Microzonuloscopy
7
RETROLENTAL FIBROPLASIA 345 3. Kinsey, V. E.: Retrolental fibroplasia: Co-operative study of retrolental fibroplasia and the use of oxygen. AMA Arch. Ophth., 56:481-543 (Oct.) 1956. 4. Zacharias, L.: Retrolental fibroplasia. Am. J. Ophth., 49:382-384 (Feb.) 1960. 5. Zacharias, L., Reynolds, W. E., Chisholm, J. F. Jr., and King, M. J.: The incidence and severity of retrolental fibroplasia in relation to possible causative factors. Am. J. Ophth., 38:317-336 (Sept.) 1954. MICROZONULOSCOPY BlOMICROSCOPIC EXAMINATION OF THE ZONULES WITHOUT A CONTACT LENS EMANUEL ROSEN, M.D. Newark, New Jersey Improvement in biomicroscopic techniques, associated with facility of manipulation and increased intensity of illumination, has cre- ated a more ready accessibility of certain zones heretofore rendered visible only through use of auxiliary prisms, mirrors and contact lenses. Nevertheless, there are still many unexplored areas accessible by way of older methods free of these mechanisms. To elucidate this point, it is known that the lens equator and suspensory ligament can ordinarily be observed only through an iris coloboma, in aniridia and in subluxated lens. 1 On the other hand, Busacca 2 demon- strated a normal perceptibility for Petit's space, the edge of the lens and the posterior zonular fibers. This could be seen only in a patient with widely dilated pupils, in whom the lens was small, and only when the patient looked sharply downward. It obviously fol- lowed, after employing this angulation, that further advantage could be attained by modi- fying the equipment ordinarily employed in biomicroscopy, in such manner that greater rotations of the head could be obtained. At the expense of belaboring this point a bit, there certainly appears to be no physio- logic reason why, in the biomicroscopic ap- proach, one should fail to take advantage of gazing into at least 120 degrees of unex- plored periphery of the eye just because the instrument limits the field of view of the eye to a small sector of a circumference by forcing one to view the eye in a vertical plane, as shown in Figure 1. The advantages to be gained in the "up-and-down field" may be appreciated from the illustrations; while the advantages of a chinrest rotating to right and left have been described in a previous communication. 3 In this paper only the "downward-gaze technique" will be dis- cussed, although the same advantages may be obtained for the upper fields by displac- ing the chin upward and tilting the head back 45 degrees or more. Having employed this modified technique for some time now, I have become increasingly aware of its many rewards (even in biomicroscopy of the in- ferior periphery with the plus 55 or plus 32 lens) and would like to make this relatively simple method available to others. The following study deals with a method of examining the anterior hyaloid membrane, Wieger's ligament, the posterior zonular fi- bers, the retrozonular space and, in well-di- lated pupils, the ciliary processes, all without any aid other than the biomicroscope and without employing any scierai pressure. The technique requires a few special pro- cedures which differ from the usual biomi- croscopy but which are in no sense more diffi- cult. For example, it is necessary to raise the patient's chair or stool eight to 10 inches higher than usual. The patient must assume a leaning over rather than an erect position. The chinrest is not employed. The upper part of the forehead must be pressed firmly against the headband (fig. 2). In this posi- tion the head is actually angled 45 to 60 de- grees toward the floor, thus permitting a view of an eye which is looking down 60 degrees or more. The upper eyelid must be raised
Transcript of Microzonuloscopy

RETROLENTAL FIBROPLASIA 345
3. Kinsey, V. E.: Retrolental fibroplasia: Co-operative study of retrolental fibroplasia and the use of oxygen. AMA Arch. Ophth., 56:481-543 (Oct.) 1956.
4. Zacharias, L.: Retrolental fibroplasia. Am. J. Ophth., 49:382-384 (Feb.) 1960. 5. Zacharias, L., Reynolds, W. E., Chisholm, J. F. Jr., and King, M. J.: The incidence and severity
of retrolental fibroplasia in relation to possible causative factors. Am. J. Ophth., 38:317-336 (Sept.) 1954.
MICROZONULOSCOPY
BlOMICROSCOPIC EXAMINATION OF THE ZONULES WITHOUT A CONTACT LENS
EMANUEL ROSEN, M.D. Newark, New Jersey
Improvement in biomicroscopic techniques, associated with facility of manipulation and increased intensity of illumination, has created a more ready accessibility of certain zones heretofore rendered visible only through use of auxiliary prisms, mirrors and contact lenses. Nevertheless, there are still many unexplored areas accessible by way of older methods free of these mechanisms.
To elucidate this point, it is known that the lens equator and suspensory ligament can ordinarily be observed only through an iris coloboma, in aniridia and in subluxated lens.1 On the other hand, Busacca2 demonstrated a normal perceptibility for Petit's space, the edge of the lens and the posterior zonular fibers. This could be seen only in a patient with widely dilated pupils, in whom the lens was small, and only when the patient looked sharply downward. It obviously followed, after employing this angulation, that further advantage could be attained by modifying the equipment ordinarily employed in biomicroscopy, in such manner that greater rotations of the head could be obtained.
At the expense of belaboring this point a bit, there certainly appears to be no physiologic reason why, in the biomicroscopic approach, one should fail to take advantage of gazing into at least 120 degrees of unexplored periphery of the eye just because the instrument limits the field of view of the eye to a small sector of a circumference by forcing one to view the eye in a vertical plane, as shown in Figure 1. The advantages to be gained in the "up-and-down field" may
be appreciated from the illustrations; while the advantages of a chinrest rotating to right and left have been described in a previous communication.3 In this paper only the "downward-gaze technique" will be discussed, although the same advantages may be obtained for the upper fields by displacing the chin upward and tilting the head back 45 degrees or more. Having employed this modified technique for some time now, I have become increasingly aware of its many rewards (even in biomicroscopy of the inferior periphery with the plus 55 or plus 32 lens) and would like to make this relatively simple method available to others.
The following study deals with a method of examining the anterior hyaloid membrane, Wieger's ligament, the posterior zonular fibers, the retrozonular space and, in well-dilated pupils, the ciliary processes, all without any aid other than the biomicroscope and without employing any scierai pressure.
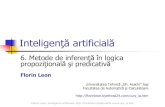
The technique requires a few special procedures which differ from the usual biomicroscopy but which are in no sense more difficult. For example, it is necessary to raise the patient's chair or stool eight to 10 inches higher than usual. The patient must assume a leaning over rather than an erect position. The chinrest is not employed. The upper part of the forehead must be pressed firmly against the headband (fig. 2) . In this position the head is actually angled 45 to 60 degrees toward the floor, thus permitting a view of an eye which is looking down 60 degrees or more. The upper eyelid must be raised
346 EMANUEL ROSEN
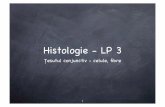
Fig. 1 (Rosen). Area of light cut when eye looks down 60 degrees included within the lines A-B, C-D. This illustrates the area which is accessible to mi-crozonuloscopy in the eyes-down position. (Modified after a drawing by Busacca.)
and the head of the patient should be so adjusted that the beam of light clears the obstruction produced by the eyebrow.
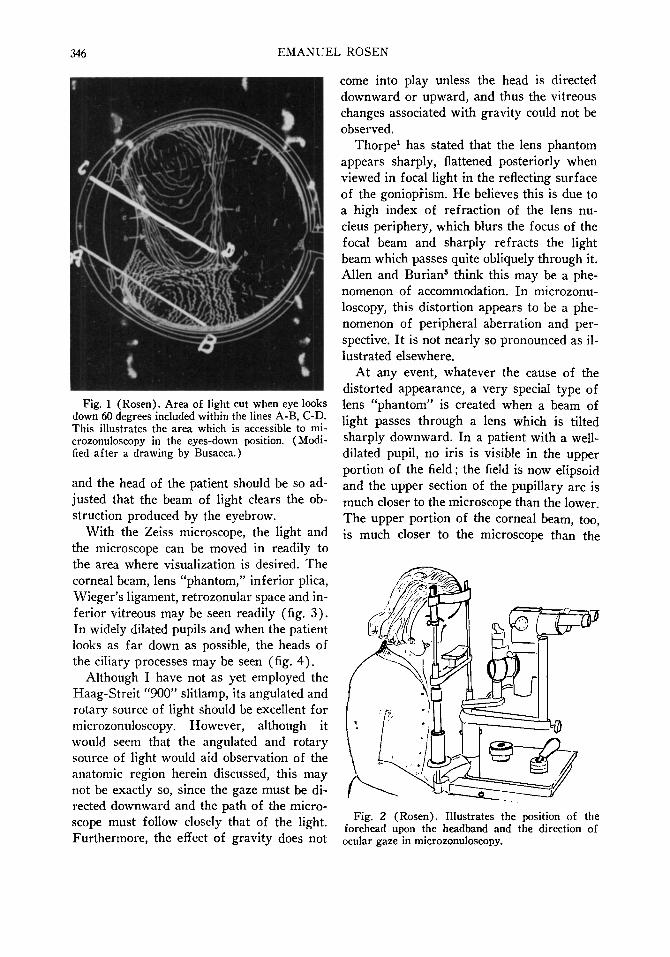
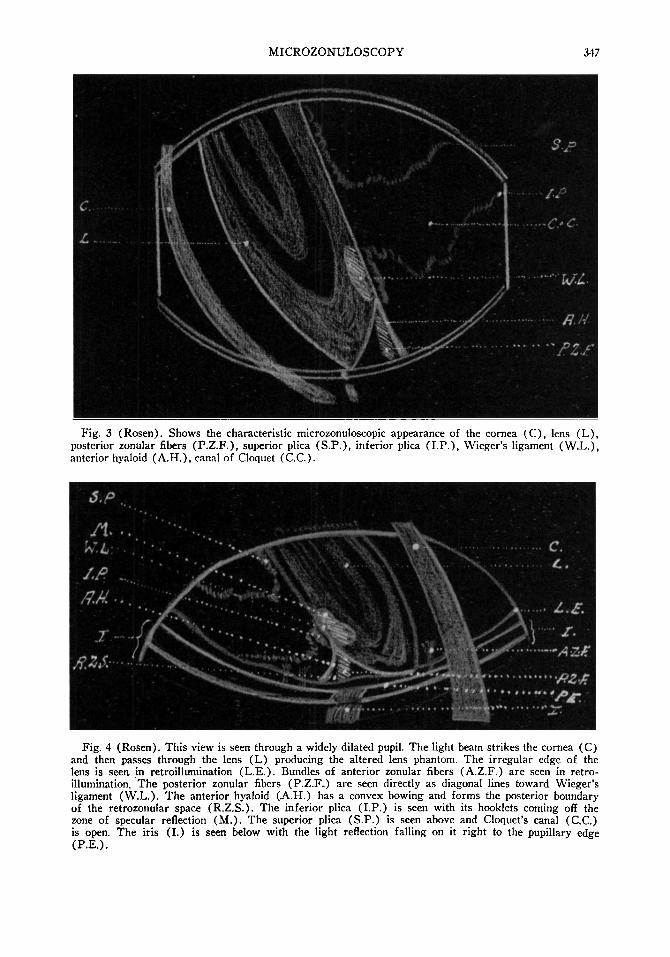
With the Zeiss microscope, the light and the microscope can be moved in readily to the area where visualization is desired. The corneal beam, lens "phantom," inferior plica, Wieger's ligament, retrozonular space and inferior vitreous may be seen readily (fig. 3). In widely dilated pupils and when the patient looks as far down as possible, the heads of the ciliary processes may be seen (fig. 4) .
Although I have not as yet employed the Haag-Streit "900" slitlamp, its angulated and rotary source of light should be excellent for microzonuloscopy. However, although it would seem that the angulated and rotary source of light would aid observation of the anatomic region herein discussed, this may not be exactly so, since the gaze must be directed downward and the path of the microscope must follow closely that of the light. Furthermore, the effect of gravity does not
come into play unless the head is directed downward or upward, and thus the vitreous changes associated with gravity could not be observed.
Thorpe1 has stated that the lens phantom appears sharply, flattened posteriorly when viewed in focal light in the reflecting surface of the gonioprism. He believes this is due to a high index of refraction of the lens nucleus periphery, which blurs the focus of the focal beam and sharply refracts the light beam which passes quite obliquely through it. Allen and Burian5 think this may be a phenomenon of accommodation. In microzonuloscopy, this distortion appears to be a phenomenon of peripheral aberration and perspective. It is not nearly so pronounced as illustrated elsewhere.
At any event, whatever the cause of the distorted appearance, a very special type of lens "phantom" is created when a beam of light passes through a lens which is tilted sharply downward. In a patient with a well-dilated pupil, no iris is visible in the upper portion of the field ; the field is now elipsoid and the upper section of the pupillary arc is much closer to the microscope than the lower. The upper portion of the corneal beam, too, is much closer to the microscope than the
Fig. 2 (Rosen). Illustrates the position of the forehead upon the headband and the direction of ocular gaze in microzonuloscopy.
MICROZONULOSCOPY 347
Fig. 3 (Rosen). Shows the characteristic microzonuloscopic appearance of the cornea (C), lens (L), posterior zonular fibers (P.Z.F.), superior plica (S.P.), inferior plica (I.P.), Wieger's ligament (W.L.), anterior hyaloid (A.H.), canal of Cloquet (C.C.).
Fig. 4 (Rosen). This view is seen through a widely dilated pupil. The light beam strikes the cornea (C) and then passes through the lens (L) producing the altered lens phantom. The irregular edge of the lens is seen in retroillumination (L.E.). Bundles of anterior zonular fibers (A.Z.F.) are seen in retro-illumination. The posterior zonular fibers (P.Z.F..) are seen directly as diagonal lines toward Wieger's ligament (W.L.). The anterior hyaloid (A.H.) has a convex bowing and forms the posterior boundary of the retrozonular space (R.Z.S.). The inferior plica (I.P.) is seen with its hooklets coming off the zone of specular reflection (M.). The superior plica (S.P.) is seen above and Cloquet's canal (C.C.) is open. The iris (I.) is seen below with the light reflection falling on it right to the pupillary edge (P.E.).
348 EMANUEL ROSEN
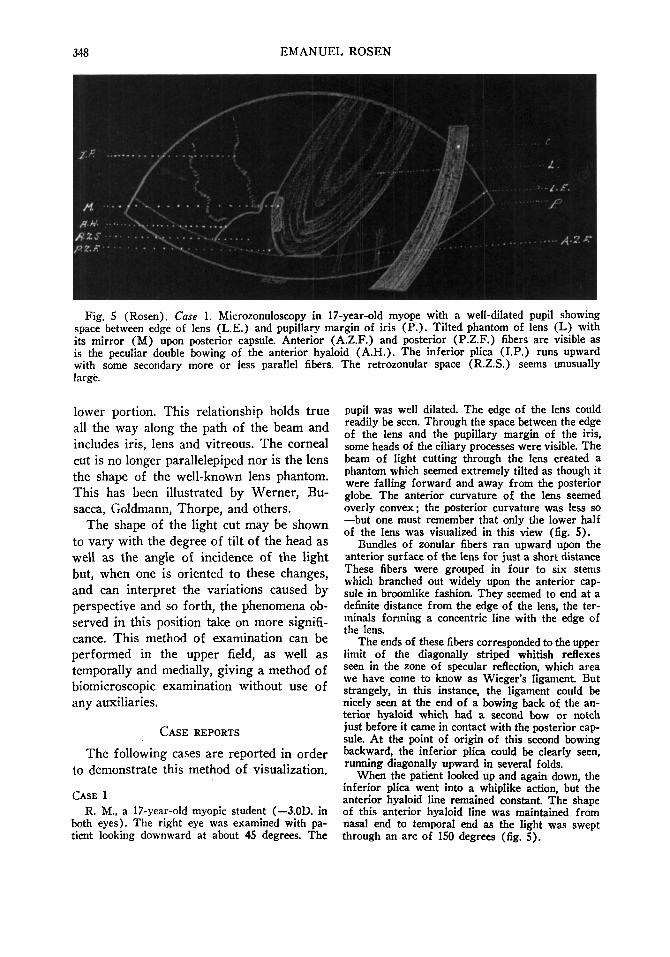
Fig. S (Rosen). Case 1. Microzonuloscopy in 17-year-old myope with a well-dilated pupil showing space between edge of lens (L.E.) and pupillary margin of iris (P.) . Tilted phantom of lens (L) with its mirror (M) upon posterior capsule. Anterior (A.Z.F.) and posterior (P.Z.F.) fibers are visible as is the peculiar double bowing of the anterior hyaloid (A.H.). The inferior plica (I.P.) runs upward with some secondary more or less parallel fibers. The retrozonular space (R.Z.S.) seems unusually large.
lower portion. This relationship holds true all the way along the path of the beam and includes iris, lens and vitreous. The corneal cut is no longer parallelepiped nor is the lens the shape of the well-known lens phantom. This has been illustrated by Werner , Bu-sacca, Goldmann, Thorpe, and others.
The shape of the light cut may be shown to vary with the degree of tilt of the head as well as the angle of incidence of the light but, when one is oriented to these changes, and can interpret the variations caused by perspective and so forth, the phenomena observed in this position take on more significance. This method of examination can be performed in the upper field, as well as temporally and medially, giving a method of biomicroscopic examination without use of any auxiliaries.
CASE REPORTS
The following cases are reported in order to demonstrate this method of visualization.
CASE 1 R. M., a 17-year-old myopic student (—3.0D. in
both eyes). The right eye was examined with patient looking downward at about 45 degrees. The
pupil was well dilated. The edge of the lens could readily be seen. Through the space between the edge of the lens and the pupillary margin of the iris, some heads of the ciliary processes were visible. The beam of light cutting through the lens created a phantom which seemed extremely tilted as though it were falling forward and away from the posterior globe. The anterior curvature of the lens seemed overly convex; the posterior curvature was less so —but one must remember that only the lower half of the lens was visualized in this view (fig. 5).
Bundles of zonular fibers ran upward upon the anterior surface of the lens for just a short distance These fibers were grouped in four to six stems which branched out widely upon the anterior capsule in broomlike fashion. They seemed to end at a definite distance from the edge of the lens, the terminals forming a concentric line with the edge of the lens.
The ends of these fibers corresponded to the upper limit of the diagonally striped whitish reflexes seen in the zone of specular reflection, which area we have come to know as Wieger's ligament. But strangely, in this instance, the ligament could be nicely seen at the end of a bowing back of the anterior hyaloid which had a second bow or notch just before it came in contact with the posterior capsule. At the point of origin of this second bowing backward, the inferior plica could be clearly seen, running diagonally upward in several folds.
When the patient looked up and again down, the inferior plica went into a whiplike action, but the anterior hyaloid line remained constant. The shape of this anterior hyaloid line was maintained from nasal end to temporal end as the light was swept through an arc of ISO degrees (fig. 5).
MICROZONULOSCOPY 349
Burian and Allen" have described this condition and, in all but two cases studied by them, the anterior hyaloid, running from Wieger's ligament, was convex anteriorly. In one exception, the convexity was posterior, as described in my Case 1, in which, under dilatation, the posterior bowing disappeared and the anterior hyaloid became a straight line with the posterior capsule. This was not true in Burian and Allen's case when under dilatation, which makes one question the conclusion drawn by these authors, namely, "Finally our observations upon the periphery of the vitreous surface strongly suggest that the vitreous body far from pressing upon the periphery of the lens was actually under reduced tension during accommodation." (These remarks are not intended as a criticism of the theory advanced by Burian and Allen5 but are intended to illustrate an important diagnostic biomicroscopic method—not difficult to perform and free of the complexities inherent in the gonioscopic method.)
CASE 2
This 43-year old patient presented with a characteristic nuclear cataract. The changes in the posterior cortex and in the posterior capsule consisted primarily of vacuoles. When the vitreous was examined in eyes straight ahead, this structure could be seen with difficulty but, when examined upon looking sharply downward, much more could be observed.
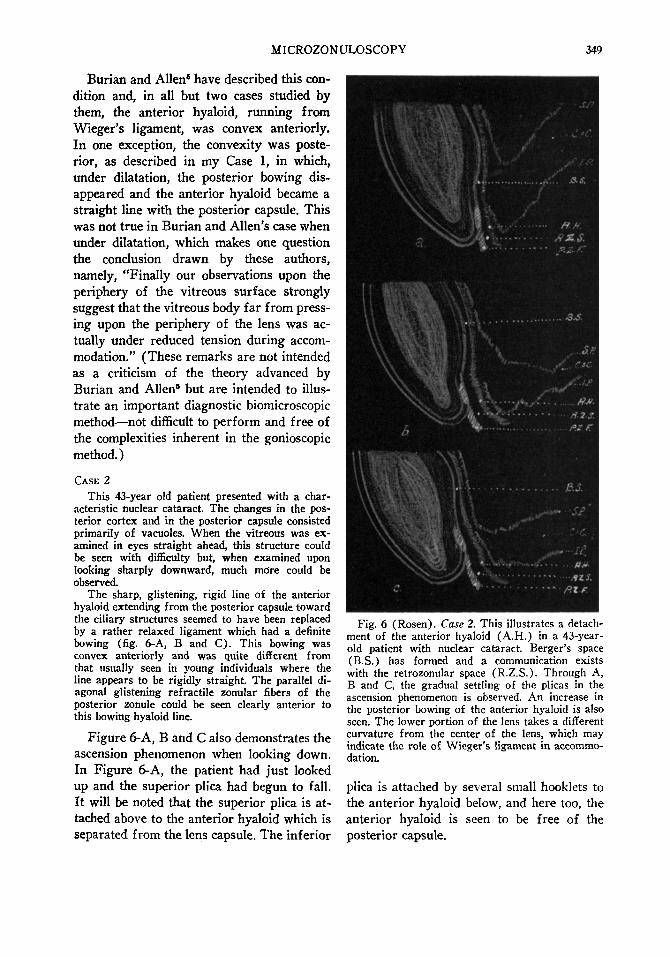
The sharp, glistening, rigid line of the anterior hyaloid extending from the posterior capsule toward the ciliary structures seemed to have been replaced by a rather relaxed ligament which had a definite bowing (fig. 6-A, B and C). This bowing was convex anteriorly and was quite different from that usually seen in young individuals where the line appears to be rigidly straight. The parallel diagonal glistening refractile zonular fibers of the posterior zonule could be seen clearly anterior to this bowing hyaloid line.
Figure 6-A, B and C also demonstrates the ascension phenomenon when looking down. In Figure 6-A, the patient had just looked up and the superior plica had begun to fall. It will be noted that the superior plica is attached above to the anterior hyaloid which is separated from the lens capsule. The inferior
Fig. 6 (Rosen). Case 2. This illustrates a detachment of the anterior hyaloid (A.H.) in a 43-year-old patient with nuclear cataract. Berger's space (B.S.) has formed and a communication exists with the retrozonular space (R.Z.S.). Through A, B and C, the gradual settling of the plicas in the ascension phenomenon is observed. An increase in the posterior bowing of the anterior hyaloid is also seen. The lower portion of the lens takes a different curvature from the center of the lens, which may indicate the role of Wieger's ligament in accommodation.
plica is attached by several small hooklets to the anterior hyaloid below, and here too, the anterior hyaloid is seen to be free of the posterior capsule.

350 EMANUEL ROSEN
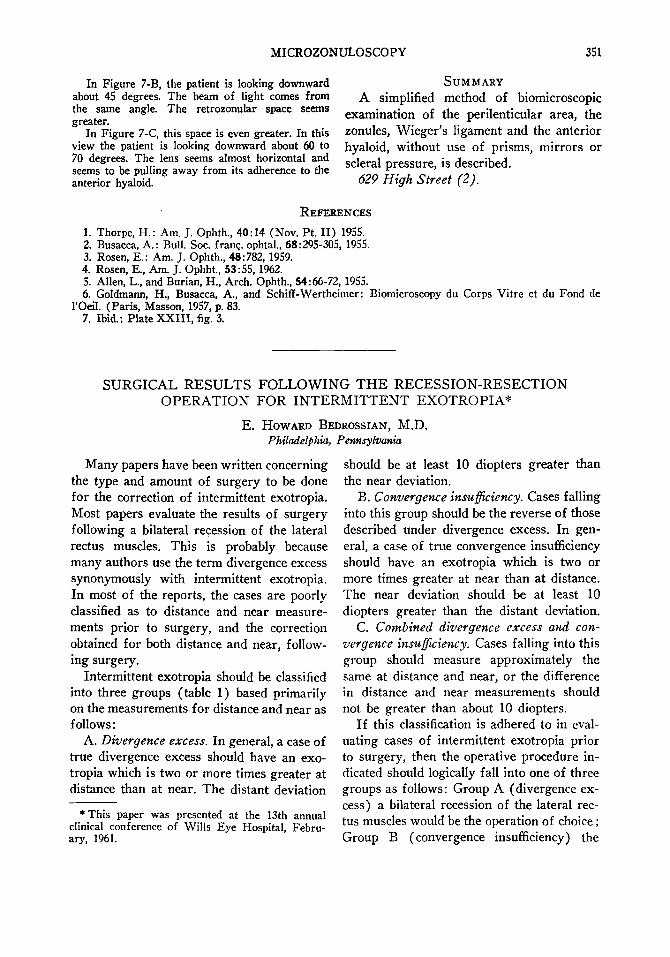
Fig. 7 (Rosen). Case 3. Examination at three different angles of the inferior perilenticular region of a 13-year-old girl. (A) Patient looking down about 30 degrees. The inferior plica (I.P.) is attached to the anterior hyaloid (A.H.) but a space seems to separate the ligament from its point of attachment, the space running beyond its usual limit. (B) In this view the abnormal spatial cleft is even more evident. The lens is inclined at about 45 degrees and the inferior plica sweeps up even more acutely. (C) In angulation of the lens to 60 to 70 degrees, the intercommunicating space is further elongated and the inferior plica is approximately vertical in direction.
This separation of the anterior hyaloid creates an intercommunicating path between Berger's space and the retrozonular space. Berger's space is only a potential space rendered visible in pathologic situations and limited in its boundary at the point of insertion of the posterior zonular fibers.
This has been clearly illustrated and nicely documented by Busacca.2 In cases of uveitis, Busacca has shown a detachment of the anterior hyaloid which thus creates a communication between Berger's space and the retrozonular space.7
The retrozonular space, so named by Gold-mann, is the space posterior to the posterior zonular fibers and anterior to the anterior hyaloid membrane. This, too, is a pathologic space known in the literature as Petit's space. Goldmann has proposed the self-explanatory terms of "infrazonular" space and "retrozonular" space which should eradicate any epynomic errors.
In Figure 6-B, the superior plica is seen to have dropped further and is now approaching the anterior hyaloid line which, in its inferior portion, seems to bow posteriorly and even more so in Figure 6-C. The posterior zonular fibers are seen extend
ing toward Wieger's ligament which is seen in the zone of specular reflection as diagonal white lines.
Because in Case 2, this nuclear involvement was in a fairly young individual, and because there was no peripheral lens opaci-fication (which is usual at the inferior pole of the lens phantom) it was possible to examine this inferior perilenticular area and to see the development of a potential Berger's space and its communication with the "retrozonular" space. The formation of this space may be of considerable significance in the explanation of the success or failure with the use of alpha chymotrypsin in congenital cataract extraction.
CASE 3
This 13-year-old girl presented a mild refractive problem. The pupils were widely dilated with the usual mydriatric agents. The study was made in three special views (fig. 7-A, B and C). In Figure 7-A the patient is looking down about 30 degrees. The inferior plica is seen at its attachment to the anterior hyaloid but a narrow space separates the ligament from its junction with the postlens capsule, the retrozonular space thus appearing to run beyond the mirror (zone of specular reflection) designating Wieger's ligament. This space seemed to become more pronounced as the patient looked increasingly downward.
MICROZONULOSCOPY 351
In Figure 7-B, the patient is looking downward about 45 degrees. The beam of light comes from the same angle. The retrozonular space seems greater.
In Figure 7-C, this space is even greater. In this view the patient is looking downward about 60 to 70 degrees. The lens seems almost horizontal and seems to be pulling away from its adherence to the anterior hyaloid.
Many papers have been written concerning the type and amount of surgery to be done for the correction of intermittent exotropia. Most papers evaluate the results of surgery following a bilateral recession of the lateral rectus muscles. This is probably because many authors use the term divergence excess synonymously with intermittent exotropia. In most of the reports, the cases are poorly classified as to distance and near measurements prior to surgery, and the correction obtained for both distance and near, following surgery.
Intermittent exotropia should be classified into three groups (table 1) based primarily on the measurements for distance and near as follows:
A. Divergence excess. In general, a case of true divergence excess should have an exotropia which is two or more times greater at distance than at near. The distant deviation
* This paper was presented at the 13th annual clinical conference of Wills Eye Hospital, February, 1961.
SUMMARY A simplified method of biomicroscopic
examination of the perilenticular area, the zonules, Wieger's ligament and the anterior hyaloid, without use of prisms, mirrors or scierai pressure, is described.
629 High Street (2).
should be at least 10 diopters greater than the near deviation.
B. Convergence insufficiency. Cases falling into this group should be the reverse of those described under divergence excess. In general, a case of true convergence insufficiency should have an exotropia which is two or more times greater at near than at distance. The near deviation should be at least 10 diopters greater than the distant deviation.
C. Combined divergence excess and convergence insufficiency. Cases falling into this group should measure approximately the same at distance and near, or the difference in distance and near measurements should not be greater than about 10 diopters.
If this classification is adhered to in evaluating cases of intermittent exotropia prior to surgery, then the operative procedure indicated should logically fall into one of three groups as follows: Group A (divergence excess) a bilateral recession of the lateral rectus muscles would be the operation of choice ; Group B (convergence insufficiency) the
REFERENCES
1. Thorpe, H.: Am. J. Ophth., 40:14 (Nov. Pt. II) 1955. 2. Busacca, A.: Bull. Soc. franc, ophtal., 68:295-305, 1955. 3. Rosen, E.: Am. J. Ophth., 48:782, 1959. 4. Rosen, E., Am. J. Ophht., 53:55, 1962. 5. Allen, L., and Burian, H., Arch. Ophth., 54:66-72, 1955. 6. Goldmann, H., Busacca, A., and Schiff-Wertheimer : Biomicroscopy du Corps Vitre et du Fond de
l'Oeil. (Paris, Masson, 1957, p. 83. 7. Ibid.: Plate XXIII, fig. 3.
SURGICAL RESULTS FOLLOWING T H E RECESSION-RESECTION OPERATION FOR INTERMITTENT EXOTROPIA*
E. HOWARD BEDROSSIAN, M.D. Philadelphia, Pennsylvania