,3 Thus, besides restricting ambulation, lower limb flex ion contractures may contribute to upper limb skeletal impairment; consequently, correcting them is essential.
Flexion deformity of the knee is associated with both soft-tissue and bony changes.4
Although soft-tissue involvement is global, the fixed contractures that develop primarily involve contracture of the structures posterior to the axis of knee rotation. The posterior capsule is particularly contracted and adherent to the posterior femur and tibia. The posterior cruciate ligament can be contracted, together with the hamstring tendons, especially the semimembranosus. Proliferative posterior osteophytes can contribute to the flexion contracture because of the tethering effect.5
To constitute a true fixed flexion contracture, the deformity must persist despite local or systemic analgesia to alleviate the pain. Persistent flexion contractures cause a significant ambulatory deficit, with patients unable to obtain full extension and to achieve adequate relaxation of the quadriceps mechanism.
There are several treatment options, which include physical therapy, orthotic therapy and corrective devices, and surgical procedures.6 Some key parameters that should be considered when choosing the best therapeutic option include: the patient’s age, contracture severity, the presence of surrounding contractures, duration of the condition, muscular development, gait pattern, the presence of an articular subluxation, radiological findings, willingness of the patient to cooperate, and availability of health care.7,8
Several conservative methods have been developed for treating knee flexion contractures in patients with hemophilia. Regardless of the method chosen, factor replacement should be instituted during any orthopaedic treatment.
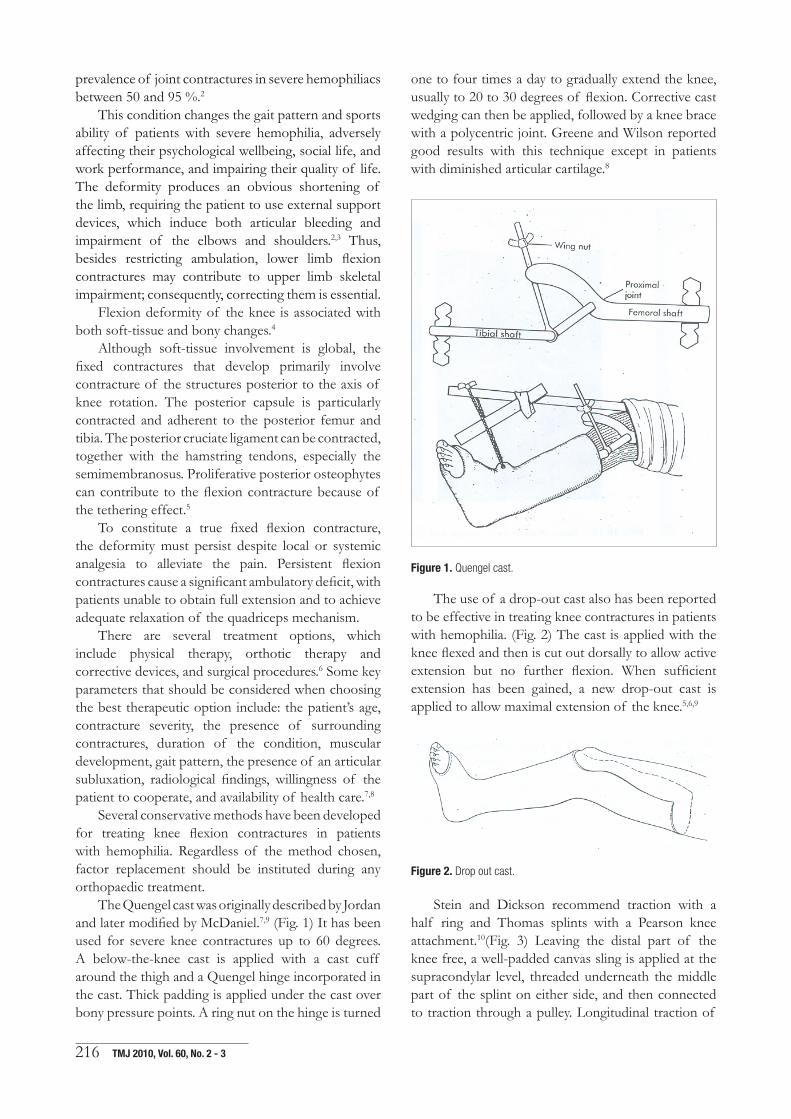
The Quengel cast was originally described by Jordan and later modified by McDaniel.7,9 (Fig. 1) It has been used for severe knee contractures up to 60 degrees. A below-the-knee cast is applied with a cast cuff around the thigh and a Quengel hinge incorporated in the cast. Thick padding is applied under the cast over bony pressure points. A ring nut on the hinge is turned
one to four times a day to gradually extend the knee, usually to 20 to 30 degrees of flexion. Corrective cast wedging can then be applied, followed by a knee brace with a polycentric joint. Greene and Wilson reported good results with this technique except in patients with diminished articular cartilage.8
Figure 1. Quengel cast.
The use of a drop-out cast also has been reported to be effective in treating knee contractures in patients with hemophilia. (Fig. 2) The cast is applied with the knee flexed and then is cut out dorsally to allow active extension but no further flexion. When sufficient extension has been gained, a new drop-out cast is applied to allow maximal extension of the knee.5,6,9
Figure 2. Drop out cast.
Stein and Dickson recommend traction with a half ring and Thomas splints with a Pearson knee attachment.10(Fig. 3) Leaving the distal part of the knee free, a well-padded canvas sling is applied at the supracondylar level, threaded underneath the middle part of the splint on either side, and then connected to traction through a pulley. Longitudinal traction of
Narcis F. Tepeneu et al 217
2-3 kilos is applied. Stein and Dickson reported better and more rapid response with this method than with cast wedging.
Figure 3. Reversed dynamic sling for knee flexion contracture.
Nelson et al described the use of a flowtron garment air-bag (Flowtron Machine, Huntleigh Medical, Luton, England) with intermittent compression for knee flexion contractures.11
Figure 4. 90/90 degree traction for knee contracture.
Bianco and Peterson12 use 90/90-degree traction for knee flexion contractures in patients with juvenile
rheumatoid arthritis, and this can be applied to some patients with hemophilia. (Fig. 4) Under adequate factor control, a skeletal pin is inserted in the proximal tibia, carefully avoiding the tibial tubercle. Traction is begun at 90 degrees of hip flexion and 90 degrees of knee flexion and, as the tibia is brought anteriorly and the subluxation reduced, the hip and knee gradually are extended until the contracture is corrected. During traction treatment the hip and knees are exercised daily to preserve the existing range of motion.
MATERIAL AND METHODS
Eleven patients with chronic hemophilic arthropathy were treated in the Pediatric Surgery and Orthopaedics Clinic of the Pediatric Emergency Hospital ‘’Louis Turcanu’’ Timisoara during a period of nine years (2000- 2009).
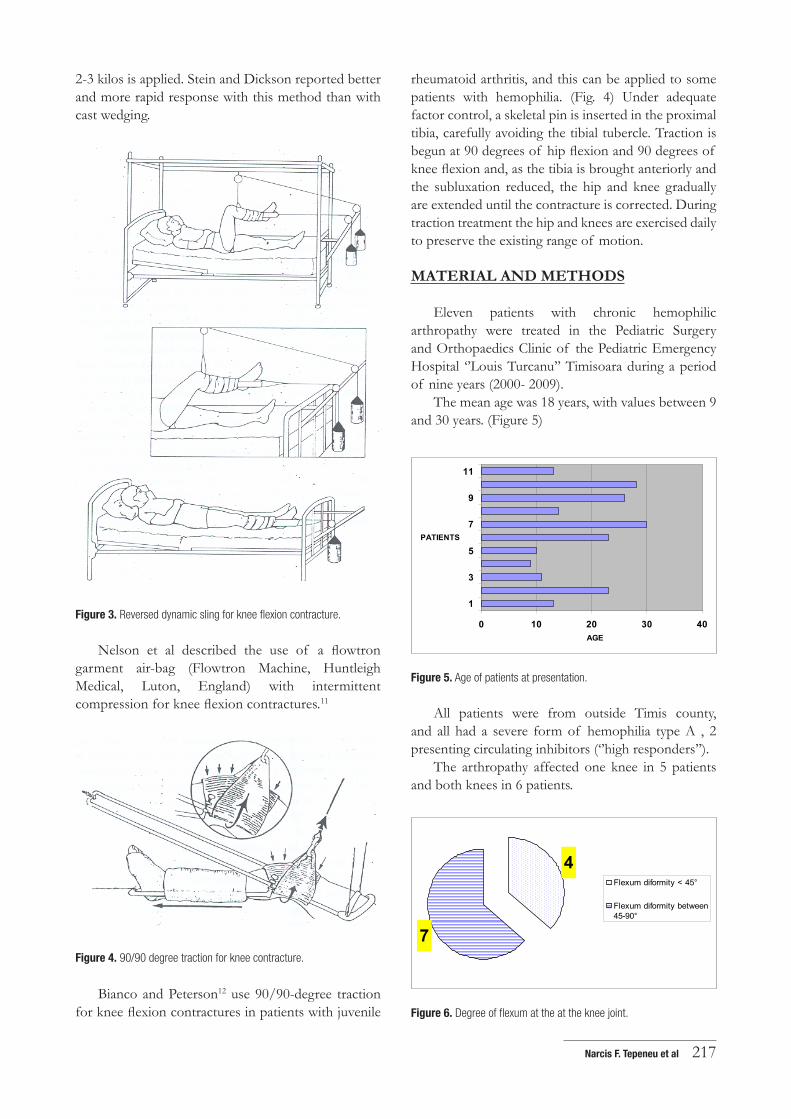
The mean age was 18 years, with values between 9 and 30 years. (Figure 5)
0 10 20 30 40
1
3
5
7
9
11
PATIENTS
AGE
Figure 5. Age of patients at presentation.
All patients were from outside Timis county, and all had a severe form of hemophilia type A , 2 presenting circulating inhibitors (‘’high responders’’).
The arthropathy affected one knee in 5 patients and both knees in 6 patients.
4
7
Flexum diformity < 45°
Flexum diformity between45-90°
Figure 6. Degree of flexum at the at the knee joint.
218 TMJ 2010, Vol. 60, No. 2 - 3
The degree of flexum was between 30 si 90°. We split the lot in 2 groups: patients with flexum deformity below 45 °(4 patients) and those with flexum deformity over 45° (7 patients). (Fig. 6)
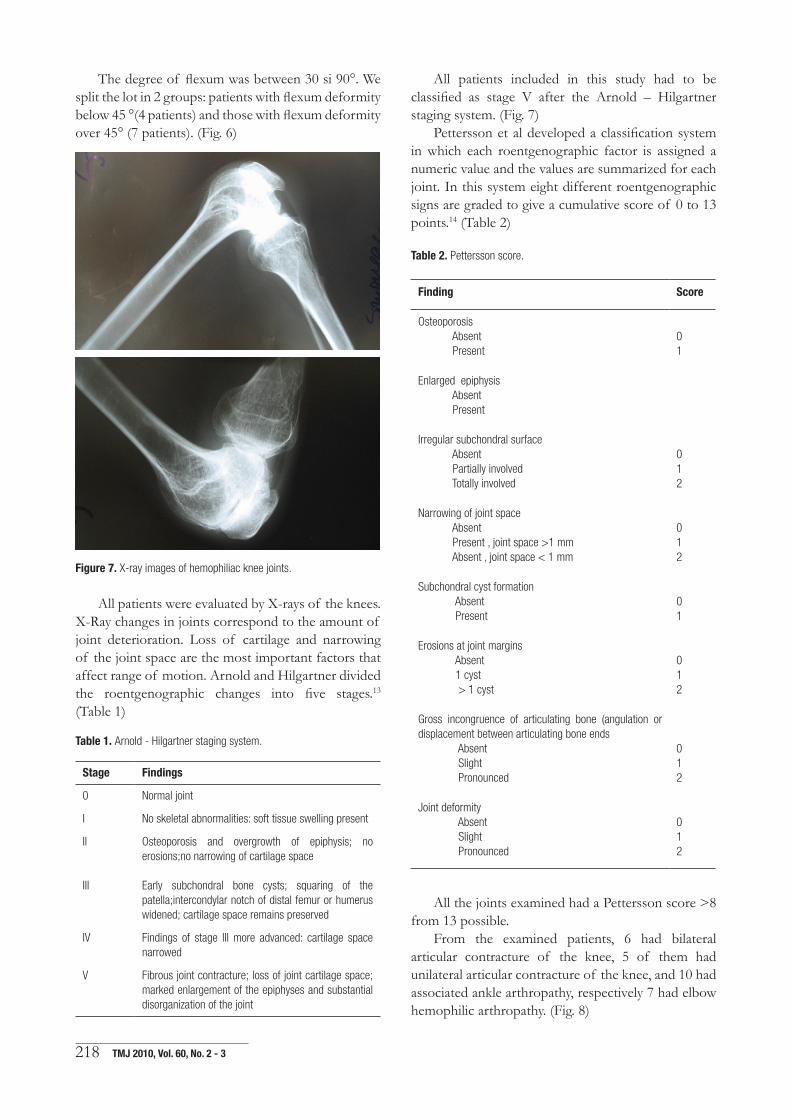
Figure 7. X-ray images of hemophiliac knee joints.
All patients were evaluated by X-rays of the knees. X-Ray changes in joints correspond to the amount of joint deterioration. Loss of cartilage and narrowing of the joint space are the most important factors that affect range of motion. Arnold and Hilgartner divided the roentgenographic changes into five stages.13 (Table 1)
Table 1. Arnold - Hilgartner staging system.
Stage Findings
0 Normal joint
I No skeletal abnormalities: soft tissue swelling present
II Osteoporosis and overgrowth of epiphysis; no erosions;no narrowing of cartilage space
III Early subchondral bone cysts; squaring of the patella;intercondylar notch of distal femur or humerus widened; cartilage space remains preserved
IV Findings of stage III more advanced: cartilage space narrowed
V Fibrous joint contracture; loss of joint cartilage space; marked enlargement of the epiphyses and substantial disorganization of the joint
All patients included in this study had to be classified as stage V after the Arnold – Hilgartner staging system. (Fig. 7)
Pettersson et al developed a classification system in which each roentgenographic factor is assigned a numeric value and the values are summarized for each joint. In this system eight different roentgenographic signs are graded to give a cumulative score of 0 to 13 points.14 (Table 2)
Table 2. Pettersson score.
Finding Score
Osteoporosis Absent Present
01
Enlarged epiphysis Absent Present
Irregular subchondral surface Absent Partially involved Totally involved
012
Narrowing of joint space Absent Present , joint space >1 mm Absent , joint space < 1 mm
012
Subchondral cyst formation Absent Present
01
Erosions at joint margins Absent 1 cyst > 1 cyst
012
Gross incongruence of articulating bone (angulation or displacement between articulating bone ends Absent Slight Pronounced
012
Joint deformity Absent Slight Pronounced
012
All the joints examined had a Pettersson score >8 from 13 possible.
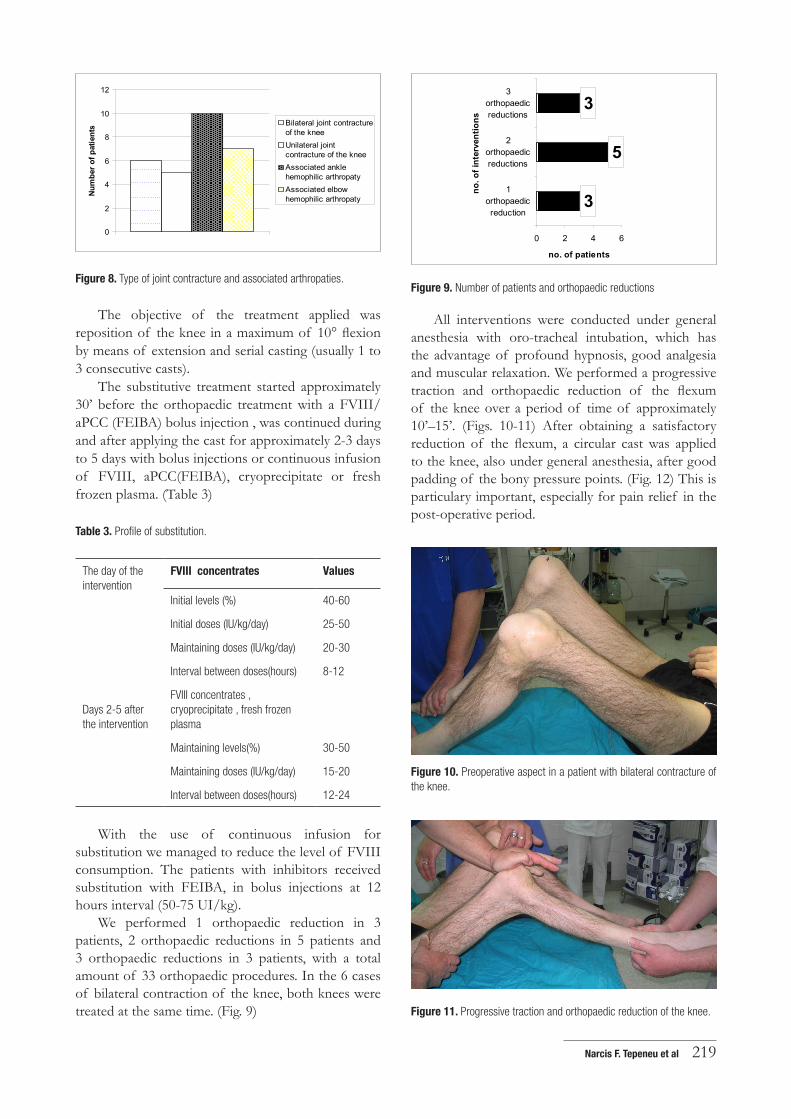
From the examined patients, 6 had bilateral articular contracture of the knee, 5 of them had unilateral articular contracture of the knee, and 10 had associated ankle arthropathy, respectively 7 had elbow hemophilic arthropathy. (Fig. 8)
Narcis F. Tepeneu et al 219
0
2
4
6
8
10
12Nu
mbe
r of p
atie
nts Bilateral joint contracture
of the kneeUnilateral jointcontracture of the kneeAssociated anklehemophilic arthropaty Associated elbowhemophilic arthropaty
Figure 8. Type of joint contracture and associated arthropaties.
The objective of the treatment applied was reposition of the knee in a maximum of 10° flexion by means of extension and serial casting (usually 1 to 3 consecutive casts).
The substitutive treatment started approximately 30’ before the orthopaedic treatment with a FVIII/aPCC (FEIBA) bolus injection , was continued during and after applying the cast for approximately 2-3 days to 5 days with bolus injections or continuous infusion of FVIII, aPCC(FEIBA), cryoprecipitate or fresh frozen plasma. (Table 3)
Table 3. Profile of substitution.
The day of the intervention
FVIII concentrates Values
Initial levels (%) 40-60
Initial doses (IU/kg/day) 25-50
Maintaining doses (IU/kg/day) 20-30
Interval between doses(hours) 8-12
Days 2-5 after the intervention
FVIII concentrates , cryoprecipitate , fresh frozen plasma
Maintaining levels(%) 30-50
Maintaining doses (IU/kg/day) 15-20
Interval between doses(hours) 12-24
With the use of continuous infusion for substitution we managed to reduce the level of FVIII consumption. The patients with inhibitors received substitution with FEIBA, in bolus injections at 12 hours interval (50-75 UI/kg).
We performed 1 orthopaedic reduction in 3 patients, 2 orthopaedic reductions in 5 patients and 3 orthopaedic reductions in 3 patients, with a total amount of 33 orthopaedic procedures. In the 6 cases of bilateral contraction of the knee, both knees were treated at the same time. (Fig. 9)
3
5
3
0 2 4 6
1orthopaedicreduction
2orthopaedicreductions
3orthopaedicreductions
no. o
f int
erve
ntio
ns
no. of patients
Figure 9. Number of patients and orthopaedic reductions
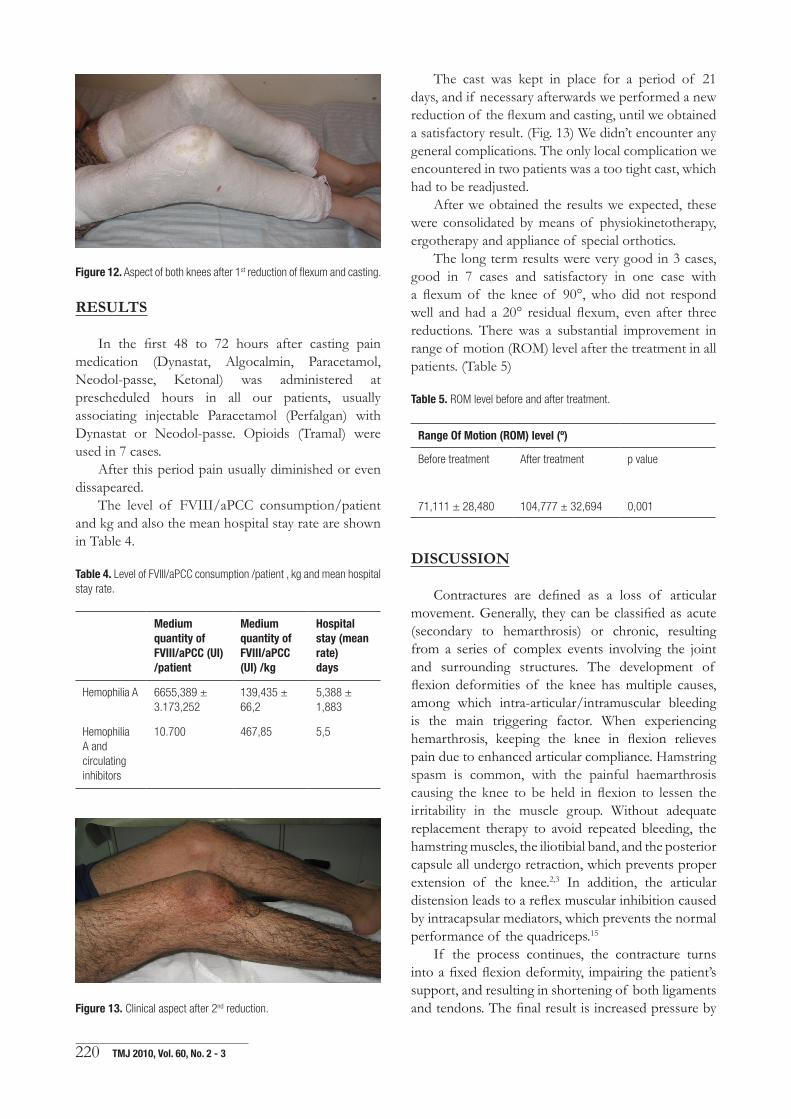
All interventions were conducted under general anesthesia with oro-tracheal intubation, which has the advantage of profound hypnosis, good analgesia and muscular relaxation. We performed a progressive traction and orthopaedic reduction of the flexum of the knee over a period of time of approximately 10’–15’. (Figs. 10-11) After obtaining a satisfactory reduction of the flexum, a circular cast was applied to the knee, also under general anesthesia, after good padding of the bony pressure points. (Fig. 12) This is particulary important, especially for pain relief in the post-operative period.
Figure 10. Preoperative aspect in a patient with bilateral contracture of the knee.
Figure 11. Progressive traction and orthopaedic reduction of the knee.
220 TMJ 2010, Vol. 60, No. 2 - 3
Figure 12. Aspect of both knees after 1st reduction of flexum and casting.
RESULTS
In the first 48 to 72 hours after casting pain medication (Dynastat, Algocalmin, Paracetamol, Neodol-passe, Ketonal) was administered at prescheduled hours in all our patients, usually associating injectable Paracetamol (Perfalgan) with Dynastat or Neodol-passe. Opioids (Tramal) were used in 7 cases.
After this period pain usually diminished or even dissapeared.
The level of FVIII/aPCC consumption/patient and kg and also the mean hospital stay rate are shown in Table 4.
Table 4. Level of FVIII/aPCC consumption /patient , kg and mean hospital stay rate.
Medium quantity of FVIII/aPCC (UI) /patient
Medium quantity of FVIII/aPCC (UI) /kg
Hospital stay (mean rate)days
Hemophilia A 6655,389 ± 3.173,252
139,435 ± 66,2
5,388 ± 1,883
Hemophilia A and circulating inhibitors
10.700 467,85 5,5
Figure 13. Clinical aspect after 2nd reduction.
The cast was kept in place for a period of 21 days, and if necessary afterwards we performed a new reduction of the flexum and casting, until we obtained a satisfactory result. (Fig. 13) We didn’t encounter any general complications. The only local complication we encountered in two patients was a too tight cast, which had to be readjusted.
After we obtained the results we expected, these were consolidated by means of physiokinetotherapy, ergotherapy and appliance of special orthotics.
The long term results were very good in 3 cases, good in 7 cases and satisfactory in one case with a flexum of the knee of 90°, who did not respond well and had a 20° residual flexum, even after three reductions. There was a substantial improvement in range of motion (ROM) level after the treatment in all patients. (Table 5)
Table 5. ROM level before and after treatment.
Range Of Motion (ROM) level (º)
Before treatment After treatment p value
71,111 ± 28,480 104,777 ± 32,694 0,001
DISCUSSION
Contractures are defined as a loss of articular movement. Generally, they can be classified as acute (secondary to hemarthrosis) or chronic, resulting from a series of complex events involving the joint and surrounding structures. The development of flexion deformities of the knee has multiple causes, among which intra-articular/intramuscular bleeding is the main triggering factor. When experiencing hemarthrosis, keeping the knee in flexion relieves pain due to enhanced articular compliance. Hamstring spasm is common, with the painful haemarthrosis causing the knee to be held in flexion to lessen the irritability in the muscle group. Without adequate replacement therapy to avoid repeated bleeding, the hamstring muscles, the iliotibial band, and the posterior capsule all undergo retraction, which prevents proper extension of the knee.2,3 In addition, the articular distension leads to a reflex muscular inhibition caused by intracapsular mediators, which prevents the normal performance of the quadriceps.15
If the process continues, the contracture turns into a fixed flexion deformity, impairing the patient’s support, and resulting in shortening of both ligaments and tendons. The final result is increased pressure by

Narcis F. Tepeneu et al 221
unit of area in the posterior condyles over the tibial plateau, subluxating the tibia towards the back, and impairing the cartilage irreversibly. These deforming forces can also produce a valgus deformity. A hip flexion contracture and/or an equinus foot deformity will also contribute to flexion deformity at the knee.
This initiates an arthritic process with reduced articular spaces, osteophytes, and the deformities that are typical of hemophilic joint disease.16
In a paper published in 1999 Fernandez-Palazzi and Battistella have used serial casting and wedging in 58 patients and extension/desubluxation orthoses in 13 patients.1 On average it was possible to achieve –5° of extension by 4 weeks, with only a little improvement in the following 4 weeks. The short- to medium- term results using either extension/desubluxation hinges or serial casting were similar. Both methods have been shown to result in significant improvement in joint contracture. These non-invasive methods are generally successful in mild contractures, and are used as adjuncts after radical soft-tissue release, in order to stretch the tight neurovascular structures gradually.
It is considered that the amount of corrective force that may be applied with casts, splints and braces is limited by the inability of the skin to tolerate direct pressure.5,17,18
However, using the method we described above, we encountered none of these complications, with good functional results and improvement of range of motion in all patients. Great care must be taken, because all these conservative treatment methods can cause articular subluxation. Taking care and applying progressive traction and reduction of the knee over a period of 10 to 15 minutes under general anesthesia proved to be a safe method. We didn’t encounter any articular subluxation.
Experimental evidence suggests that low-load prolonged stretch is preferred to high-load brief intermittent stretch in the elongation of collagen.5,18
Problems encountered include a rebound phenomenon after cast removal, with loss of the temporarily increased total arc of motion .However this can be overcome with the use of proper orthotics and physiokinetotherapy..18,19
There are still two unanswered questions: Why does the muscle stretch? How can the rebound phenomenon be minimized?
A combination of continued clinical and basic research will, it is hoped, provide answers to these questions.
There are also minimal requirements which have to be taken into consideration for a safe and efficient attempt of treatment:
1. Access to adequate replacement therapy, under quantitative and qualitative aspects, for all kind of clinical forms of the disease;
2. Continuous monitoring of the coagulation factors level, of the recovery time and of the inhibitors level during pre-, intra- and post-interventional follow-up;
3. Access to adequate anesthesia;4. An experienced and engaged team of doctors,
nurses and haemostasis laboratory assistants, based on a good cooperation.
CONCLUSIONS
Treatment of knee contractures in patients with haemophilia should be primarily by physiotherapy, splintage, casts and corrective devices.18
The orthopaedic non-surgical treatment by means of the method described in this paper proved to be a good alternative to other conservative methods of treatment and especially to surgical correction.
The treatment proved to be well tolerated and without major complications. Also it brings a great functional gain to the patients affected by knee contracture, with regaining of ambulation and increase of range of motion of affected joints and quality of life of the patient.
It is also very cost efficient compared to the surgical treatment , especially by means of reducing factor VIII /aPCC consumption, a highly important fact in a country like Romania where we frequently experience insufficient replacement therapy, both for the quantity and the duration of treatment;
REFERENCES
1. Fernández-Palazzi F, Battistella LR. Non-operative treatment of flexion contracture of the knee in haemophilia. Haemophilia, 1999;5(1):20–24.
2. Atkins RM, Henderson NJ, Duthie RB. Joint contractures in the hemophiliacs. Clin Orthop 1987; 219: 97-106.
3. Sohail MT, Akhtar ZM, Management of joint and soft tissue contractures in haemophilic patients. Sohail MT, Heijnen L (eds). In: Comprehensive hemophilia care in developing countries. Karachi, Pakistan, 2001;20:166–77.
4. Rodríguez-Merchán EC Correction of fixed contractures during total knee arthroplasty in haemophiliacs. Haemophilia, 1999;5(1):33–38.
5. Rodriguez-Merchan E. C, Goddard N. J. , Lee , C. A. , Musculoskeletal Aspects of Hemophilia, Blackwell Science; 2000.
6. Caviglia H. A. , Solimeno , L.P. , Orthopaedic Surgery in patients with haemophilia , Springer-Verlag Italia; 2008.
7. McDaniel WJ. A modified subluxation hinge for use in hemophilic knee flexion contractures. Clin Orthop 1974; 103:50.
8. Llinás A, Heijnen L, Treatment Considerations in Patients with Multiple Deformities: Rehabilitation and Orthopaedic Surgery. In: Sohail MT, Heynen L (eds). Comprehensive hemophilia care in developing countries. Karachi, Pakistan; 2001, p. 123-34.

222 TMJ 2010, Vol. 60, No. 2 - 3
9. Rodríguez-Merchán EC. Therapeutic options in the management of articular contractures in haemophiliacs. Haemophilia , 1999; 5(1):5–9
10. Stein H. , Dickinson R.A. , Reversed dynamic sling for knee flexion contracture , J. Bone Surg. 1975;57A:282-8.
11. Nelson I.W, Atkins R.M, Allen A.L. The management of knee flexion contractures in haemophilia: brief report. J Bone Joint Surg Br, 1989;71-B: 327-8.
12. Bianco AJ Jr., Peterson H.A. 90/90-degree traction for a knee contracture with subluxation, Orthop. Clin. North Am 1971;2:745,1971.
13. Arnold WD, Hilgartner MW. Hemophilic arthropathy. J Bone Joint Surg (Am) , 1977;59:287–305.
14. Pettersson H., Ahlberg A. , Nilsson I. M., A radiologic classification of
haemophilic arthropathy, Clin Orthop. 1980;153-59 .15. Spencer JD, Hayes KC, Alexander IJ Knee joint effusion and quadriceps
reflex inhi bition in man. Arch Phys Med Rehab, 1984;65:171–7.16. Heim M, Horoszowski H, Varon D et al. The fixed flexed and subluxed
knee in the haemophilic child: what should be done? Haemophilia 1996;2:47–50.
17. Rodriguez-Merchan E. C., Proximal tibial valgus osteotomy for hemophilic arthropathy of the knee, Orthop Rev 1992;21:204–8.
18. Rodriguez-Merchan. The Haemophilic Joint – New perspectives, Blackwell Science, 2003.
19. Heijnen L, De Kleijn P. Physiotherapy for the treatmentof articular contractures in haemophilia. Haemophilia 1999;5 (Suppl. 1):16–99.