Medicina SportivaMedicina Sportiva (2013), vol. IX, no 3, 2147-2159 Romanian Sports Medicine Society...
70
EDITORIAL STAFF Assoc. Prof. Mirela Maria Vasilescu - Editor-in-Chief Assoc. Prof. Anca Ionescu - Managing Editor EDITORIAL BOARD Apostol Adela - Bucharest, Romania Atanasescu Renee - Bucharest, Romania Busneag Răzvan - Bucharest, Romania Duma Eugen –Cluj Napoca, Romania Georgescu Mariana - Bucharest, Romania Panait Gabriel - Bucharest, Romania Popescu Alin - Bucharest, Romania Serbescu Ioan - Timisoara, Romania Siirghi Brandusa - Bucharest, Romania SCIENTIFIC REVIEW BOARD Avramescu Taina Elena - University of Craiova, Romania Berteanu Mihai - University of Medicine and Pharmacy Bucharest, Rehabilitation Department, Romania Bas Aslan Ummuhan – Pamukkale University, Denzli, Turkey Branzaniuc Klara – University of Medicine, Tg Mures, Anatomy Department, Romania Cavlak Ugur - Pamukkale University, School of Physical Therapy and Rehabilitation, Denzli, Turkey Cordun Mariana - National University of Physical Education and Sports, Bucharest, Romania Derevenco Petru - Romanian Academy of Medical Sciences, Romania Dikic Nenad - Anti-Doping Agency of Serbia, Sports Academy, Beograd, Serbia Dimitrova Diana – Sports Medicine Department, National Sports Academy, Sofia, Bulgaria Donatelli Robert - National Director of Specific Rehabilitation and Performance Enhancement Programs – Las Vegas, Nevada, USA Drosescu Paula – University A.I.Cuza, Faculty of Physical Education and Sport, Iasi, Romania Emin Ergen – University of Medicine, Ankara, EFSMA Executive Board, FIMS Executive Board, Turkey Gamze Ekici - Ahi Evran University, School of Physical Therapy and Rehabilitation, Kirsehie, Turkey Nastsis Konstantinos - Aristotle University of Thessaloniki, Greece Nestianu Valeriu - University of Medicine and Pharmacy Craiova, National Academy of Medical Sciences member, Romania Nica Adriana – University of Medicine and Pharmacy, Bucharest, Romania Oravitan Mihaela – West University of Timisoara, Romania Popescu Roxana - University of Medicine and Pharmacy Craiova, Romania Medicina Sportiva The Journal of Romanian Sport Medicine Society Vol. IX, No. 3 – 2013 15.09.2013
Transcript of Medicina SportivaMedicina Sportiva (2013), vol. IX, no 3, 2147-2159 Romanian Sports Medicine Society...
EDITORIAL STAFF
Assoc. Prof. Mirela Maria Vasilescu - Editor-in-Chief Assoc. Prof. Anca Ionescu - Managing Editor
EDITORIAL BOARD Apostol Adela - Bucharest, Romania Atanasescu Renee - Bucharest, Romania Busneag Răzvan - Bucharest, Romania Duma Eugen –Cluj Napoca, Romania Georgescu Mariana - Bucharest, Romania Panait Gabriel - Bucharest, Romania Popescu Alin - Bucharest, Romania Serbescu Ioan - Timisoara, Romania Siirghi Brandusa - Bucharest, Romania SCIENTIFIC REVIEW BOARD Avramescu Taina Elena - University of Craiova, Romania Berteanu Mihai - University of Medicine and Pharmacy Bucharest, Rehabilitation Department, Romania Bas Aslan Ummuhan – Pamukkale University, Denzli, Turkey Branzaniuc Klara – University of Medicine, Tg Mures, Anatomy Department, Romania Cavlak Ugur - Pamukkale University, School of Physical Therapy and Rehabilitation, Denzli, Turkey Cordun Mariana - National University of Physical Education and Sports, Bucharest, Romania Derevenco Petru - Romanian Academy of Medical Sciences, Romania Dikic Nenad - Anti-Doping Agency of Serbia, Sports Academy, Beograd, Serbia Dimitrova Diana – Sports Medicine Department, National Sports Academy, Sofia, Bulgaria Donatelli Robert - National Director of Specific Rehabilitation and Performance Enhancement Programs – Las Vegas, Nevada, USA Drosescu Paula – University A.I.Cuza, Faculty of Physical Education and Sport, Iasi, Romania Emin Ergen – University of Medicine, Ankara, EFSMA Executive Board, FIMS Executive Board, Turkey Gamze Ekici - Ahi Evran University, School of Physical Therapy and Rehabilitation, Kirsehie, Turkey Nastsis Konstantinos - Aristotle University of Thessaloniki, Greece Nestianu Valeriu - University of Medicine and Pharmacy Craiova, National Academy of Medical Sciences member, Romania Nica Adriana – University of Medicine and Pharmacy, Bucharest, Romania Oravitan Mihaela – West University of Timisoara, Romania Popescu Roxana - University of Medicine and Pharmacy Craiova, Romania
Medicina Sportiva The Journal of Romanian Sport Medicine Society Vol. IX, No. 3 – 2013 15.09.2013

ISSN 1841-0162
Publisher “Universitaria”, Brestei 156, 200177, Craiova, Romania Editorial Office Address: University of Craiova, Physical Education and Sports Faculty, Brestei 156, 200177, Craiova, Romania Site adress: http://www.medicinasportiva.ro Technical editor Eng. Aurora Beldiman (University of Craiova)

CONTENTS Vol. IX, No. 3 – 2013
A new approach to estimate the anaerobic capacity of the top athletes Apostol Adela, Ionescu Anca Mirela, Vasilescu Mirela, Mihai Berteanu
Comparison of the effects of laterally wedged insole with subtalar strapping and in-shoe lateral wedged insoles in women with knee osteoarthritis Senem Güner, Nesrin Yağci, Uğur Cavlak, Levent Özçakar
Salivary antioxidant enzymes in young exercised women Erfani Karimzadeh Toosi A, Rezaei A, Sariri Kh R Heritability in women and men of muscle strength of upper and lower limbs Elys Costa de Sousa, Michelle Vasconcelos de Oliveira, Fabiana Tenório, Vanessa Carla Monteiro Work related musculoskeletal disorders among administrators in a Nigerian university Ojoawo Adesola O, Oni Michael, Popoola O
Comparison of effectiveness of the extracorporeal shock wave therapy (ESWT) and steroid injection at plantar fasciitis treatment Mustafa Onur Serbest, Halil İbrahim Kaya, Mustafa Hilmi Demir, Sabriye Ercan, Cem Cetin Our experience in treating femoral diaphyseal fractures and their most common complications Radu Ciuvică, Mirela Vasilescu, Anca Bordianu, Ştefan Cristea
Beneficial effect of aerobic exercise and green tea on serum antioxidants Amani Sandyani S, Erfani Karimzadeh Toosi A, Sariri R, Razmi N Posterolateral knee instability in patients with anterior cruciate ligament lesion - clinical and MRI evaluation (case presentation) Ion Bogdan Codorean, Ioan Codorean, Stefan Mitulescu, Eduard Cernat
2147
2160
2166
2171
2177
2185
2191
2198
2203
Medicina Sportiva The Journal of Romanian Sport Medicine Society Vol. IX, No. 3 – 2013 15.09.2013


Medicina Sportiva (2013), vol. IX, no 3, 2147-2159 Romanian Sports Medicine Society
A new approach to estimate the anaerobic capacity of the top athletes Apostol Adela1, Ionescu Anca Mirela1, Vasilescu Mirela2, Mihai Berteanu3
1Sports Medicine Department, University of Medicine and Pharmacy Carol Davila, Bucharest, Romania 2Kinetotherapy and Sports Medicine Department, University of Craiova, Romania 3Medical Rehabilitation Department, University of Medicine and Pharmacy Carol Davila, Bucharest, Romania Abstract. In this study, it was achieved a parallel between one of the most used protocol for testing anaerobic effort capacity called the Wingate Test and the Total Work Performed Test, proposed by Szogy and Cherebetiu , which is used in Romania for about 4o years ago in order to estimate the top athletes. For this study the athletes performed only one 45 seconds maximal effort whereas data issued by the Monark cyclo-ergometer soft have been used to obtain both the significant parameters considered by the TW authors and the ones showed by Szogy and Cherebetiu within the Total Work Performed Test. This study results shoed high significant positive correlations existed between the Peak Power and the Total Work Performed on 10 seconds also between the Total Work Performed on 45 seconds and the Average Power on 30” (p<0.05 for all correlation coefficients). Key words: anaerobic capacity, Wingate test, Total Work Performed test, peak power, average power. Introduction In this study, it was achieved a parallel between one of the most used technique as to the anaerobic effort capacity called the Wingate test (1,2) and the test proposed by Szogy and Cherebetiu (3), which is used in Romania for about 4o years ago in order to estimate the top athletes. This work objective was not only to have in view the authentification of one of the tests and the non-authentification of the one but also to put into emphasize those parameters which give to the readers the most important information being useful for the training process. This study’s goal was the one to establish if there is a resemblance between the Wingate Test (TW) and the Total Work Performed Test performed by Szogy and Cherebetiu (TWPT). Moreover, the comparative estimation of parameters used within the Wingate Test and of the ones proposed by Szogy and Cherebetiu within the Total Worked Performed Test will lead to the way in which some indication will be issued to choose the optimal testing method on the anaerobic effort capacity depending on the features of sport test. This two testing types correlation’s establishment presents always the disadvantage in the way in which it is impossible to exactly show the
conditions the two tests occur: the match period, testing hours, equivalent environment and physiological conditions, partial determination of sports man to perform the two tests, etc. For the present case, these obstacles were canceled do to the fact the subjects (we’re referring to) put into effect only for a time the testing, the last one being understood by both proceedings. Further on, it is to be mentioned that for this study the athletes performed only one maximal effort whereas data issued by the Monark cycle-ergometer soft have been used to obtain both the significant parameters considered by the WT authors and the ones showed by Szogy and Cherebetiu within the TWPT. It is considered that on these terms, an eventually correlation making evident done between the results of both tests has got a high accuracy degree and it could show the validity and equivalence of the two testing methods (TW and TWPT). In addition to it, achievement at the same time of the TW and TWPT, tests study led to the issuing of more information relating to the anaerobic efforts intermediary phases: 5 seconds (PP in case of TW), 10 seconds and 20 seconds (Total Work Performed at 10 and 20 seconds from TWPT),
2147

A new approach to estimate the anaerobic capacity of the top athletes
Apostol Adela & all
Medicina Sportiva
2148 30 de seconds (AP from TW) and 45 seconds (Total Work Performed at 45 seconds from TWPT). The multitude of shown proceedings and of parameters considered to be defined for anaerobic skills by various authors (4-6) led to a great difficulty to establish a “common language” as to the marks obtained by the athletes during the testing. In spite of these differences, there are a few testing conditions which are seemed to be important for all these proceedings’ authors: the test has to be of maximum intensity in order to allow the highest percentage of energy given by the anaerobic sources and it is to be kept to estimate the body ability to keep the muscles work, as much as possible. The Wingate test (1, 2) and also the Total Work Performed Test described by Szogy and Cherebetiu (3) are proceedings which use the same maximal pedaling on the cyclo-ergometer. The TW needs a pedaling against a constancy braking resistance that is calculated depending on the body weight (e.g., 0.075 kp·kg-1). Although the proceeding of TWPT described by Szogy and Cherebetiu initially supposed that the effort to be performed on a gradual load cycle-ergometer, these days, testing took place on the same type of constancy load cyclo-ergometer as WT on which the same braking strength was used (e.g., 0.075 kp·kg-1). The two tests suggest different time periods to perform the standard effort: 30 seconds for the TW and 45 seconds for TWPT. Much moreover, difference between them is seen also through the physique parameters and periods of time on which determinations are performed. Thus, WT measures the average power on the periods of time of 5 respectively of 30 seconds whereas TWPT measures the total mechanical work performed on the periods of time of 10, 20 and respectively 45 seconds since the efforts have be done (TWP 10”, TWP 20” and TWP 45”). It is to be mentioned the fact that the original version of the TWPT set up a standard effort time of 60 seconds due to the authors’ views, establishment of Total Work performed till the end of first minute end of maximal effort gives significant information relating to the lactate limit of subject After a period of 45 seconds, the aerobic energetic systems part is significant to sustain the effort, so that, there is about the same contribution of the two systems, at the end of the
first minute of effort. For this reason, within the Romanian National Institute of Sports Medicine, testing time was diminished from 60 to 45 seconds. It was also imposed by the fact that the athletes bodies hardly tolerated such a period of time of maximal test and giving up of the effort was produced before the ending of testing period recommended by the authors, for many times. Material and Method The Romanian National and Olympic teams run over a pre-participation examination, every six month, at the Romanian National Institute of Sports Medicine (Bucharest, Romania). This study analyzed the results from 450 top athletes obtained during the assessment of the effort capacity, between January 2008– December 2010. The subjects were accordingly divided to the specifics of the athletic trial, in four groups.Group 1: 162 athletes participating in alactic anaerobic disciplines (100m, 200m sprints, 100 m hurdles, vertical jumps). The female group contained 85 athletes and the male group contained 77 athletes. Group 2: 62 athletes participating in anaerobic trials, but with an important lactic component: 400m sprints and 400m hurdles runners. The female group was made of 31 athletes, and the male group contained 31 athletes. Group 3: 156 athletes participating in sports with mixed energogenesis, aerobic and anaerobic: middle runners 800m and 1500m but also football and handball. The female group had 64 athletes, and the male group had 92 athletes. Group 4: 70 athletes participating in high endurance: marathon and race walk, of which 35 were women and 35 men. For every each team, interpretations have been separately for achieved for feminine and masculine subjects. There was the following final teams structure: alactic anaerobic tests - girls team (85) and boys team (77), lactic anaerobic tests - girls team (31) and boys team (31), mixed energogenesis tests - girls team (64) and boys team (92), aerobic tests girls team (35) and boys team (35). The testing protocol. The assessment of the anaerobic capacity was performed on a Monark 894-E, bicycle ergometer, wired to a computer using original, manufacturer-delivered software (Sports Medicine Industries, Inc. (SMI) (St. Cloud, MN) (Power software), software which can graphically represent the basic parameter of a
A new approach to estimate the anaerobic capacity of the top athletes Apostol Adela & all
Medicina Sportiva
2149 Wingate testing: the power. The resistance applied to the cycle-ergometer was calculated for each subject according to their body weight (kg multiplied with 7.5%). The data from each subject was introduced in the SMI Program software. Before collecting the data, and before applying the break on the wheel, the athlete pedaled without resistance for a few seconds, trying to reach the maximum speed in order to overcome the wheel’s inertia. Right after that, the assistant released the break weight and the software started collecting the data. All the subjects pedaled as fast as they could over a time span of 45 seconds. The athlete was verbally encouraged during the entire testing and was told every 5 seconds the time left until the end of the effort. Data analyses. The Monark bicycle soft performed counting of pedaling cycles, multiplies the pedaling number with the wheel circumference and with the strength applied on the wheel, then the resulted value is divided to 5 in order to obtain an average power on each 5 seconds time period. The registering values analysis allows showing of the parameters proposed by TW: Peak Power - PP (the highest value of average power measured on each time period of 5 consecutive seconds), Average Power -AP (average power registered during the 30 seconds of maximal effort ), Minimum Power - Pm (the lowest value of average power measured on each time period of 5 consecutive seconds), Power Drop (difference between the highest and the lowest value of power measured on time period of 5 seconds) and the fatigue index - FI (being a result of dividing the difference done between the Maximal Power and the Minimal Power to the Maximal Power, this result being multiplied with 100 ). The registering powers are expressed into Watt/s. Within this study testing fulfillment, the pedaling time period was extended to 45 seconds whereas the cycle- ergometer going on to registered for the whole testing period. Subsequent to it, results issued by soft have been used in order to obtain also the parameters recommended by Szogy-Cherebetiu: the total work performed (TWP) registering during the period of time of 10, 20 and 45 seconds. In this way, the total work performed for the proposed time periods (TWP 10”, TWP 20”, TWP 45”) is calculated by summing of the efforts performed for each 5 seconds time period issued by soft, which result from the average power values.
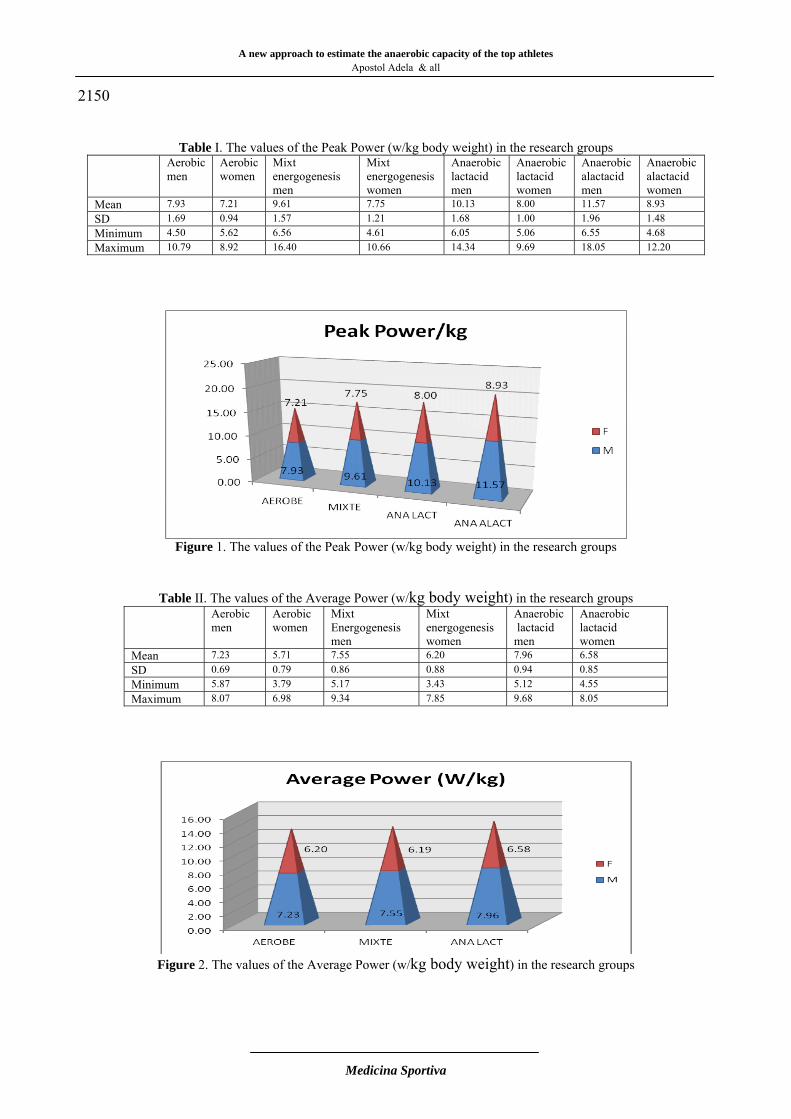
Subsequent to it, it is expressed TWP into kgm as an absolutely value (changing watt into kgm using formula 1 watt = 6.11829727787 kgm/min) and into kgm/kg body weight as a unitary or a relative (the TTR value is divided by the subject’s weight expressed into kg). Within this study there were followed up the relative values (kgm/kg body weight) obtained both for the TW (PP, AP) parameters and for the TWPT (TWP 10”, TWP 20”, TWP 45”) ones. The kg-body value was not used for the fatigue index because of the fact it represents a percentage value. The statistical analysis was performed using the standard statistical analysis of the Microsoft Excel software and included: medium values, standard deviations (SD) and value intervals for the parameters measured. The comparison between the levels of these parameters for each separate group was done using the Student test. The correlations between parameters were evaluated through the Pearson correlation method and the level of signification was considered at p<0.05. Results Peak Power. The peak power (PP) expressed as a relative size (W/kg body weight) registered the following values per studied teams: aerobic feminine tests 7.21±0.94, aerobic masculine tests 7.93±1.69, feminine mixed energogenesis tests 7.75 ± 1.21, masculine mixed energogenesis tests 9.61±1.57, feminine alactic aerobic tests 8±1 whereas for masculine 10.13±1.68, feminine alactic aerobic tests 8.93±1.48 whereas for masculine 11.57±1.96. The plotting shows that the athletes trained for the alactic anaerobic tests get the highest values, being followed by the lactic anaerobic tests ones and by the mixed energogenesis tests ones, whereas these parameter lowest values to be registered for the athletes teams who take part in the aerobic tests. Average Power. Further on , it is to be mentioned the fact that the Average Power parameter per kg body weight per 30”, that is recommended by the Wingate test protocol register the same rising trend as the Peak Power on the way in which the respective sports require a bigger aerobic metabolism and an aerobic one into a low percentage.
A new approach to estimate the anaerobic capacity of the top athletes
Apostol Adela & all
Medicina Sportiva
2150
Table I. The values of the Peak Power (w/kg body weight) in the research groups
Aerobic men
Aerobic women
Mixt energogenesis men
Mixt energogenesis women
Anaerobic lactacid men
Anaerobic lactacid women
Anaerobic alactacid men
Anaerobic alactacid women
Mean 7.93 7.21 9.61 7.75 10.13 8.00 11.57 8.93 SD 1.69 0.94 1.57 1.21 1.68 1.00 1.96 1.48 Minimum 4.50 5.62 6.56 4.61 6.05 5.06 6.55 4.68 Maximum 10.79 8.92 16.40 10.66 14.34 9.69 18.05 12.20
Figure 1. The values of the Peak Power (w/kg body weight) in the research groups
Table II. The values of the Average Power (w/kg body weight) in the research groups Aerobic
men Aerobic women
Mixt Energogenesis men
Mixt energogenesis women
Anaerobic lactacid men
Anaerobic lactacid women
Mean 7.23 5.71 7.55 6.20 7.96 6.58 SD 0.69 0.79 0.86 0.88 0.94 0.85 Minimum 5.87 3.79 5.17 3.43 5.12 4.55 Maximum 8.07 6.98 9.34 7.85 9.68 8.05
Figure 2. The values of the Average Power (w/kg body weight) in the research groups
A new approach to estimate the anaerobic capacity of the top athletes Apostol Adela & all
Medicina Sportiva
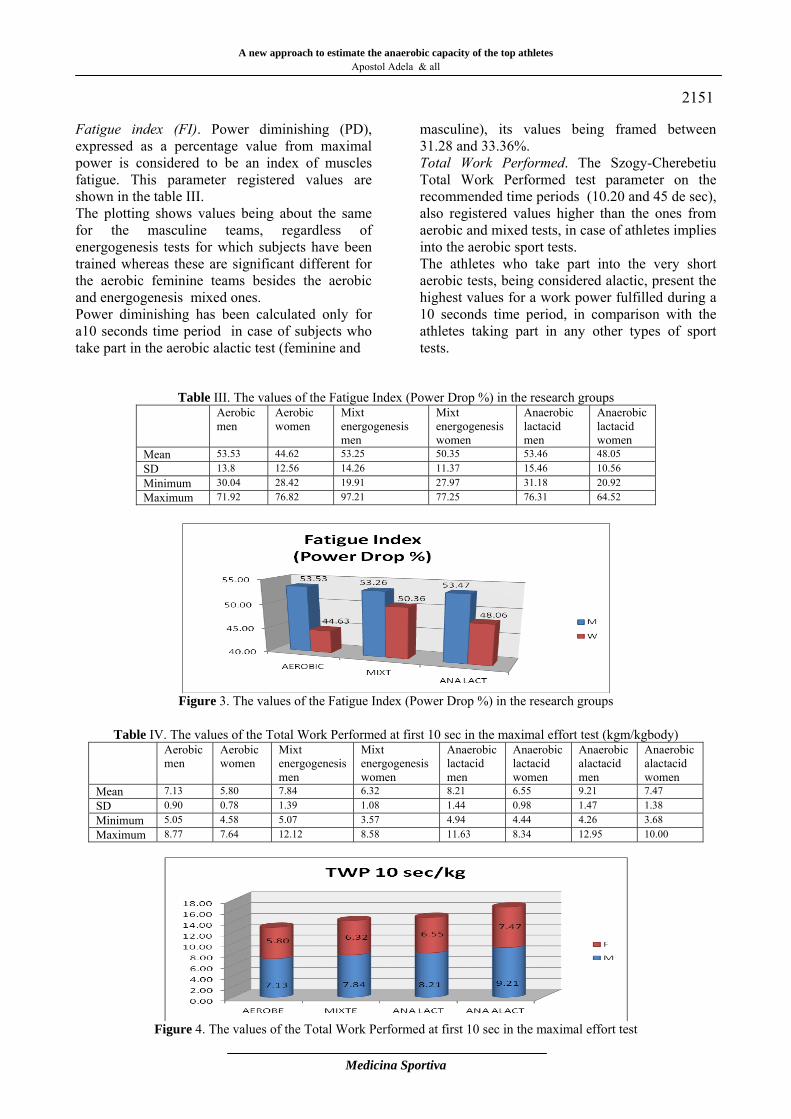
2151 Fatigue index (FI). Power diminishing (PD), expressed as a percentage value from maximal power is considered to be an index of muscles fatigue. This parameter registered values are shown in the table III. The plotting shows values being about the same for the masculine teams, regardless of energogenesis tests for which subjects have been trained whereas these are significant different for the aerobic feminine teams besides the aerobic and energogenesis mixed ones. Power diminishing has been calculated only for a10 seconds time period in case of subjects who take part in the aerobic alactic test (feminine and
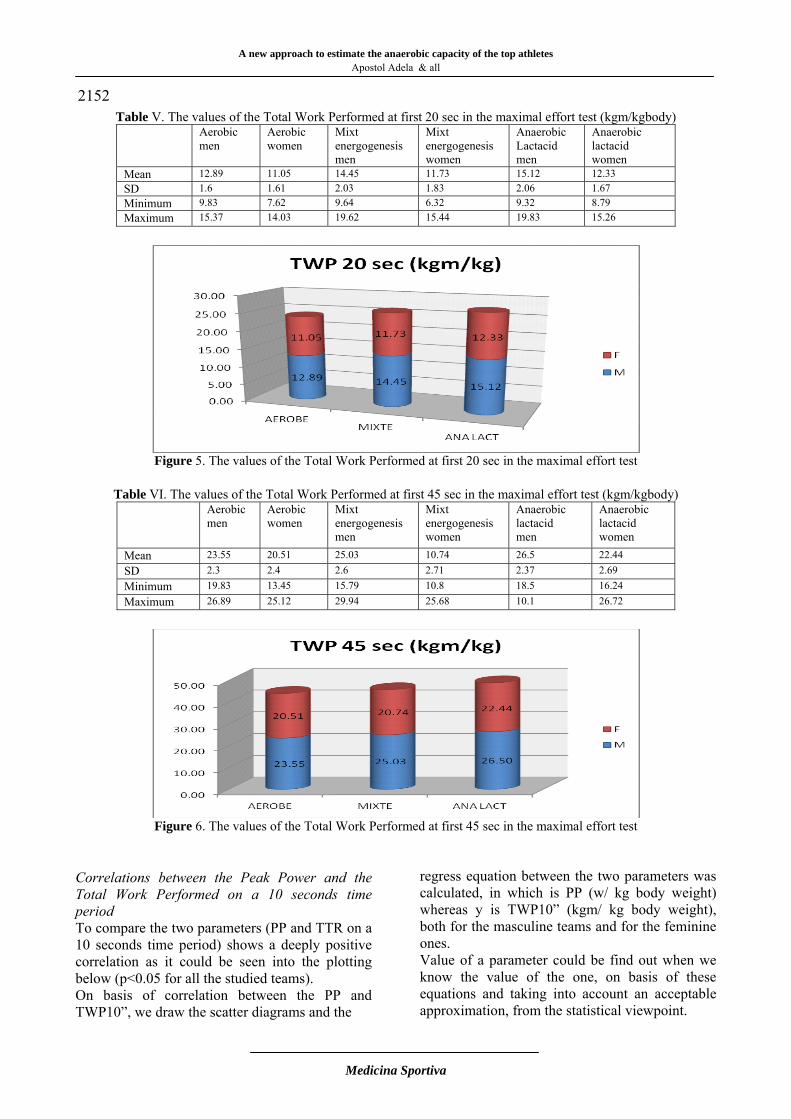
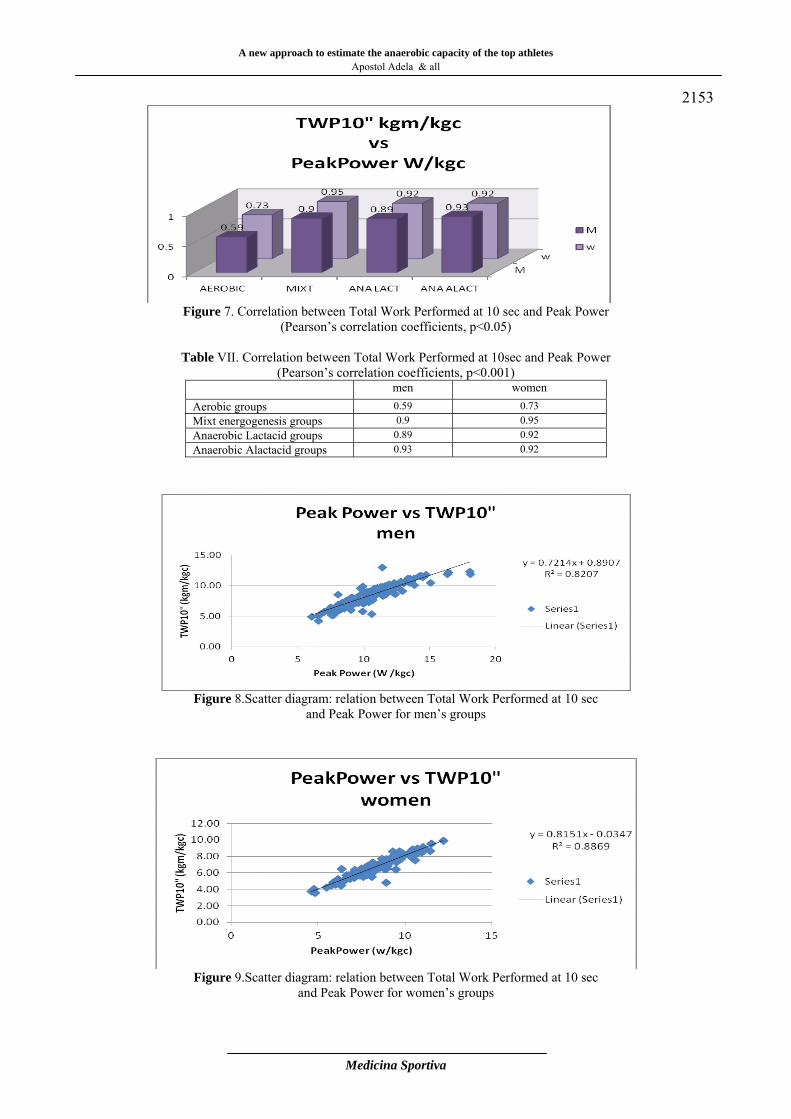
masculine), its values being framed between 31.28 and 33.36%. Total Work Performed. The Szogy-Cherebetiu Total Work Performed test parameter on the recommended time periods (10.20 and 45 de sec), also registered values higher than the ones from aerobic and mixed tests, in case of athletes implies into the aerobic sport tests. The athletes who take part into the very short aerobic tests, being considered alactic, present the highest values for a work power fulfilled during a 10 seconds time period, in comparison with the athletes taking part in any other types of sport tests.
Table III. The values of the Fatigue Index (Power Drop %) in the research groups Aerobic
men Aerobic women
Mixt energogenesis men
Mixt energogenesis women
Anaerobic lactacid men
Anaerobic lactacid women
Mean 53.53 44.62 53.25 50.35 53.46 48.05 SD 13.8 12.56 14.26 11.37 15.46 10.56 Minimum 30.04 28.42 19.91 27.97 31.18 20.92 Maximum 71.92 76.82 97.21 77.25 76.31 64.52
Figure 3. The values of the Fatigue Index (Power Drop %) in the research groups
Table IV. The values of the Total Work Performed at first 10 sec in the maximal effort test (kgm/kgbody)
Aerobic men
Aerobic women
Mixt energogenesis men
Mixt energogenesis women
Anaerobic lactacid men
Anaerobic lactacid women
Anaerobic alactacid men
Anaerobic alactacid women
Mean 7.13 5.80 7.84 6.32 8.21 6.55 9.21 7.47 SD 0.90 0.78 1.39 1.08 1.44 0.98 1.47 1.38 Minimum 5.05 4.58 5.07 3.57 4.94 4.44 4.26 3.68 Maximum 8.77 7.64 12.12 8.58 11.63 8.34 12.95 10.00
Figure 4. The values of the Total Work Performed at first 10 sec in the maximal effort test
A new approach to estimate the anaerobic capacity of the top athletes
Apostol Adela & all
Medicina Sportiva
2152 Table V. The values of the Total Work Performed at first 20 sec in the maximal effort test (kgm/kgbody)
Aerobic men
Aerobic women
Mixt energogenesis men
Mixt energogenesis women
Anaerobic Lactacid men
Anaerobic lactacid women
Mean 12.89 11.05 14.45 11.73 15.12 12.33 SD 1.6 1.61 2.03 1.83 2.06 1.67 Minimum 9.83 7.62 9.64 6.32 9.32 8.79 Maximum 15.37 14.03 19.62 15.44 19.83 15.26
Figure 5. The values of the Total Work Performed at first 20 sec in the maximal effort test
Table VI. The values of the Total Work Performed at first 45 sec in the maximal effort test (kgm/kgbody)
Aerobic men
Aerobic women
Mixt energogenesis men
Mixt energogenesis women
Anaerobic lactacid men
Anaerobic lactacid women
Mean 23.55 20.51 25.03 10.74 26.5 22.44 SD 2.3 2.4 2.6 2.71 2.37 2.69 Minimum 19.83 13.45 15.79 10.8 18.5 16.24 Maximum 26.89 25.12 29.94 25.68 10.1 26.72
Figure 6. The values of the Total Work Performed at first 45 sec in the maximal effort test
Correlations between the Peak Power and the Total Work Performed on a 10 seconds time period To compare the two parameters (PP and TTR on a 10 seconds time period) shows a deeply positive correlation as it could be seen into the plotting below (p<0.05 for all the studied teams). On basis of correlation between the PP and TWP10”, we draw the scatter diagrams and the
regress equation between the two parameters was calculated, in which is PP (w/ kg body weight) whereas y is TWP10” (kgm/ kg body weight), both for the masculine teams and for the feminine ones. Value of a parameter could be find out when we know the value of the one, on basis of these equations and taking into account an acceptable approximation, from the statistical viewpoint.
A new approach to estimate the anaerobic capacity of the top athletes Apostol Adela & all
Medicina Sportiva
2153
Figure 7. Correlation between Total Work Performed at 10 sec and Peak Power
(Pearson’s correlation coefficients, p<0.05)
Table VII. Correlation between Total Work Performed at 10sec and Peak Power (Pearson’s correlation coefficients, p<0.001)
men women Aerobic groups 0.59 0.73 Mixt energogenesis groups 0.9 0.95 Anaerobic Lactacid groups 0.89 0.92 Anaerobic Alactacid groups 0.93 0.92
Figure 8.Scatter diagram: relation between Total Work Performed at 10 sec
and Peak Power for men’s groups
Figure 9.Scatter diagram: relation between Total Work Performed at 10 sec
and Peak Power for women’s groups
A new approach to estimate the anaerobic capacity of the top athletes
Apostol Adela & all
Medicina Sportiva
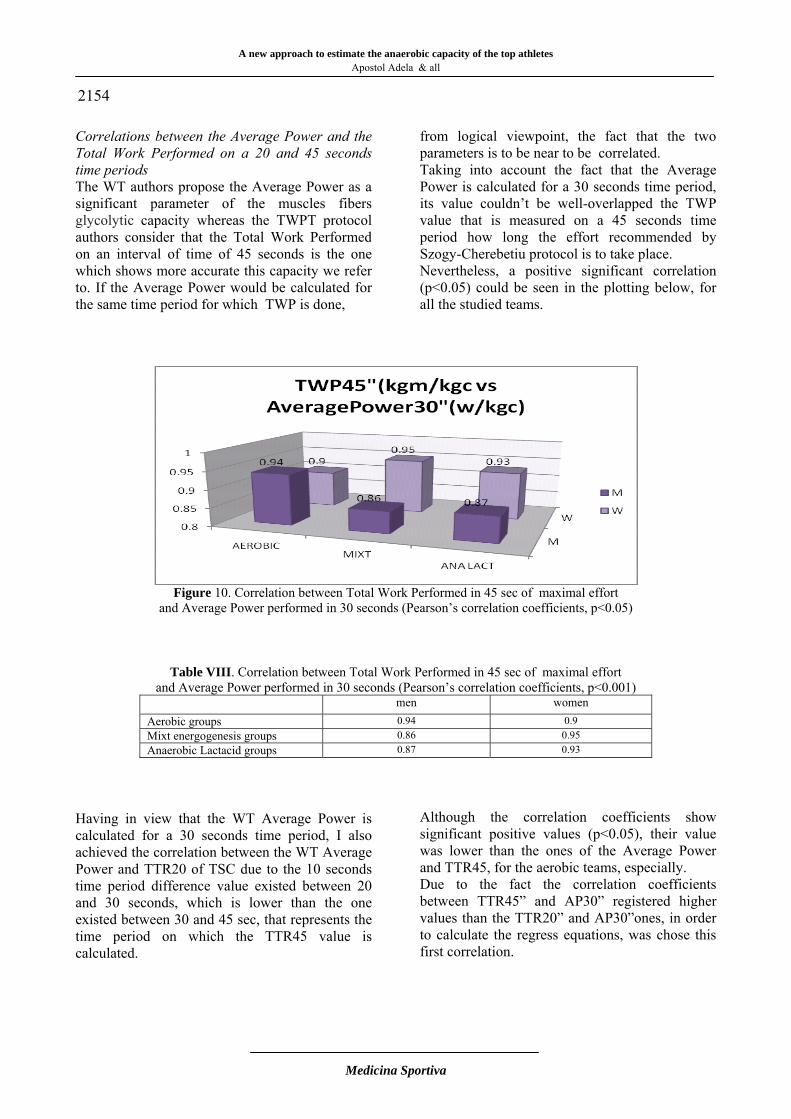
2154 Correlations between the Average Power and the Total Work Performed on a 20 and 45 seconds time periods The WT authors propose the Average Power as a significant parameter of the muscles fibers glycolytic capacity whereas the TWPT protocol authors consider that the Total Work Performed on an interval of time of 45 seconds is the one which shows more accurate this capacity we refer to. If the Average Power would be calculated for the same time period for which TWP is done,
from logical viewpoint, the fact that the two parameters is to be near to be correlated. Taking into account the fact that the Average Power is calculated for a 30 seconds time period, its value couldn’t be well-overlapped the TWP value that is measured on a 45 seconds time period how long the effort recommended by Szogy-Cherebetiu protocol is to take place. Nevertheless, a positive significant correlation (p<0.05) could be seen in the plotting below, for all the studied teams.
Figure 10. Correlation between Total Work Performed in 45 sec of maximal effort
and Average Power performed in 30 seconds (Pearson’s correlation coefficients, p<0.05)
Table VIII. Correlation between Total Work Performed in 45 sec of maximal effort and Average Power performed in 30 seconds (Pearson’s correlation coefficients, p<0.001)
men women Aerobic groups 0.94 0.9 Mixt energogenesis groups 0.86 0.95 Anaerobic Lactacid groups 0.87 0.93
Having in view that the WT Average Power is calculated for a 30 seconds time period, I also achieved the correlation between the WT Average Power and TTR20 of TSC due to the 10 seconds time period difference value existed between 20 and 30 seconds, which is lower than the one existed between 30 and 45 sec, that represents the time period on which the TTR45 value is calculated.
Although the correlation coefficients show significant positive values (p<0.05), their value was lower than the ones of the Average Power and TTR45, for the aerobic teams, especially. Due to the fact the correlation coefficients between TTR45” and AP30” registered higher values than the TTR20” and AP30”ones, in order to calculate the regress equations, was chose this first correlation.
A new approach to estimate the anaerobic capacity of the top athletes Apostol Adela & all
Medicina Sportiva
2155
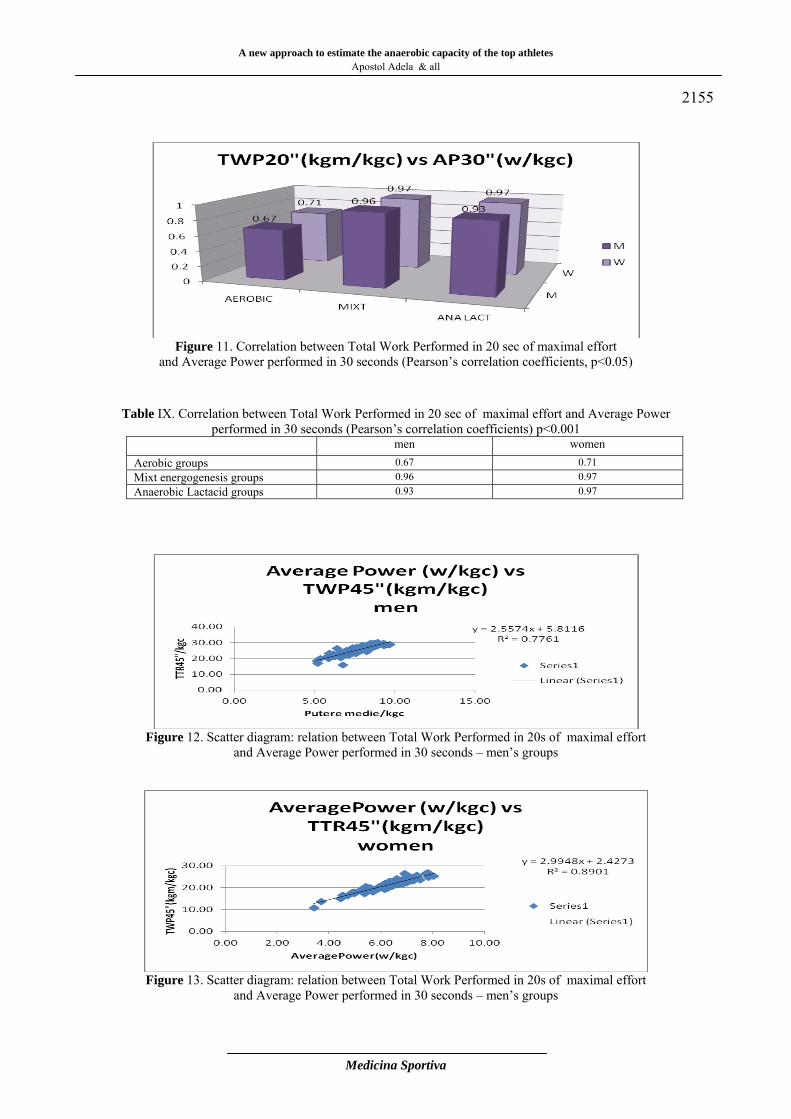
Figure 11. Correlation between Total Work Performed in 20 sec of maximal effort
and Average Power performed in 30 seconds (Pearson’s correlation coefficients, p<0.05)
Table IX. Correlation between Total Work Performed in 20 sec of maximal effort and Average Power
performed in 30 seconds (Pearson’s correlation coefficients) p<0.001 men women Aerobic groups 0.67 0.71 Mixt energogenesis groups 0.96 0.97 Anaerobic Lactacid groups 0.93 0.97
Figure 12. Scatter diagram: relation between Total Work Performed in 20s of maximal effort
and Average Power performed in 30 seconds – men’s groups
Figure 13. Scatter diagram: relation between Total Work Performed in 20s of maximal effort
and Average Power performed in 30 seconds – men’s groups
A new approach to estimate the anaerobic capacity of the top athletes
Apostol Adela & all
Medicina Sportiva
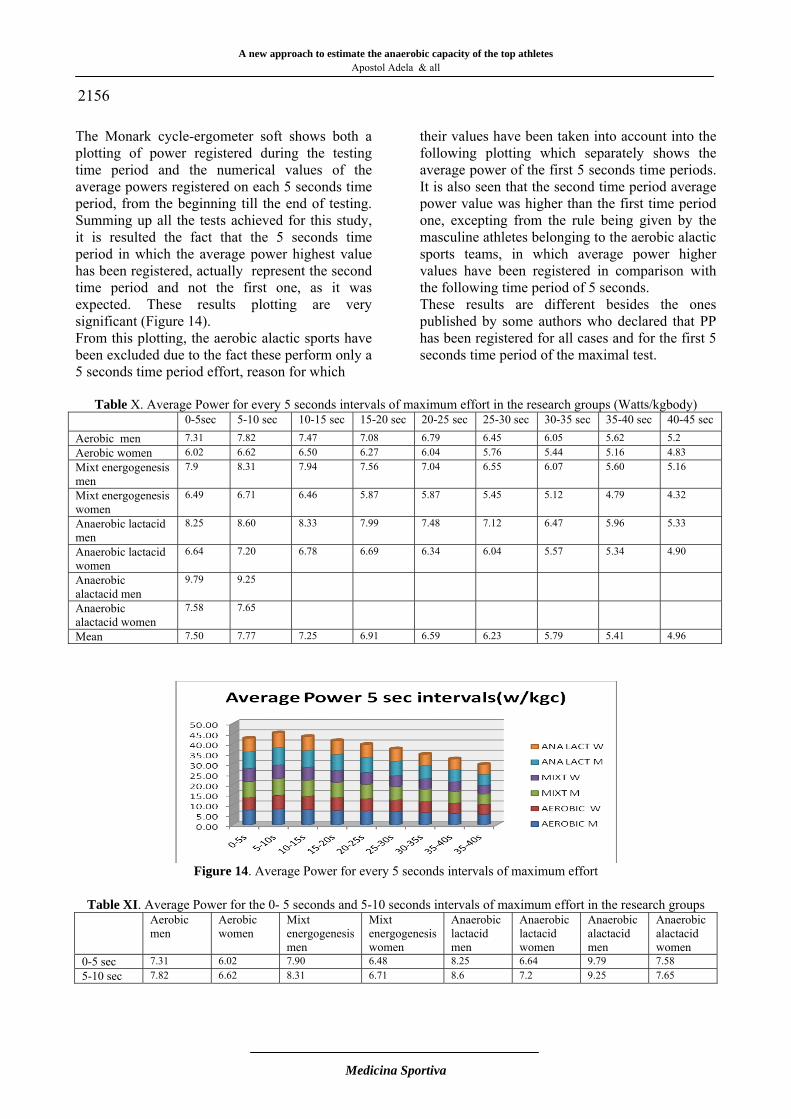
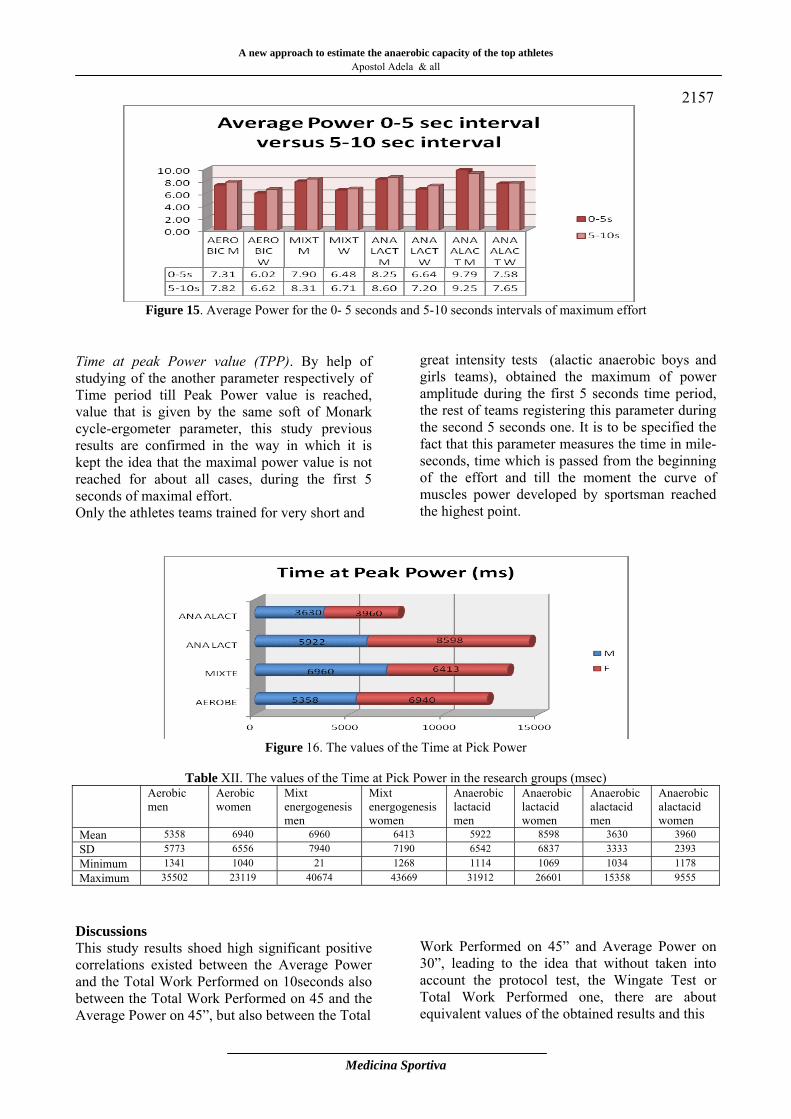
2156 The Monark cycle-ergometer soft shows both a plotting of power registered during the testing time period and the numerical values of the average powers registered on each 5 seconds time period, from the beginning till the end of testing. Summing up all the tests achieved for this study, it is resulted the fact that the 5 seconds time period in which the average power highest value has been registered, actually represent the second time period and not the first one, as it was expected. These results plotting are very significant (Figure 14). From this plotting, the aerobic alactic sports have been excluded due to the fact these perform only a 5 seconds time period effort, reason for which
their values have been taken into account into the following plotting which separately shows the average power of the first 5 seconds time periods. It is also seen that the second time period average power value was higher than the first time period one, excepting from the rule being given by the masculine athletes belonging to the aerobic alactic sports teams, in which average power higher values have been registered in comparison with the following time period of 5 seconds. These results are different besides the ones published by some authors who declared that PP has been registered for all cases and for the first 5 seconds time period of the maximal test.
Table X. Average Power for every 5 seconds intervals of maximum effort in the research groups (Watts/kgbody) 0-5sec 5-10 sec 10-15 sec 15-20 sec 20-25 sec 25-30 sec 30-35 sec 35-40 sec 40-45 sec Aerobic men 7.31 7.82 7.47 7.08 6.79 6.45 6.05 5.62 5.2 Aerobic women 6.02 6.62 6.50 6.27 6.04 5.76 5.44 5.16 4.83 Mixt energogenesis men
7.9 8.31 7.94 7.56 7.04 6.55 6.07 5.60 5.16
Mixt energogenesis women
6.49 6.71 6.46 5.87 5.87 5.45 5.12 4.79 4.32
Anaerobic lactacid men
8.25 8.60 8.33 7.99 7.48 7.12 6.47 5.96 5.33
Anaerobic lactacid women
6.64 7.20 6.78 6.69 6.34 6.04 5.57 5.34 4.90
Anaerobic alactacid men
9.79 9.25
Anaerobic alactacid women
7.58 7.65
Mean 7.50 7.77 7.25 6.91 6.59 6.23 5.79 5.41 4.96
Figure 14. Average Power for every 5 seconds intervals of maximum effort
Table XI. Average Power for the 0- 5 seconds and 5-10 seconds intervals of maximum effort in the research groups
Aerobic men
Aerobic women
Mixt energogenesis men
Mixt energogenesis women
Anaerobic lactacid men
Anaerobic lactacid women
Anaerobic alactacid men
Anaerobic alactacid women
0-5 sec 7.31 6.02 7.90 6.48 8.25 6.64 9.79 7.58 5-10 sec 7.82 6.62 8.31 6.71 8.6 7.2 9.25 7.65
A new approach to estimate the anaerobic capacity of the top athletes Apostol Adela & all
Medicina Sportiva
2157
Figure 15. Average Power for the 0- 5 seconds and 5-10 seconds intervals of maximum effort
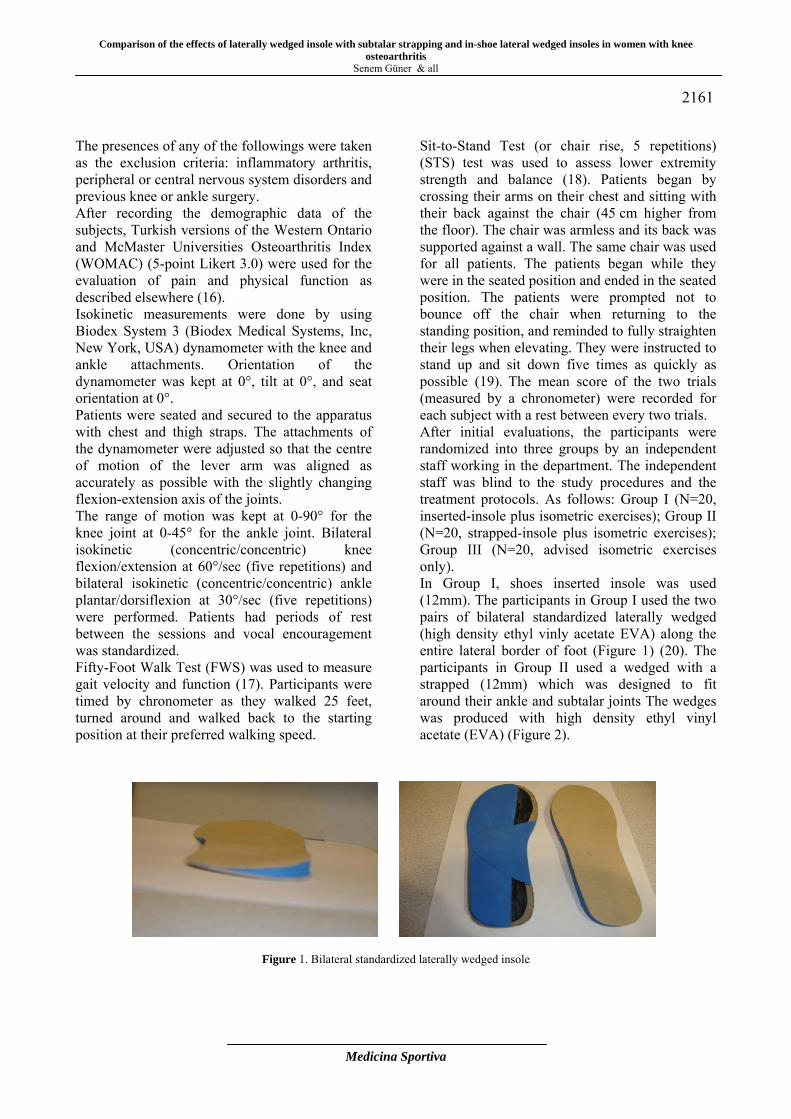
Time at peak Power value (TPP). By help of studying of the another parameter respectively of Time period till Peak Power value is reached, value that is given by the same soft of Monark cycle-ergometer parameter, this study previous results are confirmed in the way in which it is kept the idea that the maximal power value is not reached for about all cases, during the first 5 seconds of maximal effort. Only the athletes teams trained for very short and
great intensity tests (alactic anaerobic boys and girls teams), obtained the maximum of power amplitude during the first 5 seconds time period, the rest of teams registering this parameter during the second 5 seconds one. It is to be specified the fact that this parameter measures the time in mile-seconds, time which is passed from the beginning of the effort and till the moment the curve of muscles power developed by sportsman reached the highest point.
Figure 16. The values of the Time at Pick Power
Table XII. The values of the Time at Pick Power in the research groups (msec)
Aerobic men
Aerobic women
Mixt energogenesis men
Mixt energogenesis women
Anaerobic lactacid men
Anaerobic lactacid women
Anaerobic alactacid men
Anaerobic alactacid women
Mean 5358 6940 6960 6413 5922 8598 3630 3960 SD 5773 6556 7940 7190 6542 6837 3333 2393 Minimum 1341 1040 21 1268 1114 1069 1034 1178 Maximum 35502 23119 40674 43669 31912 26601 15358 9555
Discussions This study results shoed high significant positive correlations existed between the Average Power and the Total Work Performed on 10seconds also between the Total Work Performed on 45 and the Average Power on 45”, but also between the Total
Work Performed on 45” and Average Power on 30”, leading to the idea that without taken into account the protocol test, the Wingate Test or Total Work Performed one, there are about equivalent values of the obtained results and this

A new approach to estimate the anaerobic capacity of the top athletes
Apostol Adela & all
Medicina Sportiva
2158 is reason the regress equation have been calculated in order to find out parameters recommended by the Wingate Test when the results obtained by the Total Work Performed Test are known and also the reverse way. Notwithstanding, even the differences registered between the results of two types of testing aren’t significant from the statistically viewpoint, we considered that these show slight different aspects of the anaerobic effort capacity. Also the muscles power is the explosive aspect of the strength (7) it is important to be remarked the fact that it gets three aspects, such as: the maximum power (maximum power amplitude), the explosive power (speed used to reach the maximum power), and the “endurance power” (time period in which maximal power value could be kept). For instance a running test is won not by the athlete who develop the highest power value establish on a given time (aspect of maximum power amplitude) but by the one who develops a highest power value during all time the running test takes (aspect of “endurance power”). This aspect is more exactly given by physical sizes such as: the average power of test or the mechanical work totally achieved on a period of time that is specified to the test. (P = L/t). In turn of it, the aspect of explosive power is very important within the sports tests, such as jumping and throwing when the own body or an object is propelled like a missile. Sometimes, relating to the explosive power, it is used the term of "neuro-muscles power" just to show the importance the factors that influence the energy (speed on neuro-motor fibers recruitment, the speed on muscles contraction and hydrolysis rate of ATP) have on this parameter, rather than the increased production of energy. The aspect of explosive power, unlike the power endurance mostly depends on how fast fibers muscles shrink, how fast can they be co-opted by neuronal factors and rather than the availability of energy sources. There are even authors who believe that the power developed by certain movements or by specific activities is almost exclusively the result of learnt actions and improving the motor technique is the main factor that produces improving the explosive power (8, 9). Within a study published by Bell and Cobner, the authors concluded: "The value of maximum power and of the average one, also the profile corresponding to the generated power are better represented than by the cross-temporal analysis" (10).
More over, in this study we found significant negative correlations between time to reach the maximum power and maximum power for the alactic anaerobic teams and for the mixed energogenesis ones. Teams who achieved a significant negative correlation between PP and TPP were teams consisting of athletes for that the neuro-motor skills and movement pattern are very important for performance and their improvement through specific training may be an explanation for the results achieved. Thus, the alactic anaerobic teams were composed of athletes participating within the jumping and throwing tests whereas the mixed energogenesis teams were predominantly composed of athletes participating within the sports games tests (football, handball) in which jumps and throws are also practiced. Conclusions Although we obtained very high correlations between the Wingate Test parameters and the Total Work Performed Test ones, a deeply analysis of all the aspects on the anaerobic performance should include both the Wingate Test parameters and the Total Work Performed Test ones. For each sport test, it would be necessary to use those testing parameters that can give the most information on the specific issues on which the performance depends. We recommend that when the explosive anaerobic muscles power is very important for performance, the parameter preferred within the testing to be considered the Peak Power. Although it wasn’t in mind in this study from the statistically viewpoint, we consider that another parameter that is the "instantaneous maximum power", meaning the maximum amplitude of the power curve recorded by the Monark cycle-ergometer soft is preferred instead of the current Peak Power parameter. For the anaerobic alactic tests of jumping, throwing, weightlifting and as well as, of sports games in which are important aspects of speed the ball reaches after the kick, detention, etc. this parameter test is particularly useful. Studies achieved subsequent may show that the explosive movements performance is better supported with this parameter than with the Peak Power calculated on a time period of 5 seconds. Also, although it hasn’t been used till now, we believe that the temporal analysis of power curve and especially the Time parameter on Peak Power are important to be evaluated in testing the athletes from such a type of sport tests as they can provide information on when the muscles

A new approach to estimate the anaerobic capacity of the top athletes Apostol Adela & all
Medicina Sportiva
2159 generates maximum power and can be a feedback of neuromuscular factors training. For tests in which the endurance aspect of anaerobic power is more important than the explosive one (lactic anaerobic tests), for testing should be preferred parameters specific to the Total Work Performed measured on the time periods specific to the test which give general information on the performance for the respective test. . Determination of the Total Work Performed done on time periods shouldn’t be absent from testing of samples that lasts more than 10 seconds as it provides valuable information about the two energogenesis systems involved: the anaerobic glycolysis and high-energy phosphates system. We support the recommendations made by Szogy and Cherebetiu relating to the Total Work Performed Test for a 10 sec time period to investigate capacity high-energy phosphates compounds, The Total Work achieved for a 20 sec time period in case of to anaerobic glycolysis and The Total Work achieved for a 45 sec time period, being an indicator for tolerance to acidosis, so important to obtain performance in many sport tests. References 1. Inbar O, Bar-Or O, Skinner JS (1996). The
Wingate anaerobic test. Human Kinetiks, Chapaign ÎL.
2. Bar-Or O (1994). Testing of anaerobic performance by the Wingate anaerobic test. ERS Tech, Tel Aviv.
3. Szogy A, Cherebetiu G (1974). A one-minute bicycle ergometer test for determination of anaerobic capacity. European Journal of Applied Physiology and Occupational Physiology: 33(2): 171-176.
4. Bosco C, Luhtanen P, Komi PV (1983) A simple method for measurement of mechanical power in jumping. European Journal of Applied Physiology 50:273-282.
5. Margaria, R., P. Aghemo and E. Rovelli. (1966). Measurement of muscular power (anaerobic) in man. Journal of Applied Physiology .21:5, p. 1662-1664.
6. Georgescu, Miron, (1953), Contributii la studiul calitătilor fizice. În: Cultura fizică si sport. Bucuretti, nr.2, pg. 39-60
7. Sargeant AJ. Anaerobic performance. In: Armstrong N, VanMechelen W (eds), Pediatric exercise science and medicine.Oxford University Press, Oxford, 2000: 143−151.
8. Brukner P, Khan K (2001) Clinical Sports
Medicine. Second Edition. McGraw-Hill Book Co, Sydney.
9. Grabe S A, Widule CJ (1988). Comparative Biomechanics of the Jerk in Olympic Weightlifting. Research Quarterly for Exercise and Sport; 59(1): 1-8.
10. Bell W, Cobner DM (2007). Effect of individual time to peak power output on the expression of peak power output în the 30-s Wingate Anaerobic Test. Int J Sports Med; 28(2):135-9.
Corresponding Author Adela Apostol Sports Medicine Department, University of Medicine and Pharmacy Carol Davila, Bucharest, Romania E-mail: [email protected]
Received: June 10, 2013 Accepted: August 12, 2013

Medicina Sportiva (2013), vol. IX, no 3, 2160-2165 Romanian Sports Medicine Society
Comparison of the effects of laterally wedged insole with subtalar strapping and in-shoe lateral wedged insoles in women with knee osteoarthritis Senem Güner1, Nesrin Yağci 2, Uğur Cavlak 2, Levent Özçakar3
1Ankara University School of Health Care Professions Department of Prosthetics and Orthotics, Turkey 2 Pamukkale University, School of Physical Therapy and Rehabilitation, Turkey 3 Hacettepe University Medical School Department of Physical Medicine and Rehabilitation, Turkey Abstract. Aim and scope. The aim of this study was to identify the effects of laterally wedged insole and laterally wedged subtalar strapping application on muscle strength, functional state; and to compare their effects in women with knee osteoarthritis (OA). Materials and Methods. Sixty women (aged between 45-65 years) with OA were enrolled in this study. Lateral wedged insole was used in 20 women (Group 1), laterally wedged subtalar strapping in 20 women (Group 2) and women in Group 3 only received physical therapy program. Isokinetic testing for knee and ankle muscles, 50-foot walking test, 5-time repeated sit to stand test, WOMAC were performed prior to treatment and 8 weeks after treatment. Results. Knee and ankle muscle strength, functional test results and WOMAC scores improved in Groups I and II (pre- vs. post-treatment) (p<0.05). In Group III, despite the improvement in all the other test results, muscle strength was found not to have increased (p>0.05). The most significant improvement between the 3 groups is shown in group I. Conclusion. Our results show that application of laterally wedged insole and laterally wedged subtalar strapping leads to increasing knee and ankle muscle strength in addition to their positive effects on pain intensity, physical function. Key words: knee osteoarthritis, subtalar strapping, laterally wedged insole, isokinetic strength. Introduction Knee osteoarthritis (OA) is a leading cause of chronic pain and disability in the adult population. The medial tibiofemoral compartment is involved nearly 10 times more frequently than the lateral compartment (1). Therefore, progressive loss of cartilage and joint space typically results in varus malalignment, joint pain, increasing the load across the medial compartment (2-4). Management of knee OA aims to reduce pain and optimize physical function while minimizing adverse side effects of therapy. Hence, conservative, and especially nonpharmacologic, treatments are desirable. The laterally wedged insoles have been recommended as an efficacious method in this regard (5,6). Several studies have shown that they effectively reduce the load at the medial compartment of the knee joint (7-10). Thereby, optimizing the gait pattern of the patients, these insoles are considered to decrease pain and restore function. Van Raaij et al. (11) suggested that, a laterally wedged insole may be alternative to valgus bracing for noninvasively treating symptoms of medial knee OA. Recently, it has been also suggested that the additional use
of elastic subtalar strapping particularly in mild and moderate knee OA (12-14). On the other hand, no study has evaluated the effects of lateral wedge insole use with or without subtalar strapping on the lower extremity muscle strength. Accordingly, the purpose of this study was to identify the effects of laterally wedged insole and laterally wedged subtalar strapping application on muscular strength and functional state in women with knee osteoarthritis. Material and Method Sixty female patients who were diagnosed with bilaterally medial compartment knee OA according to the American College of Rheumatology criteria for the diagnosis of knee OA were enrolled (15). Subjects were informed about the study procedure and they consented to participate. All subjects had grade ≥2OA according to Kellgren Lawrence scale. The study was approved by the Local Ethics Committee. This study was supported by Pamukkale University Scientific Research Projects Commission (2008SBE007).
2160
Comparison of the effects of laterally wedged insole with subtalar strapping and in-shoe lateral wedged insoles in women with knee osteoarthritis
Senem Güner & all
Medicina Sportiva
2161 The presences of any of the followings were taken as the exclusion criteria: inflammatory arthritis, peripheral or central nervous system disorders and previous knee or ankle surgery. After recording the demographic data of the subjects, Turkish versions of the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) (5-point Likert 3.0) were used for the evaluation of pain and physical function as described elsewhere (16). Isokinetic measurements were done by using Biodex System 3 (Biodex Medical Systems, Inc, New York, USA) dynamometer with the knee and ankle attachments. Orientation of the dynamometer was kept at 0°, tilt at 0°, and seat orientation at 0°. Patients were seated and secured to the apparatus with chest and thigh straps. The attachments of the dynamometer were adjusted so that the centre of motion of the lever arm was aligned as accurately as possible with the slightly changing flexion-extension axis of the joints. The range of motion was kept at 0-90° for the knee joint at 0-45° for the ankle joint. Bilateral isokinetic (concentric/concentric) knee flexion/extension at 60°/sec (five repetitions) and bilateral isokinetic (concentric/concentric) ankle plantar/dorsiflexion at 30°/sec (five repetitions) were performed. Patients had periods of rest between the sessions and vocal encouragement was standardized. Fifty-Foot Walk Test (FWS) was used to measure gait velocity and function (17). Participants were timed by chronometer as they walked 25 feet, turned around and walked back to the starting position at their preferred walking speed.
Sit-to-Stand Test (or chair rise, 5 repetitions) (STS) test was used to assess lower extremity strength and balance (18). Patients began by crossing their arms on their chest and sitting with their back against the chair (45 cm higher from the floor). The chair was armless and its back was supported against a wall. The same chair was used for all patients. The patients began while they were in the seated position and ended in the seated position. The patients were prompted not to bounce off the chair when returning to the standing position, and reminded to fully straighten their legs when elevating. They were instructed to stand up and sit down five times as quickly as possible (19). The mean score of the two trials (measured by a chronometer) were recorded for each subject with a rest between every two trials. After initial evaluations, the participants were randomized into three groups by an independent staff working in the department. The independent staff was blind to the study procedures and the treatment protocols. As follows: Group I (N=20, inserted-insole plus isometric exercises); Group II (N=20, strapped-insole plus isometric exercises); Group III (N=20, advised isometric exercises only). In Group I, shoes inserted insole was used (12mm). The participants in Group I used the two pairs of bilateral standardized laterally wedged (high density ethyl vinly acetate EVA) along the entire lateral border of foot (Figure 1) (20). The participants in Group II used a wedged with a strapped (12mm) which was designed to fit around their ankle and subtalar joints The wedges was produced with high density ethyl vinyl acetate (EVA) (Figure 2).
Figure 1. Bilateral standardized laterally wedged insole

Comparison of the effects of laterally wedged insole with subtalar strapping and in-shoe lateral wedged insoles in women with knee
osteoarthritis Senem Güner & all
Medicina Sportiva
2162
Figure 2. Laterally wedge with subtalar strapping
Participants were requested to perform quadriceps isometric knee exercises at home (twice a day, five days weekly, with an intensity 1-10 sub maximal contraction). Participants started wearing the insoles for 1 hour, thereafter increasing use by 1 hour per day until wearing them between 5 and 10 hour each day. The device was checked every 3 weeks and proper use of insole was confirmed by the wear. On the 8th week of treatment, subjects were reevaluated with WOMAC, isokinetic and physical performance tests. Before the study, the physical medicine and Rehabilitation specialist, who is one of the authors of this study, advised the participants to quit using any kind of analgesics. Statistical analysis of data was performed with the Statistical Program for Social Sciences for Windows version 16 (SPSS Inc., Chicago, Illinois, USA). Results were presented as mean±standard deviation (SD). Data were tested for normal distribution, and thereafter, comparisons between the groups were done by using One-Way Analysis of variance (ANOVA); Post-hoc Multiple Comparisons Bonferroni Correction. Paired Samples t-test was used to compare the baseline and final evaluations of the participants in each group. In addition, linear regression analysis has also been used to eliminate the factors related to the age. A probability (p) value of less than 0,05 was considered significant for all parameters. Results Demographics belonging to the groups are illustrated in Table I. variables such as weight, height, body mass index, and length of illnesses
showed statistically. Group I and II participants showed significant improvements in knee and ankle muscle strength in terms of flexion and extension muscle. In all three groups, the participants showed improvements after interventions (p<0.001; Table II). The Group III less improvements compared to the Group I and II. But no significant differences were found in participants of group III (p>0.05). As can be seen in Table II, the participants in Group I showed higher isokinetic test scores. These improvements were found especially in ankle muscles strength (dorsi flexion) (p<0.002). WOMAC scores of the three groups improved after interventions (Table III). When the three groups were compared using by ANOVA test and Bonferroni correction, a significant difference was found in pain subgroup of WOMAC. But Group I participants showed lower scores in terms of WOMAC. This shows that Group I participants had less pain (p<0.009). On the other hand, when we used linear regression analysis it was observed that there was no significant effect of age on WOMAC scores. The three group scores in terms of physical performance tests were also analyzed before and after the interventions. The three groups showed significant improvements in terms of the following two tests just used in this current work: 1) Fifth Foot Walk test; 2) Sit-to-Stand test (Table IV). When the three groups were compared, significant differences were found in terms of fifty foot walk test (p<0.007) and five sit-to-stand test scores (p<0.035). Moreover, participants in Group I had more improvements compared to the other groups.
Table I. Characteristics of the participants at baseline assessment VARIABLES GROUP I
Mean ± SD GROUP II Mean ± SD
GROUP III Mean ± SD
P*
Age (year) 53.55± 5.61 58.70±5.74 58.05±4.52 0.006 Height (cm) 160.03±5.03 160.01±3.94 158.40±4.73 0.351 Weight (kg) 75.90±1.01 77.60±7.08 75.40±7.03 0.682
Disease Duration (year) 4.45±2.96 5.00±2.63 5.45±2.64 0.520 *One-Way Analysis was used, SD: Standard deviation
Comparison of the effects of laterally wedged insole with subtalar strapping and in-shoe lateral wedged insoles in women with knee osteoarthritis
Senem Güner & all
Medicina Sportiva
2163
Table II. Isokinetic test results of the participants
MUSCLES GROUP I (n=20) GROUP II (n=20) GROUP III (n=20)
Baseline Mean±SD
8 weeks Mean±SD
P* Baseline Mean±SD
8 weeks Mean±SD
P* Baseline Mean±SD
8 weeks Mean±SD
P*
KNEE 60°/s Ext (R) 60°/s Ext (L) 60°/s Flex (R) 60°/s Flex (L)
66.09±22.5 68.51±25.9 44.90±15.6 47.78±15.1
86.08±29.6 87.51±27.7 57.94±19.1 59.87±16.6
.001 .001 .001 .001
59.79±21.5 61.27±18.6 46.08±16.3 44.20±12.6
77.65±19.6 77.15±21.1 57.12±17.4 55.11±13.2
.001 .001 .001 .001
76.62±21.9 72.18±20.8 58.85±15.6 51.56±13.5
75.08±25.2 75.08±22.1 58.72±13.4 58.72±11.7
.678 .278 .080 .015
ANKLE 45°/s P.Flex (R) 45°/s P.Flex (L) 45°/s D.Flex. (R) 45°/s D.Flex (L)
42.61±10.6 43.80±10.5 21.31±4.3 23.13±4.6
55.64±14.3 57.75±12.2 26.14±5.1 26.56±5.1
.001 .001 .002 .007
41.38±12.4 44.38±10.8 16.24±3.9 17.65±4.6
52.32±16.7 55.72±14.4 19.23±6.2 20.97±6.7
.001 .001 .001 .004
48.11±15.9 53.15±12.2 17.79±3.9 18.58±4.0
50.19±14.9 53.74±15.2 19.61±5.3 21.11±5.8
.231 .742 .099 .026
*Paired samples t Test was used, SD: Standard deviation
Table III. WOMAC test results of the participants (mean ± SD)
WOMAC GROUP I GROUP II GROUP III
Baseline 8 weeks P* Baseline 8 weeks P* Baseline 8 weeks P*
Pain 8.40±2.89 4.15±2.34 .001 9.10±2.44 4.75±1.88 .001 8.40±2,89 6.35±2.43 .231
Physical Function
37.70±7.08 23.20±5.61 .001 33.15±11.56 22.9±9.6 .001 27.55±10,87 24.85±10.69 .742
Total 43.75±10.3 29.0±7.60 .001 37.65±4.6 29,25±11.5 .001 37.75±13,34 32.95±13.056 .026 * Paired samples t-test was used
Table IV. Functional test results of the participants (mean ± SD)
Physical Performance Test
Fifty-Foot Walk Test Sit to Stand Test Baseline 8 weeks P* Baseline 8 weeks P*
Group I 26.0±2.14 23.31±2.36 0.001 11.70±2.02 9.90±1.33 0.001 Group II 28.04±3.62 25.40±2.82 0.001 12.67±2.97 11.24±2.05 0.001 Group III 27.5±3.08 25.81±2.17 0.012 11.87±1.50 11.11±1.30 0.002
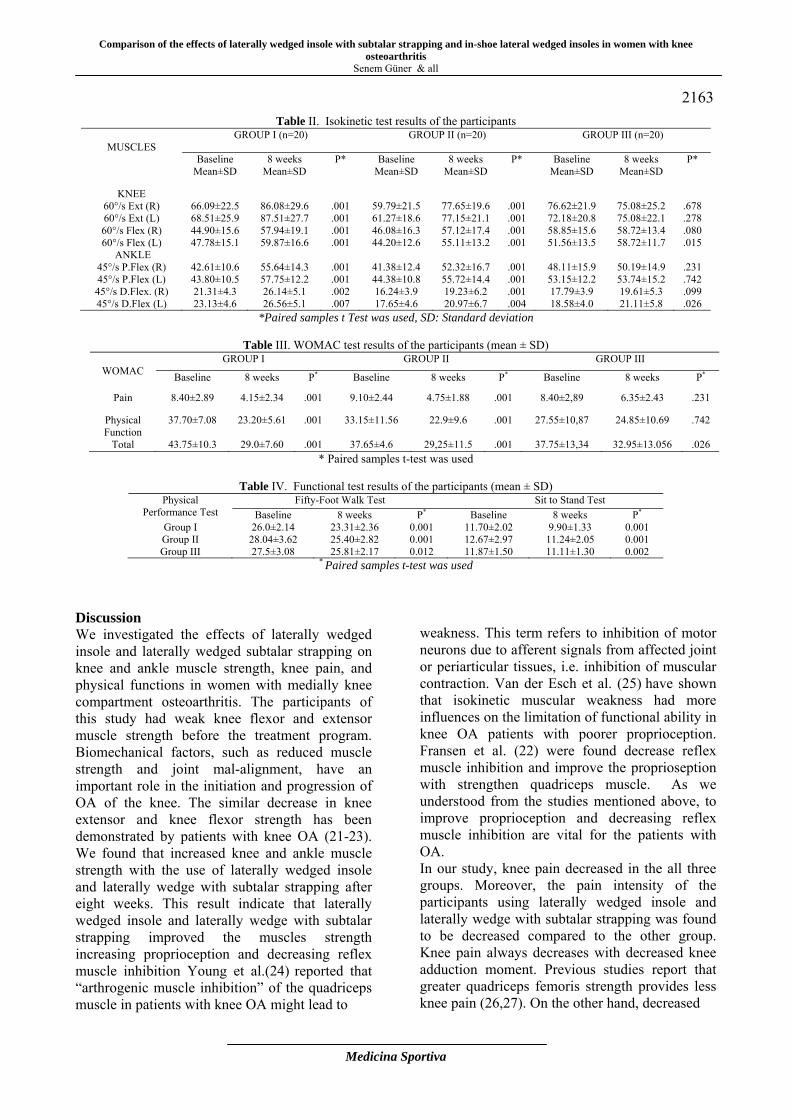
* Paired samples t-test was used Discussion We investigated the effects of laterally wedged insole and laterally wedged subtalar strapping on knee and ankle muscle strength, knee pain, and physical functions in women with medially knee compartment osteoarthritis. The participants of this study had weak knee flexor and extensor muscle strength before the treatment program. Biomechanical factors, such as reduced muscle strength and joint mal-alignment, have an important role in the initiation and progression of OA of the knee. The similar decrease in knee extensor and knee flexor strength has been demonstrated by patients with knee OA (21-23). We found that increased knee and ankle muscle strength with the use of laterally wedged insole and laterally wedge with subtalar strapping after eight weeks. This result indicate that laterally wedged insole and laterally wedge with subtalar strapping improved the muscles strength increasing proprioception and decreasing reflex muscle inhibition Young et al.(24) reported that “arthrogenic muscle inhibition” of the quadriceps muscle in patients with knee OA might lead to
weakness. This term refers to inhibition of motor neurons due to afferent signals from affected joint or periarticular tissues, i.e. inhibition of muscular contraction. Van der Esch et al. (25) have shown that isokinetic muscular weakness had more influences on the limitation of functional ability in knee OA patients with poorer proprioception. Fransen et al. (22) were found decrease reflex muscle inhibition and improve the proprioseption with strengthen quadriceps muscle. As we understood from the studies mentioned above, to improve proprioception and decreasing reflex muscle inhibition are vital for the patients with OA. In our study, knee pain decreased in the all three groups. Moreover, the pain intensity of the participants using laterally wedged insole and laterally wedge with subtalar strapping was found to be decreased compared to the other group. Knee pain always decreases with decreased knee adduction moment. Previous studies report that greater quadriceps femoris strength provides less knee pain (26,27). On the other hand, decreased
Comparison of the effects of laterally wedged insole with subtalar strapping and in-shoe lateral wedged insoles in women with knee
osteoarthritis Senem Güner & all
Medicina Sportiva
2164 pain leads to decreasing knee adduction moment (28). Moreover, many studies showed that footwear with laterally wedged insoles improved peak medially compartment load during gait cycle in both healthy and patients with OA (8, 9, 29-32). Physical performance of the participants just studied in this current work improved after the treatment programs. However, Group I and Group II participants showed greater improvement in terms of physical performance compared to the Group III. That means laterally wedged insole and laterally wedge with subtalar strapping improved physical functioning level increasing the knee and ankle muscles’ strength. Since the pain intensity of the participants in Group I and Group II decreased. They also showed an increased gait velocity. At the same time, Previous studies also reported that the same results in OA patients (27, 33). Related literature indicates that magnitude of the quadriceps femoris muscles strength is often associated with a faster walking speed (34). We also agree with previous studies. In addition to these results, we believe that the decreased pain intensity also led to increased walking speed in these patients. The results of this study and the related literature indicate that wearing a laterally wedged insole and laterally wedge with subtalar strapping have positive impact on pain intensity, muscle strength, and physical performance of the OA patients compared to conventional physiotherapy program. Moreover, these applications are inexpensive and non-invasive for regime of the knee OA. There were some limitations to the study as follows: no any long term follow up of the participants; no radiological results were collected. Further studies are needed to show the long term effects of these applications just used in the current work. Acknowledgement. The authors thank Prof. Osman Saracbası for statistical analysis. Declaration of conflicting interests. The authors declared no conflicts of interest with respect to authorship and/or publication of this article. Funding. The authors received financial support by Pamukkale University Scientific Research Projects Foundation (Grant no: 2008SBE007) for the research and/or authorship of this article.
References 1. Ahlback S (1968). Osteoarthritis of the knee: a
radiographic investigation. Acta Radiol., 277(Suppl.):70-72.
2. Duncan RC, Hay EM, Saklatvala J, Croft PR (2006). Prevalance of radiografic osteoarthritis: it all depends on your point of view. Rheumatology (Oxford); 45:757-760.
3. Schipplein OD, Andriacchi TP (1991). Interaction between active and passive knee stabilizers during level walking. J Orthop Res; 9:113 -119.
4. Gunduz H (2008). Osteoartritte Ağrı patogenezi. Türkiye Klinikleri Fiziksel Tıp ve Rehabilitasyon Dergisi Özel Sayısı; 1(2):28-32.
5. Jordan KM, Arden NK, Doherty M, Bannwarth B, Bijlsma JW, Dieppe P, et al, and Standing Committee for International Clinical Studies Including Therapeutic Trials (ESCISIT) (2003). EULAR recommendations 2003: An evidence based approach to the management of knee osteoarthritis: report of task force of the Standing Committee for International Clinical Studies Including Therapeutic Trials (ESCISIT). Ann Rheum Dis; 62(12):1145-1155.
6. American College of Rheumatology Subcommittee on Osteoarthritis Guidelines (2000). Recommendations for the medical management of osteoarthritis of the hip and knee: 2000 update. Arthritis Rheum; 43:1905-1915.
7. Sharma L, Song J, Felson DT, Cahu S, Shamiyeh E, Dunlop DD (2001). The role of knee alignment in disease progression and functional decline in knee osteoarthritis. JAMA; 286:188-195.
8. Yasuda K, Sasaki T (1987). The mechanics of treatment of the osteoarthritic knee with wedged insole. Clin Orthop; 215:162-172.
9. Kerrigan DC, Lelas JL, Goggins J, Merriman GJ (2002). Effectiveness of a lateral-wedged insole on knee varus torque in patients with knee osteoarthritis. Arch Phys Med Rehabil; 83:889-893.
10. Keating EM, Faris PM, Ritter MA, Kane J (1993). Use of lateral heel and sole wedges in the treatment of medial osteoarthritis of the knee. Orthop Rev; 22:921-926.
11. Van Raaij TM, Reijman M, Bierma-Zeinstra SM, Verhaar JA (2010). Medial knee osteoarthritis treated by insoles or braces. Clin Orthop Relat Re; 468(7): 1926-1932.
12. Toda Y, Tsukimura N, Kato A (2002). The effects of different elevations of laterally wedged insoles with subtalar strapping on medial compartment osteoarthritis of the knee. Arch Phys Med Rehabil; 83: 889-893.
13. Toda Y, Tsukimura N (2004). A six month follow-up of a randomized trial comparing the efficacy of a lateral wedged insole with subtalar strapping and an in-shoe lateral wedged insoles in
Comparison of the effects of laterally wedged insole with subtalar strapping and in-shoe lateral wedged insoles in women with knee osteoarthritis
Senem Güner & all
Medicina Sportiva
2165
patients with varus deformity osteoarthritis of the knee. Arthritis Rheum; 50: 3129-3136.
14. Toda Y, Tsukimura N, Segal N (2005). An optimal duration of daily wear for an insole with subtalar strapping in patients with varus deformity osteoarthritis of the knee. Osteoarthritis Cartilage; 13:353-360.
15. Altman R, Asch E, Bloch D, Brandth K, Borenstein D, Brandt K, et al (1986). Development of criteria for the classification and reporting of osteoarthritis: classification of osteoarthritis of the knee. Arthritis Rheum; 29: 1039-1049.
16. Tüzün EH, Eker L, Aytar A, Daşkapan A, Bayramoğlu M (2005). Acceptability, reliability, validity and responsiveness of the Turkish version of WOMAC osteoarthritis index. Osteoarthritis Cartilage; 13:28-33.
17. Grace EM, Gerecz EM, Kaassam YB, Buchanan HM, Buchanan WW, Tugwell PS (1988). 50-foot walking time: a critical assessment of an outcome measure in clinical therapeutic trials of antirheumatic drugs. Br J Rheumatol; 27: 372-374.
18. Lord SR, Murray SM, Chapman K, Munro B, Tiedemann A (2002). Sit-to-stand performance depends on sensation, speed, balance, and psychological status in addition to strength in older people. J Gerontol A Biol Sci Med Sci; 57(8): 539-543.
19. Holzberg AD, Robinson ME, Geisser ME, Gremillion HA (1996). The effects of depression and chronic pain on psychosocial and physical functioning. Clin J Pain., 12:118-125.
20. Toda Y, Segal N (2002). Usefulness of an insole with subtalar strapping for analgesia in patients with medial compartment osteoarthritis of the knee. Arthritis Rheum; 47: 468-473.
21. Alencar MA, Arantes PMM, Dias JMD, Kirkwood RN, Pereira LSM, Dias RC (2007). Muscular Function and Functional Mobility of Faller and Non-Faller Elderly Women with Osteoarthritis of the Knee. Brazilian Journal of Medical and Biological Research; 40(2): 277-283.
22. Fransen M, McConell S, Bell M (2003). Exercise for osteoarthritis of the hip or knee. Cochrane Database Syst Rev; 3: 28-41.
23. O’Reilly SC, Jones A, Muir KR, Doherty M (2003). Quadriceps weakness in knee osteoarthritis: the effect on pain and disability. Ann Rheum Dis; 57: 588–594.
24. Young A (1993). Current issues in arthrogenous inhibition. Ann Rheum Dis; 52: 829-834.
25. Van der Esch M, Steultjens M, Harlaar J, Knol D, Lems W, Dekker J (2007). Joint proprioception, muscle strength, and functional ability in patients with osteoarthritis of the knee. Arthritis Rheum; 57: 787-793.
26. Kemp G, Crossley KM, Wrigley TV, Metcalf BR, Hinman RS (2008). Reducing joint loading in
medial knee osteoarthritis: shoes and canes. Arthritis Rheum; 59: 609-614.
27. Raja K, Dewan N (2011). Efficacy of knee braces and foot orthoses in conservative management of knee osteoarthritis: a systematic review. Am J Phys Med Rehabil; 90(3): 247-262.
28. Mundermann A, Dyrby CO, Hurwitz DE, Sharma L, Andriacchi TP (2004). Potential strategies to reduce medial compartment loading in patients with knee osteoarthritis of varying severity: reduced walking speed. Arthritis Rheum; 50: 1172-1178.
29. Fisher DS, Dyrby CO, Mündermann A, Morag E, Andriacchi TP (2007). In healthy subjects without knee osteoarthritis, the peak knee adduction moment influences the acute effects of shoe interventions designed to reduce medial compartment knee load. J Orthop Res; 25: 540-546.
30. Kakihana W, Akai M, Nakazawa K, Naito K, Torii S (2007). Inconsistent knee varus moment reduction caused by a lateral wedge in knee osteoarthritis. Am J Phys Med Rehabil; 86: 446-454.
31. Shimada S, Kobayashi S, Wada M, Uchida K, Sasaki S, Kawahara H, et al (2006). Effect of disease severity on response to lateral wedged shoe insole for medial compartment knee osteoarthritis. Arch Phys Med Rehabil; 87: 1436-1441.
32. Kuroyanagi Y, Nagura T, Matsumoto H, Otani T, Suda Y, Nakamura T et al (2007). The lateral wedged insole with subtalar strapping significantly reduces dynamic knee load in the medial compartment-gait-analysis on patients with medial knee osteoarthritis. Osteoarthritis Cartilage; 15: 932-6.
33. Rubin R, Menz HB (2005). Use of laterally wedged custom foot orthosis to reduce pain associated with medial knee osteoarthritis: a preliminary investigation. J Am Podiart Med Assoc; 95: 47-52.
34. Fang MA, Taylor CE, Nouvong A, Masih S, Kao KC, Perell KL (2006). Effects of footwear on medial compartment knee osteoarthritis. J Rehabil Res Dev; 43: 427-434.
Corresponding author Prof. Dr. Uğur Cavlak Pamukkale University, School of Physical Therapy and Rehabilitation, Denizli, Turkey. E-mail: [email protected] Phone: 02582962301
Received: June 12, 2013 Accepted: August 20, 2013

Medicina Sportiva (2013), vol. IX, no 3, 2166-2170 Romanian Sports Medicine Society
Salivary antioxidant enzymes in young exercised women Erfani Karimzadeh Toosi A1, Rezaei A2, Sariri Kh R3 1Gastrointestinal and Liver Disease Research Center, Guilan University of Medical Sciences, Rasht, Iran 2Department of Periodontology, Faculty of Dentistry, Tehran University of Medical Sciences, Tehran, Iran 3 Department of Microbiology, Lahijen Branch, Islamic Azad University, Lahijan, Iran Abstract. Introduction. Saliva is the first body fluid to encounter different solids, fluids and gases entering the gastrointestinal tract. Human saliva is composed of various natural antioxidants including enzymatic and non-enzymatic systems. Free radicals are naturally produced species with an unpaired electron, i.e. reactive towards biological molecules. Production of these reactive species is affected by different factors including metabolic and various external events. An important consequence of aerobic exercise is related to increased antioxidant capacity of human body. In the present research, antioxidant enzymes in salivary fluid of young girls were investigated after aerobic exercise. Material and Method. A volunteer group of 35 healthy female university students (mean age 25.1±1.5 years) entered the study. They were told to attend a one month course of aerobic training. Three samples of their saliva were obtained at the beginning of research, after two weeks and at the end of exercise period. The activity of three antioxidant enzymes, catalase, superoxide dismutase and peroxidase were assayed in supernatant of their centrifuged saliva samples. Results. A significant increase in the activity of three antioxidant enzymes was observed. Conclusions. The increase in oxidative free radicals induced by exercise is compensated by higher activity of antioxidant enzymes of saliva. Therefore, enzymatic activity is salivary fluid could be a marker of oxidative status of saliva due to production of free radicals. Aerobic exercise for a month stimulates the activity of antioxidant enzymes in favor of radical scavenging ability. Key words: saliva, aerobic exercise, catalase, peroxidase, superoxide dismutase. Introduction Human saliva possesses a complex mixture of various biochemicals, similar in many aspects to other body fluids (1). It is one of the most important body fluids secreted primarily by three paired major salivary glands and secondarily by hundreds of minor salivary glands located below the mucosal surfaces of the mouth (2). Salivary fluid is a rich mixture of substances that makes saliva a possible source for identifying unique biomarkers that reflect oral as well as metabolic, genetic and systemic diseases (3, 4). It is believed that various exercises could be beneficial to human body through various mechanisms. A regular type of exercise can reduce the risk of many diseases including diabetes, cancer and cardiovascular disorders. However, there are some evidences on increasing the reactive oxygen (and/or nitrogen) species during intense exercise (5). It has been stated that an intense exercise increases the body’s oxygen demand to about 15-20 times the normal value (6). Reactive oxygen
species (ROS) could cause oxidative stress and increase the rate of oxidation. Natural antioxidants present in various body sites, could reduce the oxidative damage through absorption of ROS (5-7). Moderate exercise decreases possible risk of various infections through increasing body resistance (8, 9). However, athletes undergoing chronic high intensity training are in risk of upper respiratory tract infection (10). It is suggested that rise of infection in athletes could be related to a decrease in salivary immunoglobulin-A (11). Considering that saliva consists of important antioxidants and its sampling is non-invasive, the aim of this research was assessment of salivary antioxidant enzymes after a period of aerobic exercise. Materials and methods Materials. Analytical grade chemicals and solvents were purchased from local representatives and used as provided by manufacturers, no purification was needed. Superoxide dismutase kit was purchased from
2166
Salivary antioxidant enzymes in young exercised women Erfani Karimzadeh Toosi A & all
Medicina Sportiva
2167 R&D Systems Europe, Ltd, Catalog number:7500-100-K. 4-Amino antipyrine, phenol, hydrogen peroxide, horseradish peroxidase were purchased from Merck chemical company. The EnzyChromTM Catalase Assay Kit (ECAT-100) was purchased from a local provider. The necessary solutions and buffers were prepared freshly using double distilled water. All general chemicals, solvents and reagents were obtained with highest purity available. Subjects. Thirty five female university students aged 22-25 years volunteered to enter our research. The measured characteristics of subjects are reported in Table I. They were recommended to attend a one month aerobic course that was formally approved by ministries of health and exercise and a registered instructor trained them. Those with internal or genetic diseases as well as volunteers having oral, teeth and gums disorders were excluded. The aim of study was explained to all and a form about their health history was filled and signed by each. Collection of saliva samples. Un-stimulated saliva samples were obtained after fasting for 8 hours. The subjects rinsed their mouth once with distilled water, kept their saliva for 5 minutes and poured into a dry calibrated sterile tube (12).
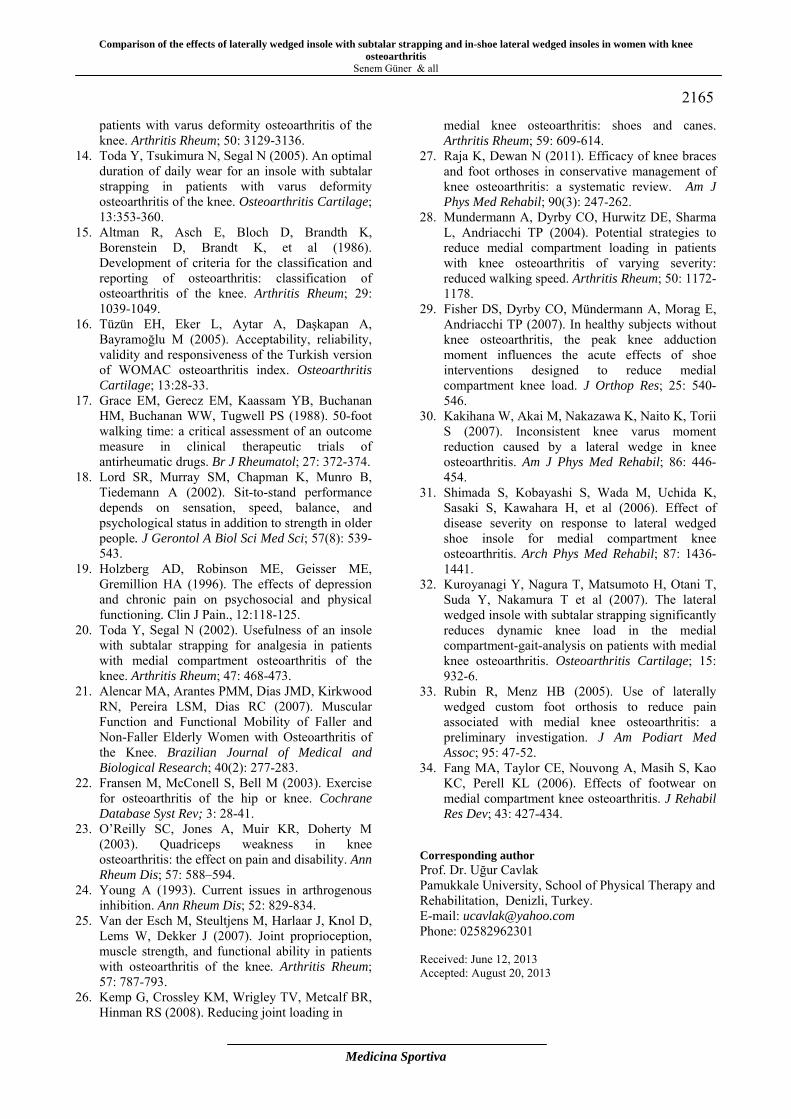
The volume of samples was measured and the flow rate calculated in ml/min. The samples were immediately centrifuged at 800 × g for 10 min at 4°C to remove squamous cells and cell debris. The resulting supernatant was stored at -70°C until assays of enzyme activity. Three saliva samples were obtained from each participant, i.e. before, after two and after four weeks training aerobic exercise. Assay of superoxide dismutase (SOD). A special kit designed to assay superoxide dismutase activity for research purposes was used. According to the recommended assay procedure, oxidation of xanthine by xanthine oxidase (XOD) generates uric acid and hydrogen peroxide. Superoxide radical anions (O2
•−), also produced in this reaction, reduce a tetrazolium salt (nitroblue tetrazolium, NBT) to colored formazan product (NBT-diformazan) which absorbs light at 550 nm. The percent inhibition of NBT reduction is a measure of the activity of SOD in the sample (Figure 1). One unit of SOD inhibits the rate of increase in absorbance at 550 nm by 50% under assay conditions. It is worth indicating that, in biological environment, the hydrogen peroxide (H2O2) produced in the SOD reaction can be removed by peroxidase or catalase, the other two antioxidant enzymes (Figure 2).
Table I. Main characteristic of volunteered female subjects Age (years) Mass (kg) Height (m) Body fat % Mean: 22.35 SD: 2.16 Range: 35-40
61.12 6.33 51.7-70.21
1.63 0.15 1.52-1.70
15.25 3.22 14.2-17.33
Figure 1. The superoxide radical anions produced by XOD reaction reduce nitroblue Tetrazolium
(NBT) to colored NBT-diformazan that absorbs light at 550 nm. Scavenging of superoxide radical anions by SOD can reduce the rate of dye formation.

Salivary antioxidant enzymes in young exercised women
Erfani Karimzadeh Toosi A & all
Medicina Sportiva
2168
Figure 2. The reactions catalysed by the antioxidant enzymes assayed in the present research
Assay of superoxide dismutase (SOD). A special kit designed to assay superoxide dismutase activity for research purposes was used. According to the recommended assay procedure, oxidation of xanthine by xanthine oxidase (XOD) generates uric acid and hydrogen peroxide. Superoxide radical anions (O2
•−), also produced in this reaction, reduce a tetrazolium salt (nitroblue tetrazolium, NBT) to colored formazan product (NBT-diformazan) which absorbs light at 550 nm. The percent inhibition of NBT reduction is a measure of the activity of SOD in the sample (Figure 1). One unit of SOD inhibits the rate of increase in absorbance at 550 nm by 50% under assay conditions. Assay of catalase. The assay kit was used as provided by the manufacturer’s representative and the activity of catalase in saliva samples was measured using the recommended procedure. This is a kit designed for direct assay of catalase in biological fluids including serum, saliva and urine. In principle, degradation of H2O2 by catalase was followed using a redox dye. The change in color intensity was measured spectrophotometrically at 570 nm. This was proportional to activity of catalase in saliva. As recommended by kit manufacturer, one unit of catalase activity (U/ml) is amount of catalase that decomposes 1 mole of H2O2 per min at pH 7.0 and ambient temperature. Statistical analysis. All experiments were preformed three times and the results presented as mean ± SD values. Any statistically significant difference between individuals was compared using un-paired t-test. P values less than 0.05 were considered statistically significant. Results and discussions Measurement of flow rate. The flow rate of un-stimulated saliva was calculated as the volume of samples obtained in one minute and gathered in Table II. Significant variations in the flow rate in all subjects were observed after exercise.
According to the results, the flow rate of saliva increased from 0.9-1.80 ml min-1 before training to 1.1-2.0 ml.min-1 after one month aerobic exercise (p<0.05). According to literature, the flow rate of biological fluids including tears (14) and saliva depends on many factors (15). For example, it has been reported that the salivary flow rate does not significantly alter due to exercise intensity (12), but decreases sharply in smokers (16) and those suffering from peptic ulcer (17). An increase in vegetarian's salivary volume and flow rate has also been reported in response to vegetarian diet (18). However, the positive effect of aerobic exercise on flow rate of saliva, observed in this study, is one of many advantages of this type of exercise, especially for older individuals who suffer from dry mouth. Superoxide dismutase activity. In Table III, the biological activity of superoxide dismutase in saliva samples of volunteers before, in the middle and after their aerobic exercise course is compared. It can be seen that activity of this enzyme has significantly increased in saliva samples of almost all volunteers after aerobic exercise compared to before training. The increased activity of antioxidant enzymes, including SOD, during aerobic exercise is the natural biological response for deactivation of excess free radicals. In support of our result, an interesting research has also reported increased SOD activity among children playing computer games (19). Peroxidase activity. Table III also shows peroxidase activity in salivary fluid of subjects. Peroxidase is one of important antioxidant enzymes in human saliva (16). A significant increase in peroxidase activity was observed after two weeks aerobic exercise which was continued to increase during the next two weeks. The enzyme scavenges free radicals produced during natural methabolic processes in the body environment. In the oral cavity, peroxidase not only protects the local environment, it also inhibits their entrance to the internal
Salivary antioxidant enzymes in young exercised women Erfani Karimzadeh Toosi A & all
Medicina Sportiva
2169 gastrointestinal environment (12). The significant increase of its activity observed after exercise is highly beneficial to both oral cavity and the whole gastrointestinal tract in terms of protection against ROS and RNS. This finding is in close agreement with the results reported for high intensity exercise in athelets (12, 13) and non athelets (20). However, various external factors could alter the activity of salivary peroxidase in different manners. For example, entirely different from our results, it has been reported that a vegetarian diet has caused a significant reduction in salivary POD (18). On the other hand, alternations on salivary defense system due to metabolic diseases such as diabetes (21), in response to smoking (16) and peptic ulcers (17) have also supported our results.
Catalase activity. The activity of catalase in saliva samples before, during and after one month aerobics exercise is presented in Table III. It can be seen that the activity of this enzyme is also increased in subjects undergoing aerobic exercise training. Although catalase has not been extensively studied in saliva according to our literature survey, the activity of this enzyme is also important in scavenging free radicals and enhancing the salivary defense system. In support of the present study, the higher activity of catalse has also been observed in high intensity exercise (12). It is suggested that enhanced activity of this enzymes is beneficial for improving oral and internal health status.
Table II. Flow rate of saliva before and after training course. Each value is the mean of 70 measurements (35 cases each duplicate)
Flow rate (ml/mim) Beginning of study After two weeks After four weeks
Mean Range (SD)
1.22 0.9-1.8 0.62
1.28 1.0-1.7 0.78
1.36 1.1-2.0 0.85
Table III. Biological activity of the three antioxidant enzymes in saliva samples of subjects before,
during and after a course of aerobic exercise Sample SOD activity
(U/ml) POD activity
(U/ml) Catalase activity (U/ml)
P values*
Beginning of the study After two weeks training After four weeks training
0.95 ± 0.24 1.05 ± 0.25 1.25 ± 0.33
0.004 ± 0.006 0.010 ± 0.01 0.035 ± 0.025
0.004 ± 0.003 0.005 ± 0.008 0.007 ± 0.005
0.03 0.04 0.04
Values presented as Mean ± SD. P values less than 0.05 were considered statistically significant. Conclusions Natural antioxidants present in healthy saliva are responsible for diminishing the activity of free radicals and, therefore, protect oral cavity. Eventually, internal body environment can be less damaged by normal action of the antioxidant system in the salivary fluid. In this study, activity of three antioxidant enzymes of saliva samples was compared before, two and four weeks after a course of aerobic exercise under supervision of a specialized trainer. The quantitative data from enzymatic antioxidant studies indicated a significant and gradual increase in antioxidant power of saliva in response to aerobic exercise. According to the results obtained from the present study, increase of antioxidant enzyme activity in oral fluid could be the result of regular aerobic exercise. Therefore, it is concluded that a continued and long lasting exercise as a health
strategy could gradually rise the ability of saliva as a barrier to free radicals. This could not only protect the oral cavity, especially teeth and gums, but also provides a safe barrier for substances entering the body by oral pathway. Last not least, performing aerobic exercise is highly effective in improving health status of both oral cavity and gastrointestinal tract by inhibition of free radical attack. Acknowledgements. Our sincere thanks to student volunteers for donation of saliva samples. References 1. Bardow A, Madsen J, Nauntofte B (2000). The
bicarbonate concentration in human saliva does not exceed plasma level. Clinical Oral Investigation; 4: 245-253.
2. Herrera JL, Lyons IIMF Johnson LF (1998). Saliva: its role in health and disease. Journal of Clinical Gastroenterology; 10: 569-578.
Salivary antioxidant enzymes in young exercised women
Erfani Karimzadeh Toosi A & all
Medicina Sportiva
2170 3. Novak MJ, Potter RM, Blodgett J Ebersole JL
(2008). Periodontal disease in Hispanic Americans with type 2 diabetes. Journal of Periodontology; 79: 629-636.
4. Aizenbud D, Peri-Front Y, Nagler RM (2008). Salivary analysis and antioxidants in cleft lip and palate children. Archieves of Oral Biology; 53: 517-522.
5. Clarkson PM, Thompson HS (2000). Antioxidants: what role do they play in physical activity and health? Am J Cli Nutr; 72: 637-646.
6. Carlsohn A, Rohan S, Bittmann F, Railamayer F (2008). Exercise Increases the Plasma Antioxidant Capacity of Adolescent Athletes. Ann Nutr Metab; 53: 96-103.
7. Bailey DM, Lawrenson L, McEneny J, Young IS, James PE, Jackson SK, Henry RR, Mathieu-Costello O, McCord JM, Richardson R (2007). Electron paramagnetic spectroscopic evidence of exercise-induced free radical accumulation in human skeletal muscle. Free Rad Res; 41: 182-190.
8. Pretz W. Running from infection (1984). Running World; 19: 78-79.
9. Algrove JE, Gomes E, Hough J, Gleeson M (2008). Effects of exercise intensity on salivary antimicrobial proteins and markers of stress in active men. J Sport Sci; 26: 653-661.
10. Peters EM, Bateman ED (1983). Ultramarathon running and upper respiratory tract infections. S Afr Med J; 64: 582-584.
11. Tra GP, Barnes M (1990). Reduction of immunoglobulin-A by swim training. Eur J Appl Physiol; 60: 61-64.
12. Damirchi A, Kiani M, Jafarian V, Sariri R (2010). Response of salivary peroxidase to exercise intensity. Eur J Appl Physiol; 108: 1233-1237.
13. Sariri R, Damirchi A, Nazari Y (2013). Salivary antioxidant variations in athletes after intense exercise. Romanian Sports Medicine Society Medicina Sportiva; IX(1): 2043- 2050.
14. Emina MO (2010). Aging and topical pilocarpine concentrations effects on pupil size and tear flow rate. Journal of Optometry; 3(2): 102-106.
15. Inoue H, Ono K, Masuda W, Morimoto Y, Tanaka T, Yokota M, Inenaga K (2006). Gender difference in unstimulated whole saliva flow rate and salivary gland sizes. Archives of Oral Biology; 51(12): 1055-1060.
16. Sariri R, Varasteh A, Erfani A, Rezaei A, Heidari Z (2010). Inhibition of salivary peroxidase by cigarette smoke. Health; 2: 347-351.
17. Motamedi M, Mansour Ghanaei F, Sariri R, Vesal M (2013). Salivary enzymes in peptic ulcer disease. J Oral Biol Craniofacial Res; http://dx.doi.org/10.1016/j.jobcr.2013.03.004.
18. Amirmozafari N, Pourghafar H, Sariri R (2013). Salivary defense system alters in vegetarian. J Oral Biol Craniofacial Res; http://dx.doi.org/10.1016/j.jobcr.2013.05.004.
19. Imge B, Ergoder, llker Durak (2006). Effects of computer use on human salivary oxidant/antioxidant status. J Biol Sci; 6: 14-17.
20. Nazari Y, Damirchi A, Sariri R and Taheri M (2012). Response of salivary antioxidants to intense exercise in non-athlete men. J Exerc Physiologyonline; 15(3): 1-9.
21. Willis AM, Coulter WA, Fulton CR, Hayes JR, Bell PM, Lamey PJ (1999). Oral candidal carriage and infection in insulin-treated diabetic patients. Diabetes Medicine; 16: 675-679.
Corresponding author Erfani Karimzadeh Toosi A Gastrointestinal and Liver Disease Research Center, Guilan University of Medical Sciences, Rasht, Iran E-mail: [email protected] Fax: 00981313233647 Received: June 28, 2013 Accepted: August 26, 2013

Medicina Sportiva (2013), vol. IX, no 3, 2171-2176 Romanian Sports Medicine Society
Heritability in women and men of muscle strength of upper and lower limbs Elys Costa de Sousa, Michelle Vasconcelos de Oliveira, Fabiana Tenório, Vanessa Carla Monteiro Pinto, Luciano Alonso Valente dos Santos, Paulo Moreira Silva Dantas Universidade Federal do Rio Grande do Norte, Brasil
Abstract. This study aimed to analyze the heritability in women and men muscle strength of upper and lower limbs in a broad age range. The sample included 88 twins, 8 and 36 years of age, which were 56 monozygotic (MZ) divided between 28 women and 28 men and 32 dizigotics (DZ) divided between 18 women and 14 men, all of them residents of metropolitan area of Natal in Rio Grande do Norte - Brazil. The test of explosive strength lower limbs was performed by vertical jump. The upper limb strength was measured during maximal voluntary isometric contraction of elbow flexion of 90°. Data were evaluated in non-parametric statistics, analyzed based on the variance of the intrapair twins. Applied the equation of heritability (h²) = ((S²DZ – S²MZ)/S²DZ) x 100, demonstrating how each variable has genotypic and phenotypic character. The confidence interval (25% - 75%) was calculated from the medians found. For women explosive strength in lower limbs was h²= 85% (77% -97%) and h²= 68% (53% -75%) for men. For females isometric strength in upper limbs was h² = 39% (35%-46%) and for male, h²= 73% (53% -77%). It was demonstrated for women a high h² for lower limbs strength and a low moderate h² in upper limbs strength; for men, a high moderate h² for both lower limbs strength as superior limbs strength. As for age range, although extensive, it did not influence the results. Key words: heredity, twins, isometric exercise, genotype, phenotype. Introduction The focus on heritability (h²) motor skills through studies with pairs of twins has been discussed. The contribution from the genotype in determining the phenotype (Method of twin) instigates the proposition that the twins are a sample of the general population and the components of each pair of twins are exposed to the same environmental influences (1). These possible genetic and environmental influences should be considered for human performance. Isometric strength and muscle power tend to present higher heritability (2). In this way, it can be affirmed that the strength and muscle power are multifactorial phenotypes, with the result of the interaction between environment and genetic effects. Some people can be more prone to low muscle strength in various muscle groups due to genetics and other people environmental effects (3). The relative contributions of the environmental effects and genetics to variability of muscle strength may change over time. According to observations made by Carmelli and Reed (4), the estimated value of handgrip strength decreased during 10 years of monitoring of 35 to 22%, whereas the shared environmental effects
increased from 39 to 45% in male twins average age of 63 years. The application of criteria to identify the contributions of genotypic and environmental factors in the individual and collective characteristics is crucial for us to understand how the individual reaches different levels of physical performance. From the foregoing, this study aims to examine the heritability in women and men muscle strength of lower and upper limbs in a wide age range. Material and Method There were participants in the study pairs of monozygotic and dizigotics twins, residents of metropolitan area of Natal in Rio Grande do Norte - Brazil, during the years 2011 and 2012. To achieve the objectives of this study, the sample was composed of 88 twins between 08-36 years, 56 being monozygotic (MZ) divided between 28 women and 28 men, and 32 dizigotics (DZ) divided between 18 women and 14 men. In the search for understanding the action of time on the scale of results of heritability, our study opted for a broad age range, in order to observe how the variability of the ages of the twin pairs
2171

Heritability in women and men of muscle strength of upper and lower limbs
Elys Costa de Sousa & all
Medicina Sportiva
2172 could induce the results. We believe that a large variability of age can interfere with the amplitude of the results of h2, and the smaller intervals of age range, responsible for reducing the chance of large amplitude. However, we opted for the fact that extreme values are offset by its correlates in the opposite end. And for the greater security of our findings we use the confidence interval (CI) between 25% and 75% in an attempt to eliminate this trend to higher amplitude. The first moment of data collection was the selection of pairs of twins in a non-probabilistic intentional and signature of the Informed Consent Form for participants over 18 years, and for the younger, the term was by their parents or guardians. After signature the consent form, applied with twins or parents of children under 18 years of age, medical history of the participants was analyzed, and also their state of health and lifestyle habits regarding physical activity. They answered a physical activity questionnaire PAR-Q to analyze the readiness to physical activities. The zigosity was determined by administrating a questionnaire of zigosity to the mothers of the twins by phone, validated by Peeters (5), which can only be answered by the mothers of each pair. It was performed an observation of similarity in physical characteristics between the pair of twins (skin color, eye and heir color, hair type, shape of nose, mouth and teeth, height and body mass) (1). The study excluded individuals with physical disabilities that prevented assessments of muscle strength, pregnant women, individuals in drug treatment related to obesity and patients with endogenous obesity or secondary (Down syndrome, Prader Willi syndrome, hypo- thyroidism, etc..). There were also excluded from the study pairs of twins of different sex, the pairs that did not share the same environment and same habits of physical activity and the pairs with difference in pubertal stage. When looking for differences in anthropometric intrapair variables by height and body mass greater than 5 cm or greater than 5 kg, respectively, the pair was excluded from the sample, with the intention of increase reliability of
the results. Similarly, for self-assessment (6) of pubertal stage was set as the cutoff for deletion of a pair of twins, the difference staging. For this, was measured twice: first after the preliminary interviews and the second after the physical assessments. Thus, it was possible to calculate the weighted kappa index between repeated measures of self-assessment of pubertal stage separately for individuals monozygotic (MZ) and dizigotics (DZ), in which values were greater than 0.890 with p <0.001. If there was a difference intrapair twin to the outcome of pubertal stage, this pair would be removed from the analysis. The present study was approved by the Ethics Committee of the Hospital Onofre Lopes – CEP/HUOL duly recognized by the National Research Ethics under protocol CEP/HUOL: 484/10, according to the guidelines of Resolution CNS 196 / 96 and the Treaty of Helsinki, 1975. Explosive strength (Figure 1). The test of the strength of the lower limbs was performed by the Counter Movement Jump to Contact Carpet CEFISE ®. The results were analyzed by Jump System software, version 1.0. The results used were obtained in W/kg. Prior to application of the test, the twins were instructed to make a general warming up lasting 5 minutes with static stretching of quadriceps and hamstrings for 15 seconds for each movement. Measurements were performed with a twin at a time. The individual performed four jumps with maximum strength, obeying the interval of 60 seconds between them. Twin positioned on the carpet in the upright position (position 1), and when received authorization from the evaluator performed the jump squat thrust up to 90 degrees of knee joint (position 2). Hands stayed fixed at the hip, in the region of the iliac crest, and the feet were positioned parallel and hip-width apart. From this position, the individual performed a vertical jump as high as possible while keeping the verticality of the trunk and legs extended in the air (position 3). In damping the fall (position 4), the twins could bend knees, but during the flight, should keep them extended. If there was flexion of the knees before the authorization of the evaluator, the jump was considered invalid, having the need to repeat the sequence of jumps (7). The value used was the largest of four jumps.
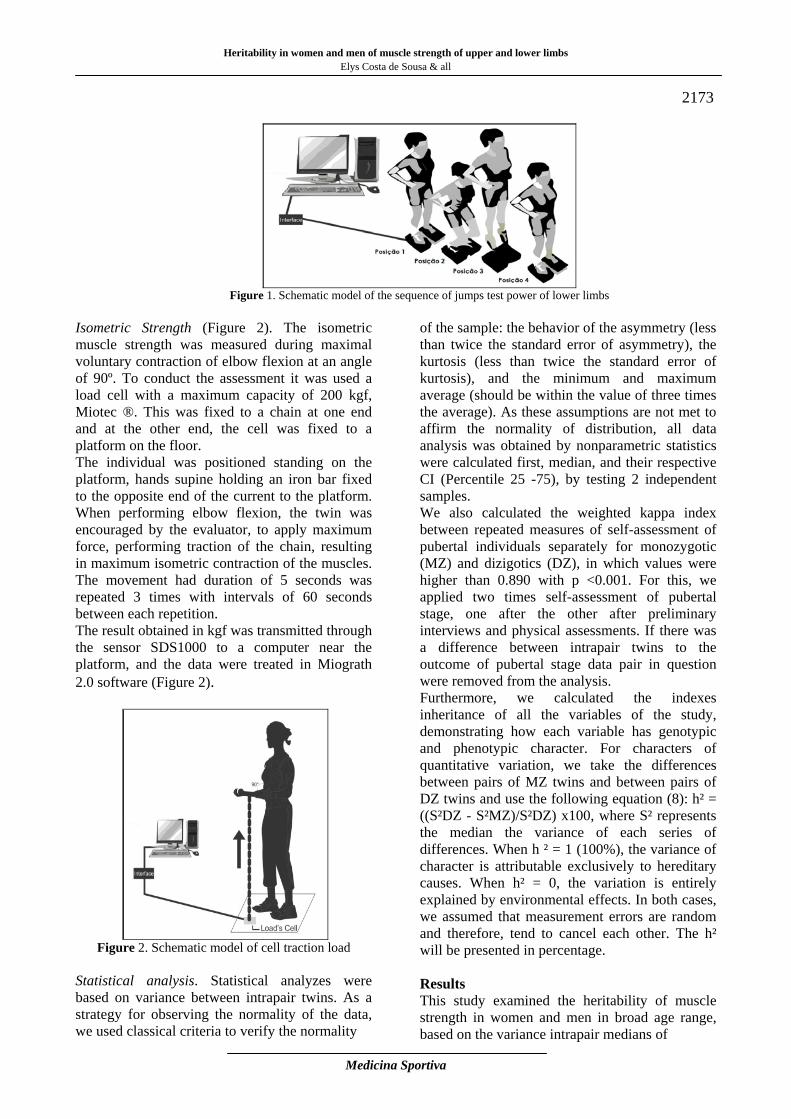
Heritability in women and men of muscle strength of upper and lower limbs Elys Costa de Sousa & all
Medicina Sportiva
2173
Figure 1. Schematic model of the sequence of jumps test power of lower limbs
Isometric Strength (Figure 2). The isometric muscle strength was measured during maximal voluntary contraction of elbow flexion at an angle of 90º. To conduct the assessment it was used a load cell with a maximum capacity of 200 kgf, Miotec ®. This was fixed to a chain at one end and at the other end, the cell was fixed to a platform on the floor. The individual was positioned standing on the platform, hands supine holding an iron bar fixed to the opposite end of the current to the platform. When performing elbow flexion, the twin was encouraged by the evaluator, to apply maximum force, performing traction of the chain, resulting in maximum isometric contraction of the muscles. The movement had duration of 5 seconds was repeated 3 times with intervals of 60 seconds between each repetition. The result obtained in kgf was transmitted through the sensor SDS1000 to a computer near the platform, and the data were treated in Miograth 2.0 software (Figure 2).
Figure 2. Schematic model of cell traction load
Statistical analysis. Statistical analyzes were based on variance between intrapair twins. As a strategy for observing the normality of the data, we used classical criteria to verify the normality
of the sample: the behavior of the asymmetry (less than twice the standard error of asymmetry), the kurtosis (less than twice the standard error of kurtosis), and the minimum and maximum average (should be within the value of three times the average). As these assumptions are not met to affirm the normality of distribution, all data analysis was obtained by nonparametric statistics were calculated first, median, and their respective CI (Percentile 25 -75), by testing 2 independent samples. We also calculated the weighted kappa index between repeated measures of self-assessment of pubertal individuals separately for monozygotic (MZ) and dizigotics (DZ), in which values were higher than 0.890 with p <0.001. For this, we applied two times self-assessment of pubertal stage, one after the other after preliminary interviews and physical assessments. If there was a difference between intrapair twins to the outcome of pubertal stage data pair in question were removed from the analysis. Furthermore, we calculated the indexes inheritance of all the variables of the study, demonstrating how each variable has genotypic and phenotypic character. For characters of quantitative variation, we take the differences between pairs of MZ twins and between pairs of DZ twins and use the following equation (8): h² = ((S²DZ - S²MZ)/S²DZ) x100, where S² represents the median the variance of each series of differences. When h ² = 1 (100%), the variance of character is attributable exclusively to hereditary causes. When h² = 0, the variation is entirely explained by environmental effects. In both cases, we assumed that measurement errors are random and therefore, tend to cancel each other. The h² will be presented in percentage. Results This study examined the heritability of muscle strength in women and men in broad age range, based on the variance intrapair medians of
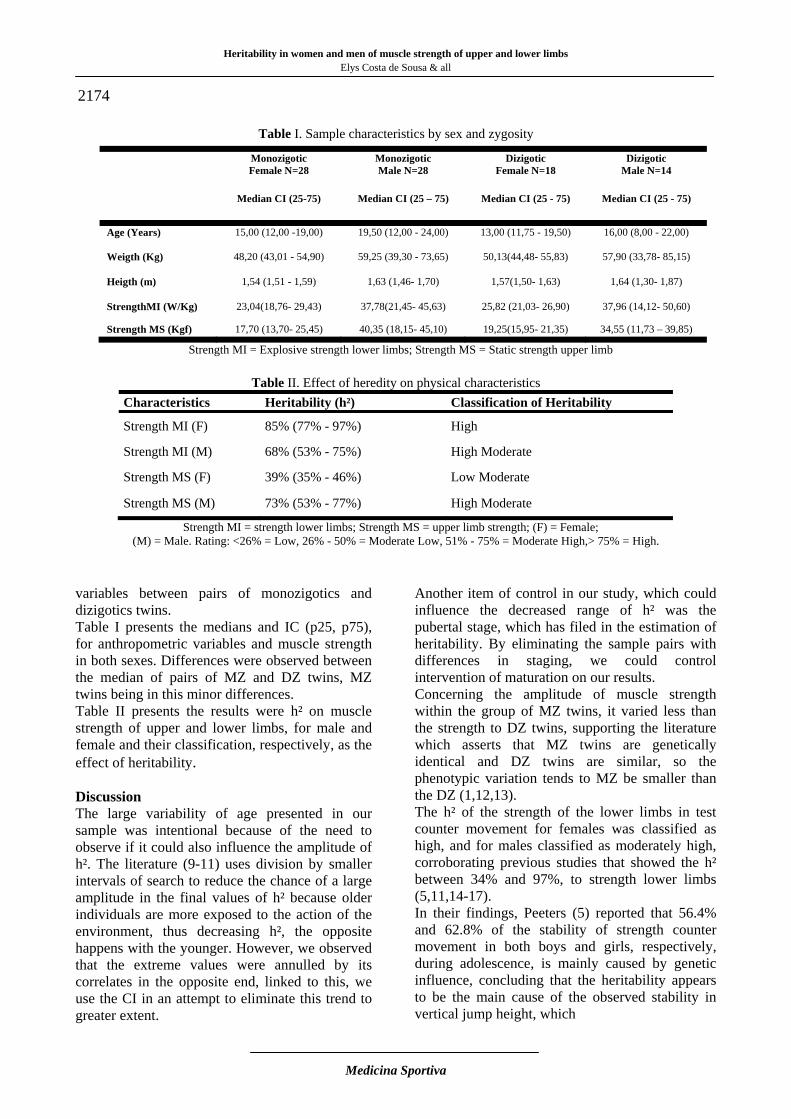
Heritability in women and men of muscle strength of upper and lower limbs
Elys Costa de Sousa & all
Medicina Sportiva
2174
Table I. Sample characteristics by sex and zygosity
Strength MI = Explosive strength lower limbs; Strength MS = Static strength upper limb
Table II. Effect of heredity on physical characteristics Characteristics Heritability (h²) Classification of Heritability
Strength MI (F) 85% (77% - 97%) High
Strength MI (M) 68% (53% - 75%) High Moderate
Strength MS (F) 39% (35% - 46%) Low Moderate
Strength MS (M) 73% (53% - 77%) High Moderate
Strength MI = strength lower limbs; Strength MS = upper limb strength; (F) = Female; (M) = Male. Rating: <26% = Low, 26% - 50% = Moderate Low, 51% - 75% = Moderate High,> 75% = High.
variables between pairs of monozigotics and dizigotics twins. Table I presents the medians and IC (p25, p75), for anthropometric variables and muscle strength in both sexes. Differences were observed between the median of pairs of MZ and DZ twins, MZ twins being in this minor differences. Table II presents the results were h² on muscle strength of upper and lower limbs, for male and female and their classification, respectively, as the effect of heritability. Discussion The large variability of age presented in our sample was intentional because of the need to observe if it could also influence the amplitude of h². The literature (9-11) uses division by smaller intervals of search to reduce the chance of a large amplitude in the final values of h² because older individuals are more exposed to the action of the environment, thus decreasing h², the opposite happens with the younger. However, we observed that the extreme values were annulled by its correlates in the opposite end, linked to this, we use the CI in an attempt to eliminate this trend to greater extent.
Another item of control in our study, which could influence the decreased range of h² was the pubertal stage, which has filed in the estimation of heritability. By eliminating the sample pairs with differences in staging, we could control intervention of maturation on our results. Concerning the amplitude of muscle strength within the group of MZ twins, it varied less than the strength to DZ twins, supporting the literature which asserts that MZ twins are genetically identical and DZ twins are similar, so the phenotypic variation tends to MZ be smaller than the DZ (1,12,13). The h² of the strength of the lower limbs in test counter movement for females was classified as high, and for males classified as moderately high, corroborating previous studies that showed the h² between 34% and 97%, to strength lower limbs (5,11,14-17). In their findings, Peeters (5) reported that 56.4% and 62.8% of the stability of strength counter movement in both boys and girls, respectively, during adolescence, is mainly caused by genetic influence, concluding that the heritability appears to be the main cause of the observed stability in vertical jump height, which
Monozigotic Female N=28
Monozigotic Male N=28
Dizigotic Female N=18
Dizigotic Male N=14
Median CI (25-75) Median CI (25 – 75) Median CI (25 - 75) Median CI (25 - 75)
Age (Years) 15,00 (12,00 -19,00) 19,50 (12,00 - 24,00) 13,00 (11,75 - 19,50) 16,00 (8,00 - 22,00)
Weigth (Kg) 48,20 (43,01 - 54,90) 59,25 (39,30 - 73,65) 50,13(44,48- 55,83) 57,90 (33,78- 85,15)
Heigth (m) 1,54 (1,51 - 1,59) 1,63 (1,46- 1,70) 1,57(1,50- 1,63) 1,64 (1,30- 1,87)
StrengthMI (W/Kg) 23,04(18,76- 29,43) 37,78(21,45- 45,63) 25,82 (21,03- 26,90) 37,96 (14,12- 50,60)
Strength MS (Kgf) 17,70 (13,70- 25,45) 40,35 (18,15- 45,10) 19,25(15,95- 21,35) 34,55 (11,73 – 39,85)
Heritability in women and men of muscle strength of upper and lower limbs Elys Costa de Sousa & all
Medicina Sportiva
2175 confirms our results, in which the contribution was greater than the inherited environment for this feature, corroborating Lemmer et al (18) indicated that alterations in strength of lower limbs between men and women after a training program of 24 weeks and were similar and significant alterations in the level of strength of both women and men, highlighting the influence of environmental 15% female and 32% male. It was found in this study that the muscle strength of the lower limbs has a character genotypic very strong, so it provides a margin of trainability very small, especially for females, that is the choice of an athlete for a particular sport that requires this feature must be made with extreme caution, since the possibility of environmental interference (strength training) is smaller. For example, not all women who have great facility to increase the muscle mass of the lower limbs and this has an important link with the characteristic bone length and in turn has to do with family characteristics (19). The results for the h² muscle strength of the upper limbs reflect moderate genotypic contribution for both women and men, with low moderate to female and moderate high to male (Table 2). These estimates are confirmed in the literature, where studies with small samples, heritability ranges between 14% and 83%, which characterizes this variable from low contribution of genotype to high heritability. Also corroborating our findings, Tainen (3) asserts that the genetic influence on muscle strength behaves moderate, this way, the variability of upper limb strength ranges between 22% and 52%. By identify in this study, the genetic factor is less significant in women, the phenotypic factor can be developed more effectively, confirming the study conducted with men and women (20) to analyze alterations in upper limb strength after 16 weeks of training. In all exercises, women had a higher percentage of change in strength when compared to men, thus characterizing environmental adaptation higher in females. Thus, the contribution identified in genotypic results found in this study is affirmed. A systematic analysis of isometric strength in adulthood and sexual differences, showed that among danish twins there were sex differences in the relative contribution of genes and environment, with a heritability of 52% (21). In the upper limb strength, the greater the possibility of interference from the environment is found in females, although this is not the segment
more trained for this population, because it is an area that contrasts to secondary sexual characteristics and acts directly on aesthetics female body (22). But, for males, the h² upper limb is moderately high, which reduces the range of the gain strength through training. However, despite the values for males to females excel, it is clear the role of training (environmental influence), the result of male interest in gaining strength and muscle mass in the trunk and upper limbs (22). Thus, gender differences in adherence to strength training are not always clear, but the genotype appears to perform in determining muscle strength a prominent role in men than in women (23). Conclusion The greatest h² in women of the strength of the lower limbs indicates that intervention strategies physical training should observe important hereditary contributions. For men, this contribution was somewhat lower, indicating greater action of the environment, which may also influence the strategies of training. Although, regarding the upper limb strength in the female lower contribution of h² indicates that the changes arising from physical training could be more tonics. In men, there was a balance of h² between upper and lower limbs, thus indicating strategies very close physical training considering the action of heredity. It was evident in this study, although the age range is extensive, to consider the proposed confidence interval, the possible effects of this magnitude were minimized. References
1. Beiguelman B. (1994). Dinâmica dos genes nas famílias e nas populações: Sociedade Brasileira de Genética.
2. Beunen, G., & Thomis, M. (2000). Muscular strength development in children and adolescents. Pediatric Exercise Science; 12: 174-197.
3. Tiainen K., Sipilä S, Alen M, Heikkinen E, Kaprio J, Koskenvuo M, et al. (2004). Heritability of maximal isometric muscle strength in older female twins. Journal of Applied Physiology; 96(1): 173-180.
4. Jack L M, Reed T, Guralnik J M (2000). The contribution of genetic influences to measures of lower-extremity function in older male twins. Journal of Gerontology; 55(1): B49-B53.
5. Peeters M W, Thomis M A, Maes H H M, Loos R J F, Claessens A ., Vlietinck R, et al. (2005). Genetic and environmental causes of tracking in explosive strength during adolescence. Behavior
Heritability in women and men of muscle strength of upper and lower limbs
Elys Costa de Sousa & all
Medicina Sportiva
2176
Genetics; 35(5): 551-563. doi: DOI 10.1007/s10519-005-5417-z
6. Matsudo S M M, Matsudo V K. R (1991). Validade da auto-avaliação na determinação da maturação sexual. Revista Brasleira de Ciência e Movimento; 5(2): 17.
7. Rafael M A, Del Olmo M F, González OV, Jodar X A, Pérez F J V (2008). DSJ (vertical jump without counter-movement from bending the knees over 120º) and the 30m sprint from the rest. Fitness & Performance Journal; 7(5):319-25.
8. Clark P J (1956). The heritability of certain anthropometric characters as ascertained from measurements of twins. American Journal of Human Genetics; 8(1): 49.
9. Komi P V, Viitasalo J T, Rauramaa R, Vihko V (1978). Effect of Isometric Strength Training on Mechanical, Electrical, and Metabolic Aspects of Muscle Function. European Journal of Applied Physiology and Occupational Physiology; 40(1): 45-55. doi: Doi 10.1007/Bf00420988
10. Missitzi J, Geladas N, Klissouras V (2007). Genetic variation of maximal velocity and EMG activity. International Journal of Sports Medicine, 29(03); 177-181.
11. Chatterjee S, Das N (1995). Physical and Motor Fitness in Twins. Japanese Journal of Physiology; 45(3): 519-534.
12. Beiguelman B, Franchi-Pinto C, Krieger H, Magna L.A (1996). Twinning rate in a southeastern Brazilian population. Acta Genet Med Gemellol (Roma); 45(3): 317-324.
13. Beiguelman B (2008). O estudo de gêmeos. Ribeirão Preto: SBG.
14. Thomis M A I, Beunen G P, Van Leemputte M, Maes H H, Blimkie C J, Claessens A L, et al. (1998). Inheritance of static and dynamic arm strength and some of its determinants. Acta Physiologica Scandinavica; 163(1): 59-71.
15. Maes H H M, Beunen G P, Vlietinck R F, Neale M C, Thomis M, VandenEynde B, et al. (1996). Inheritance of physical fitness in 10-yr-old twins and their parents. Medicine and Science in Sports and Exercise; 28(12): 1479-1491.
16. Beunen G, Thomis M, Peeters M, Maes H, Claessens A, Vlietinck R (2003). Genetics of strength and power characteristics in children and adolescents. Pediatric Exercise Science; 15(2): 128-138.
17. Okuda E, Horii D, Kano T (2005). Genetic and environmental effects on physical fitness and motor performance. International Journal of Sport and Health Science; 3(0): 1-9.
18. Lemmer J T, Ivey F M, Ryan A S, Martel G F, Hurlbut D E, Metter J E, et al. (2001). Effect of strength training on resting metabolic rate and physical activity: age and gender comparisons.
Medicine and Science in Sports and Exercise; 33(4): 532-541.
19. Reis V M, Machado J V, Fortes M S, Fernandes P R, Silva A J, Dantas P S, et al. (2007). Evidence for higher heritability of somatotype compared to body mass index in female twins. J Physiol Anthropol; 26(1): 9-14. doi: JST.JSTAGE/jpa2/26.9 [pii]
20. Cureton K J, Collins M A, Hill D W, McElhannon F (1988). Muscle hypertrophy in men and women. Medicine and Science in Sports and Exercise; 20(4): 338-344.
21. Frederiksen H, Christensen K. (2003). The influence of genetic factors on physical functioning and exercise in second half of life. Scandinavian Journal of Medicine and Science in Sports; 13(1): 9-18.
22. Estevão A, Bagrichevsky M (2009). Cultura da “corpolatria” e body-building: notas para reflexão. Revista Mackenzie de Educação Física e Esporte, 3(3).
23. Beunen G, Thomis M (2006). Gene driven power athletes? Genetic variation in muscular strength and power. British Journal of Sports Medicine; 40(10): 822-823.
Corresponding author Elys Costa de Sousa Universidade Federal do Rio Grande do Norte, Brasil Postal address: Rua Praça Deodoro, 19ª- Tirol- Natal/RN – Brazil. CEP 59014-520 E-mail: [email protected] Phone: +55 84 8812-0572 Received: May 16, 2013 Accepted: July 23, 2013

Medicina Sportiva (2013), vol. IX, no 3, 2171-2184 Romanian Sports Medicine Society
Work related musculoskeletal disorders among administrators in a Nigerian university Ojoawo Adesola O1, Oni Michael1, Popoola O2
1Department of Medical Rehabilitation, Faculty of Basic Medical Sciences, Obafemi Awolowo University, Ile Ife. Nigeria 2Department of Public Administration, Faculty of Administration, Obafemi Awolowo University, Ile Ife. Nigeria Abstract. The aim of this study was to carry out a survey of musculoskeletal disorders (MSKDS) and its effect on daily activities of administrators in a Nigerian university. Material and Method. Seventy eight (41 males and 37 females) administrators participated in this study. Respondent were selected by purposive sampling at different section of administrative department such as senate, division of student affairs, faculty offices and the university library. Modified questionnaire on pattern of musculoskeletal pain and injury among bankers was adopted for the study. Data were analyzed using descriptive and inferential statistics. Results. Result shows that low back pain (48.5%) was the most common complaint among administrators, followed by bilateral knee (13.6%) and right hand (10.6%). These were followed by head pain (7.6%), left hand pain (7.6%), neck pain 6.1%), and pain in the interior body (6.1%). It was found that most of the causes of musculoskeletal injury were due to poor knowledge of practicing techniques (66.7%) and inadequate space (69.6%). In addition, prolonged sitting (59.1%) is a major predisposing factor to MSKDS while other activity such as driving (1.5%), lifting (4.5%), standing (7.6%) and walking (9.1%) contributed the least among the causes of MSKDS. There was a significant association between nature of MSKDS and rate of recurrence but there was no significant association between MSKDS and years of experience. Conclusion. It could be concluded from the study that the most prevalent musculoskeletal pain among administrator is low back pain due to prolong sitting but this does not affect the activities in office and the longer the pain the more tendency for its reoccurrence. Key words: low back pain, neck pain, administrators, punctuality, musculoskeletal. Introduction Musculoskeletal disorders are a global problem affecting human endeavor gulping a lot of money as compensation in many developed countries (1). It is a leading cause of long –term disability, with substantial impact on quality of life and use of health resources. In the United States of America, the overall cost of MSKDS was estimated to be about 214.9 billion U.S Dollars and the direct cost of managing MSKDS that was –related amounted to 88.7 billion U.S Dollars of which 38% was spent on hospital admission and 21% on nursing care (2). In the United Kingdom, 13% -44% of workers were reported to suffer MSKDS and about 11.6 million working days were reported to lost to MSKDS in 2004 and 2005 (3,4). Musculoskeletal disorders (MSKDS) represent a significant occupational problem among nurses; however, data on musculoskeletal health of nurses in Sub-Sahara Africa are sparse (5). The results of their work show that 84.5% of the nurses have had work-related musculoskeletal disorders once
or more in their occupational lives. Work-related musculoskeletal disorder occurred most is low back pain (44.1%), neck pain (28.0%) and knees pain (22.4%). Thirty point three percent treated themselves or had visited other health practitioners for care. Nurses greater than 20 years of clinical experience are about 4 times more likely to develop work-related musculoskeletal disorders than those with 11-20 years of experience. Working in the same position for long periods (55.1%), lifting or transferring dependent patients (50.8%) and treating an excessive number of patients in one day (44.9%) were the most perceived job risk factors for musculoskeletal disorders. Musculoskeletal disorder can be disabling and leads to economic loss. Most people experience pain at the back, neck, and shoulder at the same time, although few have pain over a long period of time (6). Administrators are present in various ministries, parastatals and agencies.
2177

Work related musculoskeletal disorders among administrators in a Nigerian university
Ojoawo Adesola O & all
Medicina Sportiva
2178 They are well noted for their technocracy, professionalism, expertise, skill, experience and competence. Besides, many administrators have, over the years, accumulated enormous administrative, professional and managerial experience, they have become a powerful force to reckon with in all governmental activities and bureaucratic processes. It is believed that no modern society could manage the daily operation of its public affairs without the administrators (7). The use of desktops computer or a laptop which are modern office with the sitting position could be a predisposing factor to MSKDS. According to a study by Adedoyin et al (8), the most frequent complaints of pain by computer users are low back pain, neck pain, and wrist pain while foot and knee pain are the least reported when using computer system. These complaints are more severe in people with more than four years working experience on computer (9). Silberstein,(10) reported repetitious movement, awkward postures and high force levels as the three primary risk factors that have been associated with work-related musculoskeletal disorders. Effective performance of a university administrator is very important. It is one of the key factors to a successful day to day running of the University, especially Obafemi Awolowo University. The patterns of occupational musculoskeletal injuries among health professional and nurses have been documented (5). The survey of MSKDS and its effect on the functional activities of administrators in Obafemi Awolowo University is not yet known Material and Method Seventy eight administrators working at Obafemi Awolowo University were purposively selected to participate in this study. They were apparently healthy individuals that have been performing administrative duties for a minimum of six months. Exclusion from the study was pregnant women and individual with previous history of accident involving musculoskeletal system. Respondents were selected from different sections of the administrative offices in the University.
A copy of questionnaire was administered to each participant, the questionnaire was collected the same day it was administered. Instrument. Modified questionnaire by Aguda (11) on pattern of musculoskeletal disorder and injury among bankers was adopted for the study. The questionnaire consists of three sections: – Section A contains question on biodata of the
respondents such as sex, age, departmental sections, marital status, period of working hours, years of experience, academic qualification, and administrative cadre.
– Section B consists of etiology and incidence of pain, some of the questions inquired on duration of pain, nature of the pain and activity that aggravated the pain. Included in this section is location of pain and 10 point pain rating scale. The effect of pain on daily activities of respondents was also evaluated in this section.
– Section C entails etiology and incidence of injury. It enquired whether participants have had injury during the course of employment and how often. The causes of injury was also examined which may be instrument related, skill related, space or man power related.
Ethical Approval. Consent of each participant was obtained and there was ethical approval for the study from Research Committee of Institute of Public Health, OAU Ile Ife. Data Analysis. Data were analyzed using descriptive and inferential statistics. Inferential statistics of chi-square was used to examine the association between MSKDS and punctuality in office. Also chi square test of association was used to examine if there is any association between nature of pain and recurrence Results Table I shows the percentage distribution of respondents by their socio-demographic characteristics. According to the table, forty one respondents (52.6%) were male while others (47.4%) were females. More than thirty five percent (35.9%) were within age group 40-49 years, 27 respondents (34.6%) were within age group 50-60 years. Twenty eight respondents (35.9%) had spent at least 21 years at work and 17 respondents (21.8%) had between 1-5 years working experience.
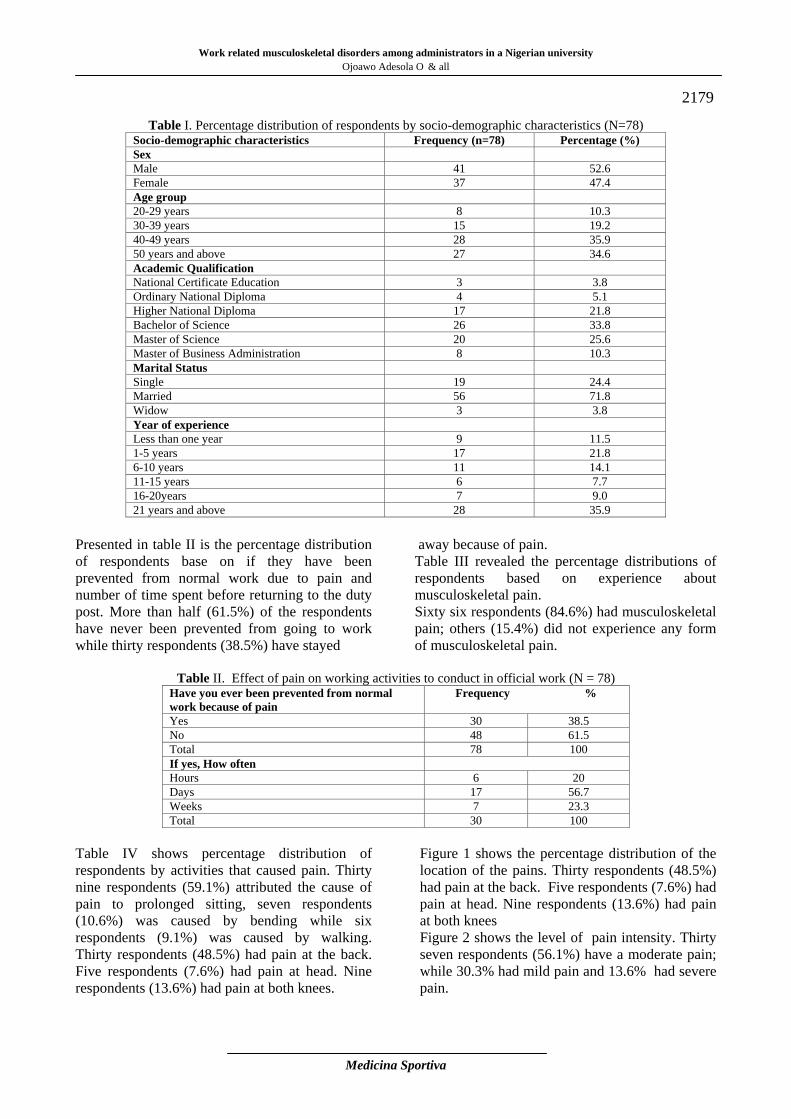
Work related musculoskeletal disorders among administrators in a Nigerian university Ojoawo Adesola O & all
Medicina Sportiva
2179
Table I. Percentage distribution of respondents by socio-demographic characteristics (N=78) Socio-demographic characteristics Frequency (n=78) Percentage (%) Sex Male 41 52.6 Female 37 47.4 Age group 20-29 years 8 10.3 30-39 years 15 19.2 40-49 years 28 35.9 50 years and above 27 34.6 Academic Qualification National Certificate Education 3 3.8 Ordinary National Diploma 4 5.1 Higher National Diploma 17 21.8 Bachelor of Science 26 33.8 Master of Science 20 25.6 Master of Business Administration 8 10.3 Marital Status Single 19 24.4 Married 56 71.8 Widow 3 3.8 Year of experience Less than one year 9 11.5 1-5 years 17 21.8 6-10 years 11 14.1 11-15 years 6 7.7 16-20years 7 9.0 21 years and above 28 35.9
Presented in table II is the percentage distribution of respondents base on if they have been prevented from normal work due to pain and number of time spent before returning to the duty post. More than half (61.5%) of the respondents have never been prevented from going to work while thirty respondents (38.5%) have stayed
away because of pain. Table III revealed the percentage distributions of respondents based on experience about musculoskeletal pain. Sixty six respondents (84.6%) had musculoskeletal pain; others (15.4%) did not experience any form of musculoskeletal pain.
Table II. Effect of pain on working activities to conduct in official work (N = 78) Have you ever been prevented from normal work because of pain
Frequency %
Yes 30 38.5 No 48 61.5 Total 78 100 If yes, How often Hours 6 20 Days 17 56.7 Weeks 7 23.3 Total 30 100
Table IV shows percentage distribution of respondents by activities that caused pain. Thirty nine respondents (59.1%) attributed the cause of pain to prolonged sitting, seven respondents (10.6%) was caused by bending while six respondents (9.1%) was caused by walking. Thirty respondents (48.5%) had pain at the back. Five respondents (7.6%) had pain at head. Nine respondents (13.6%) had pain at both knees.
Figure 1 shows the percentage distribution of the location of the pains. Thirty respondents (48.5%) had pain at the back. Five respondents (7.6%) had pain at head. Nine respondents (13.6%) had pain at both knees Figure 2 shows the level of pain intensity. Thirty seven respondents (56.1%) have a moderate pain; while 30.3% had mild pain and 13.6% had severe pain.
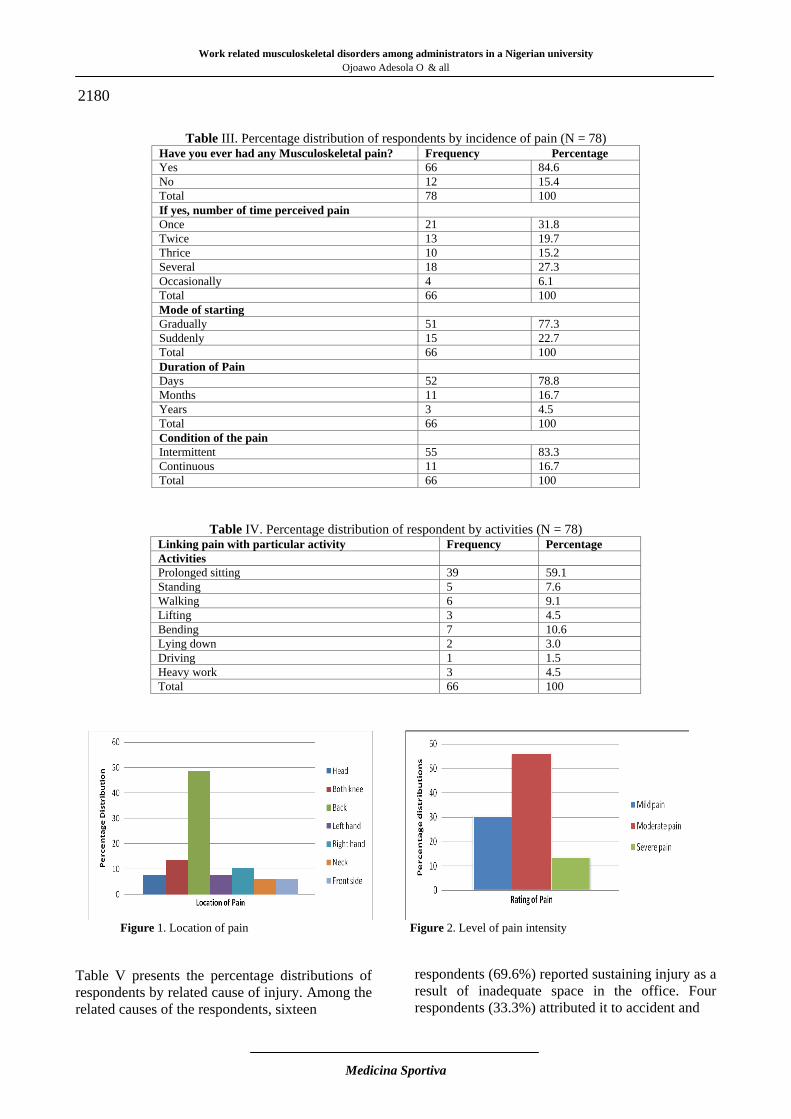
Work related musculoskeletal disorders among administrators in a Nigerian university
Ojoawo Adesola O & all
Medicina Sportiva
2180
Table III. Percentage distribution of respondents by incidence of pain (N = 78) Have you ever had any Musculoskeletal pain? Frequency Percentage Yes 66 84.6 No 12 15.4 Total 78 100 If yes, number of time perceived pain Once 21 31.8 Twice 13 19.7 Thrice 10 15.2 Several 18 27.3 Occasionally 4 6.1 Total 66 100 Mode of starting Gradually 51 77.3 Suddenly 15 22.7 Total 66 100 Duration of Pain Days 52 78.8 Months 11 16.7 Years 3 4.5 Total 66 100 Condition of the pain Intermittent 55 83.3 Continuous 11 16.7 Total 66 100
Table IV. Percentage distribution of respondent by activities (N = 78) Linking pain with particular activity Frequency Percentage Activities Prolonged sitting 39 59.1 Standing 5 7.6 Walking 6 9.1 Lifting 3 4.5 Bending 7 10.6 Lying down 2 3.0 Driving 1 1.5 Heavy work 3 4.5 Total 66 100
Figure 1. Location of pain Figure 2. Level of pain intensity Table V presents the percentage distributions of respondents by related cause of injury. Among the related causes of the respondents, sixteen
respondents (69.6%) reported sustaining injury as a result of inadequate space in the office. Four respondents (33.3%) attributed it to accident and
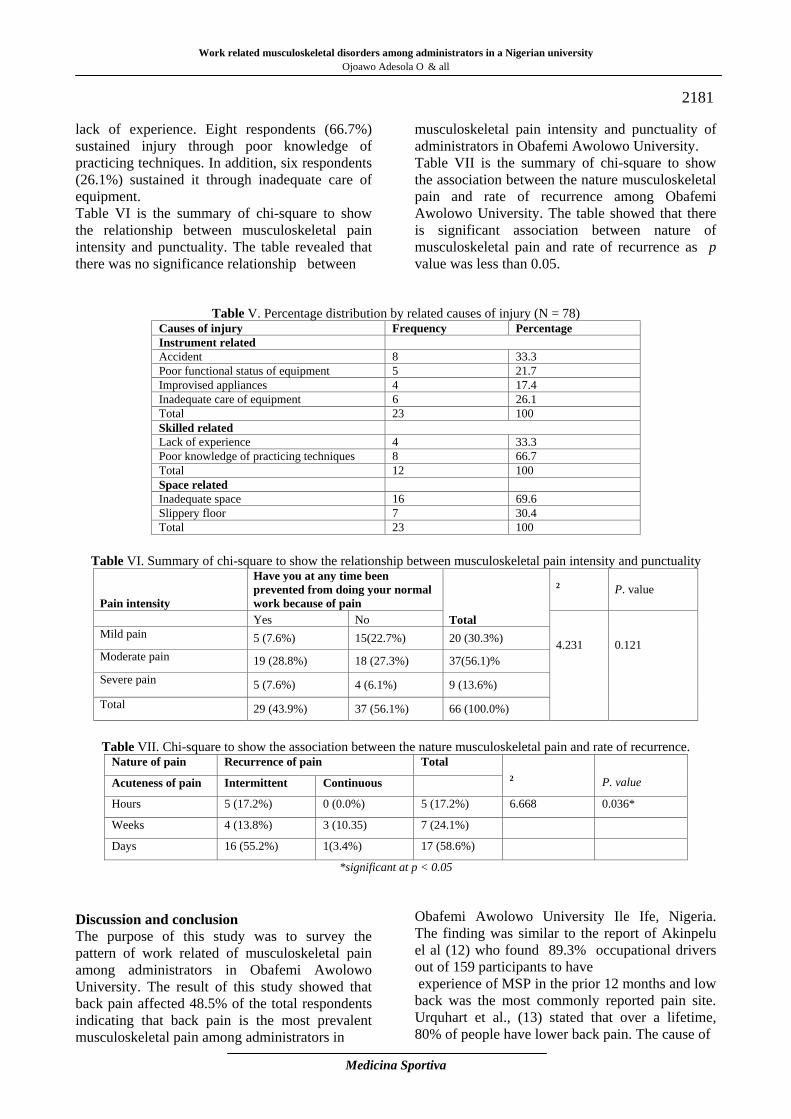
Work related musculoskeletal disorders among administrators in a Nigerian university Ojoawo Adesola O & all
Medicina Sportiva
2181 lack of experience. Eight respondents (66.7%) sustained injury through poor knowledge of practicing techniques. In addition, six respondents (26.1%) sustained it through inadequate care of equipment. Table VI is the summary of chi-square to show the relationship between musculoskeletal pain intensity and punctuality. The table revealed that there was no significance relationship between
musculoskeletal pain intensity and punctuality of administrators in Obafemi Awolowo University. Table VII is the summary of chi-square to show the association between the nature musculoskeletal pain and rate of recurrence among Obafemi Awolowo University. The table showed that there is significant association between nature of musculoskeletal pain and rate of recurrence as p value was less than 0.05.
Table V. Percentage distribution by related causes of injury (N = 78)
Causes of injury Frequency Percentage Instrument related Accident 8 33.3 Poor functional status of equipment 5 21.7 Improvised appliances 4 17.4 Inadequate care of equipment 6 26.1 Total 23 100 Skilled related Lack of experience 4 33.3 Poor knowledge of practicing techniques 8 66.7 Total 12 100 Space related Inadequate space 16 69.6 Slippery floor 7 30.4 Total 23 100
Table VI. Summary of chi-square to show the relationship between musculoskeletal pain intensity and punctuality
Pain intensity
Have you at any time been prevented from doing your normal work because of pain
Total
2
P. value
Yes No 4.231
0.121
Mild pain 5 (7.6%) 15(22.7%) 20 (30.3%) Moderate pain 19 (28.8%) 18 (27.3%) 37(56.1)% Severe pain 5 (7.6%) 4 (6.1%) 9 (13.6%) Total 29 (43.9%) 37 (56.1%) 66 (100.0%)
Table VII. Chi-square to show the association between the nature musculoskeletal pain and rate of recurrence.
Nature of pain Recurrence of pain Total 2
P. value Acuteness of pain Intermittent Continuous
Hours 5 (17.2%) 0 (0.0%) 5 (17.2%) 6.668 0.036*
Weeks 4 (13.8%) 3 (10.35) 7 (24.1%)
Days 16 (55.2%) 1(3.4%) 17 (58.6%)
*significant at p < 0.05 Discussion and conclusion The purpose of this study was to survey the pattern of work related of musculoskeletal pain among administrators in Obafemi Awolowo University. The result of this study showed that back pain affected 48.5% of the total respondents indicating that back pain is the most prevalent musculoskeletal pain among administrators in
Obafemi Awolowo University Ile Ife, Nigeria. The finding was similar to the report of Akinpelu el al (12) who found 89.3% occupational drivers out of 159 participants to have experience of MSP in the prior 12 months and low back was the most commonly reported pain site. Urquhart et al., (13) stated that over a lifetime, 80% of people have lower back pain. The cause of

Work related musculoskeletal disorders among administrators in a Nigerian university
Ojoawo Adesola O & all
Medicina Sportiva
2182 pain at low back with this occupation might be attributed to prolong sitting, especially in meetings and offices which is a usual characteristic of an administrator. Prolong sitting have been known to have effect on the low back due to unnecessary stress on the spine which when occurs repeatedly can cause micro-trauma to the spine (14). Prolonged sitting in bad position leads to slackening of the abdominal muscles and curvature of the spine. In sitting, the lumbar lordosis tends to flatten and the pelvis rotates posterior. This kyphotic posture places increased stress on the posterior elements of the spine and raises intradiscal pressure (15, 16). Keegan (15) described the process of sitting in great detail in his article entitled, “Alterations of the lumbar curve related to posture and seating”. As the lumbar lordosis flattens in sitting, the center of gravity of the upper body is moved anterior to the lumbar vertebral bodies (15). This creates a perpendicular distance and thus an external flexion moment about the low back. In order to balance this moment, increased tension must be created from the lumbar erector muscles along with support from passive structures, thus increasing the load on the spine. Andersson et al. (17) found that intervertebral discs become anteriorly wedged in sitting, which places tensile pressures on the posterior aspect of the disc. Also carriage of more than 15% of the body weight may result in low back pain due to asymmetrical loading (18). This may be responsible for pain in 4.5% of the participant that involved in lifting equipment. Five respondents (7.6%) had pain at the head. This might be due to excessive irradiation by light rays, especially ultraviolet light that comes from the screen of the desktop or laptop they use. The head ache sometimes results from actinic irritation of the conjunctivae and the pain is referred to the surface of the head (19). Nine respondents have pain at both knees. This might be due to poor positioning of their legs due to inadequate spaces at the place of work since about 69.6% of the respondent complained of inadequate spaces. Stretching and strengthening exercises, 3-4 times a week is essential in order to prevent stiffness and achy knee joints (20) which may not be possible for an average administrator base on inadequate office space. Seven respondents (10.6%) have pain on their right hands while five respondents have left hand pains. This might be due to the design of the
tracking pad and mouse pad which is not designed with space for the hand to rest whenever the administrators are working on their laptop or desktop. The use of an independent keyboard and mouse when working on a laptop for more than an hour has been recommended in order to prevent pain (21). Another cause of pain at hand is any activity that involves repetitive wrist motion. De Quervain's disease is a repetitive stress injury that causes pain at the base of the thumb (22) Four respondents (6.1%) complained of neck pain. The findings of this study was lower than that of Dajpratham et al (23) who found a prevalence of 70.3 % of neck pain among dentist in a dental school in Thailand. Also Korkmaz (24) reported that neck pain was common among teachers in a part of Turkey which was in consonance with the finding of this study. Neck pain might be due to the screen height of the desktop or laptop the administrators are using. It could also be due to frequent flexion of the neck in order to write notes on the table. Ergonomist advise that the eyes should be level with the top of the monitor. This is achieved with the use of a desktop or laptop stand (25). More than 6.0% complained of having pain at the interior part of the body. This might be due to poor posture and prolonged sitting. Poor posture and prolonged sitting may result in structural deformation of the body, poor circulation, increased intravascular pressure and kicks in the bowels, slackening of the abdominal muscles and curvature of the spine which is bad for organ of digestion and breathing (8). Moreover, thirty seven respondents (56.1%) have a moderate pain, those that accounted that they have mild pains (30.3%) are more than respondent with severe pain (13.6%). This might be due to the fact that most of their administrative activity are now been performing with the assistance of a machine and equipment. The was in line with a study carried out by Ratzon et al, (26) that certain work demands such as prolonged sitting and standing activities in consulting, static postures, repetitive movement of the upper extremities, among other have been implicated in the etiology of work related musculoskeletal disorder among which is pain. The study revealed that there was no significant association between musculoskeletal pain intensity and year of experience this is in accordance with Scholey and Hair (27) who studied the incidence of musculoskeletal pain in United Kingdom and compared occupation. They found that there were
Work related musculoskeletal disorders among administrators in a Nigerian university Ojoawo Adesola O & all
Medicina Sportiva
2183 no differences between the groups for lifetime prevalence, annual prevalence, annual incidence and point prevalence for pain. This study also show that there was no significant relationship between musculoskeletal pain intensity and punctuality which was in line with a study carried out by Andersen et al, (28) on a prospective cohort study on severe pain as a risk factor for long-term sickness absence in blue- and white-collar workers They discovered that chronic knee pain, defined as at least 30 days with knee pain during the last year, was not a significant risk factor for long term sickness absence. For example, employee in sedentary occupations may not experience the same consequences of knee pain as employees with strenuous physical labor. This stresses the importance of determining occupation-specific thresholds of pain intensity for increased risk of long term sickness absence (28). In conclusion, the study has shown that the most prevalent musculoskeletal pain among administrator is low back pain due but this does not affect the activities in office and the longer the pain the higher the tendency for its reoccurrence. References
1. Haldeman S, Carroll L, Cassidy J.D, Schubert J, Nygren A (2008). The Bone and Joint Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders: Executive Summery. Spine; 33(4S), Suppl. 15 February.
2. Silverstein B, Adams D, Kalat J (2004). Work‐related Musculoskeletal Disorders of the Neck, Back and Upper Extremity in Washington State, 1994–2002. Technical Report 40‐8a‐2004, Washington State: Department of Labor and Industries.
3. Borh PC (2002). Efficacy of office ergonomic education. Journal of Occupational Rehabilitation; 10:(14).
4. Jones J R, Huxtable C S and Hodgson J T (2005). Self reported work-related illness in 2004/2005: Result from the labour force survey. A publication by Health and Safety Executives, Office of National Statics, United Kingdom: pp 47
5. Mbada C.A, Ayodele O, Fabunmi and Oyeyemi (2010). Work related musculoskeletal disorders among nurses and health practitioners in Ibadan. Journal of Epidemiology; 1:12-8.
6. Maniadakis N, Gray A. (2000). The economic burden of back pain in the UK. Pain; 84(1):95-103.
7. Popoola O.O (2012). Who is an Administrator: Unpublished write up. Dept of
Public Administration Obafemi Awolowo University, Ile Ife, Nigeria.
8. Adedoyin R.A, Idowu B.O, Adagunodo R.E, and Owoyomi A.A, Idowu P.A (2005). Musculoskeletal pain associated with the use of computer system in Nigeria. Technology and Health Care, 13:125-130.
9. Waddell G, Burton AK. (2001). Occupational health guidelines for the management of low back pain at work: evidence review. Occup Med (Lond); 51(2):124-35.
10. Silberstein S (2004). Migraine patho-physiology and its clinical implications. Cephalalgia; 24 (suppl 2): 2-7
11. Aguda Kehinde (2011). Pattern of musculoskeletal pain and injury among bankers in Ile Ife. Dissertation submitted to the Department of Medical Rehabilitation, Faculty of Basic Medical Sciences, Obafemi Awolowo University, Ile Ife. Nigeria, Questionnaire adapted and modified.
12. Akinpelu AO, Oyewole OO, Odole AC, Olukoya RO (2011). Prevalence of Musculoskeletal Pain and Health seeking Behaviour among Occupational Drivers in Ibadan, Nigeria Afr. J. Biomed. Res.; 89 - 94
13. Urquhart DM, Hoving JL, Assendelft WW, Roland M, van Tulder MW (2008). Urquhart, Donna M. ed: Antidepressants for non-specific low back pain. Cochrane database of systematic reviews. (Online) (1): CD001703.
14. Tyson A.C. Beach, Robert J. Parkinson, J. Peter Stothart, Jack P. Callaghan. (2005). Effects of prolonged sitting on the passive flexion stiffness of the in vivo lumbar spine The Spine Journal 5 145–154
15. Keegan JJ, Nebraska O (1953). Alterations of the lumbar curve related to posture and seating. Journal of Bone Joint Surgery (Br); 35A:589-603.
16. Andersson BJG, Ortengren R, Nachemson A, Elfstrom G. (1974). Lumbar disc pressure and myoelectric back muscle activity during sitting. IV studies on a car driver’s seat. ScandinavianJournal of Rehabilitation Medicine; 6:128-33.
17. Anderson BJG, Ortengren R, Nachemson AL, Elfstrom G, Broman H. (1975). The sitting posture: An electromyographic and discometric study. Orthopedic Clinics of North America; 6:105-20.
18. Ullrich Peter F. (2007). Pulled Back Muscle and Lower Back Strain. www.spine-ealth.com/.../lower-back-pain/pulled-back-muscle-and-lower-back-strain
19. Guyton Arthur C (2006). Somatic Sensation. Pain, Visceral Pain, Headache and Thermal Sensation. Textbook of Medical Physiology, 11th edition. Saunders Company Philadephia.
Work related musculoskeletal disorders among administrators in a Nigerian university
Ojoawo Adesola O & all
Medicina Sportiva
2184
20. Mueller Jen (2012) www.sparkpeople.com/ resource/fitness_articles.asp?id=895.
21. Office Ergonomics.com (2010). www.office ergonomics.com.
22. Noseworthy John (2011). Wrist pain, causes. www.mayo clinic.com.
23. Dajpratham Piyapat, Teerada Ploypetch Sirichai Kiattavorncharoen Kiatanant Boonsiriseth (2010). Prevalence and Associated Factors of Musculoskeletal Pain among the Dental Personnel in a Dental School J Med Assoc Thai; 93(6): 714-21.
24. Cetisli KN, Cavlak U, Telci EA (2011). Musculoskeletal pain, associated risk factors and coping strategies in school teachers. Scientific Research and Essays; 6(3): 649-657.
25. Stewart WF, Ricci JA, Chee E, Morganstein D, Lipton R, (2003). Lost productive time and cost due to common pain conditions in the US workforce. Journal of the American Medical Association; 290:2443–2454. jama.ama-assn.org/cgi/content/full/290/18/2443.
26. Ratzon, N.Z (1998). Musculoskeletal disorders among dentist and variation in dental work. Appl. Ergonomy; 29: 119-125.
27. Scholey M, Hair M (1989). Back pain in physiotherapist involved in back care education. Ergonomics; 32:179-190.
28. Andersen LL, Mortensen OS, Hansen JV, Burr H (2011). A prospective cohort study on severe pain as a risk factor for long-term sickness absence in blue- and white collar workers. Occup. Environ Med; 68: 590–592.
Corresponding author Ojoawo Adesola O
Department of Medical Rehabilitation, Faculty of Basic Medical Sciences, Obafemi Awolowo University (OAU) Ile Ife, Nigeria E-mail: [email protected] Received: June 14, 2013 Accepted: August 10, 2013

Medicina Sportiva (2013), vol. IX, no 3, 2185-2190 Romanian Sports Medicine Society
Comparison of effectiveness of the extracorporeal shock wave therapy (ESWT) and steroid injection at plantar fasciitis treatment Mustafa Onur Serbest, Halil İbrahim Kaya, Mustafa Hilmi Demir, Sabriye Ercan, Cem Cetin Medicine Faculty of Suleyman Demirel University, Department of Sport Medicine, Isparta, Turkey Abstract. Aim and scope. Plantar fasciitis is one of the leading causes of heel pain and approximately 10% of the population has plantar fasciitis. Plantar fasciitis is a self limiting clinical situation and most of the patients benefits from conservative treatment. The purpose of the study was to compare effectiveness of the extracorporeal shock wave therapy (ESWT) and local steroid injection at plantar fasciitis patients. Method. 30 patients with heel pain were enrolled into study were divided into two groups randomly. One of the group received steroid treatment, the other group received ESWT treatment. The steroid group had (n=15) 3 mg betametason acetate, 3.947 mg betametasondisodium phosphate and 20mg 2% prilocain injection; where the maximum tenderness and pain point; the ESWT group (n=15) had ESWT treatment (15 Hz frequency, 20 Barr Energy and 2000 shocks/session once a week) for total 3 sessions. Results. For ESWT group; VAS scores were decreased from 7.56 to 5.2 one week after treatment; to 3.78 one month after the treatment and to 3.67 three month after the treatment; respectively. Steroid groups VAS scores were decreased from 6.55 to 3.11 one week after treatment; to 2.14 one month after treatment and to 1.42 three month after treatment; respectively. Both of the groups VAS scores were decreased statistically significantly. Conclusion. As a result, both steroid injection and ESWT application are effective and safe treatment methods in heel pain caused by plantar fasciitis and are alternative methods for surgical treatment. In our study, we found that local steroid injection application provided significantly greater decrease in pain according to ESWT treatment. Local steroid injection has shown more successful than ESWT treatment. Key words: plantar fasciitis, visual analog pain scale (VAS), extracorporeal shock wave therapy (ESWT), steroid injection. Introduction Plantar fasciitis is one of the leading cause of heel pain and approximately 10% of the population have plantar fasciitis (1). In addition to injuries of origin of the plantar fascia; anomalies of the foot biomechanics can lead to this disease. Plain radiographs may reveal a plantar heel spur, but this heel spurs can be seen incidentally at patients whom does not have any symptoms of plantar fasciitis. Clinical findings and thickness of the spurs does not correlate (2,3). It’s not a traction osteophyte. However it’s considered to be occurred as a reaction at the inflamed tissue which is attached to calcaneus. On the other hand heel spur should not be thought as a reason of heel pain at plantar fasciitis (4). Sometimes there is a sharp heel pain which radiates to lower leg. And sometimes walking and mobility is significantly effected (5). The pain was reported particularly bad with the first steps taken on rising in the morning or after a prolonged rest. Prolonged standing and walking may increase the pain (6-8). Pain localized at the plantar-medial calcaneal tubercle was considered
classical sign. Pain may be reproduced by passive stretching of the plantar fascia and palpation over the heel and proximal portion of the plantar fascia (7,9). Ankle deformities, obesity, overuse injuries are caused repetitive trauma and predispose plantar fasciitis. This cumulative and repetitive microtrauma leads to chronic injury at the site of where plantar aponeurosis inserts to medial tubercle of calcaneus (5,10). The chronic damage is followed by a decreased elasticity of the insertional cartilage. Gaps in the impaired cartilage are invaded by mesenchymal cells which form scar tissue. After new vessels have developed, the scar slowly ossifies which can lead to the growing bony spurs (5). Diagnose of the plantar fasciitis isn’t complicated usually, but nerve entrapment syndromes and seronegative arthropathies should be remembered for differential diagnosis (8). Plantar fasciitis is a self limiting clinical situation and most of the patients benefits from conservative treatment (11).
2185

Comparison of effectiveness of the extracorporeal shock wave therapy (ESWT) and steroid injection at plantar fasciitis treatment
Mustafa Onur Serbest & all
Medicina Sportiva
2186 Orthopedic shoes, heel lifts for lowering the weight-bearing, non-steroidal anti-inflammatory drugs, injections of local corticosteroid and local anesthetics, iontophoresis, microwave and ultrasound are treatment modalities that are used usually (5). Extracorporeal shock wave therapy (ESWT) has been approved for plantar fasciitis at 2000 by U.S. FDA (U.S. Food and Drug Administration) (12). ESWT has advantages like being a non-invasive method, well tolerated by the patients, application without pain and less side effects (13,14). Even there are studies and meta-analyses showing ESWT is effective at treating plantar fasciitis, some other studies show that there are no significant difference between other treatment modalities and ESWT (15-17). According to Kuda et al. this results should be occurred because of technical differences (machine design, shock intensity, frequency, number of sessions, different treatment choices for placebo), differences at patient population, differences between intensity of disease and differences between the working designs (18). On literature, there are non-standardized treatment regimens like 10 shocks/session to 3000 shocks/session, from application of treatment once a week to once a month and total number of sessions from just once to six times (8,17,19). The purpose of the current study: to compare the effectiveness of ESWT treatment and local steroid injection on plantar fasciitis. Material and Method Between February 2012- February 2013, 30 patients who applied to Sports Medicine Clinic of Suleyman Demirel University Research and Education Hospital, with heel pain were enrolled to this study. Inclusion Criteria: >18 years old; severe pain at first step after wakening up in the morning; symptoms lasting more than 6 weeks; pain with passive dorsiflexion and pressure to medial calcaneal tubercule; patients who claim that don’t use any other treatments during treatment period. Exclusion Criteria: <18 years old; Diabetes mellitus; neurological deficits; nerve entrapments; rheumatoid arthritis and other rheumatological diseases; pregnancy; tumor; infection; coagulation disorders; peripheral vascular disease; calcaneal stress fracture; no corticosteroid injections should be done and no physical therapy modalities (e.g. transcutanous electrical nerve stimulation, ionto -
phoresis, ultrasound, ESWT) should be used in last 6 weeks; regular non-steroidal anti-inflammatory drug use. Plantar fasciitis was diagnosed with a thorough history and physical examination. Patients who have symptoms more than 6 weeks were enrolled to study. All patients were informed for treatment, side effects, and contraindication in orally and writing. Informed consents were signed by all patients. All of the patients had severe pain in the first step after wakening up in the morning and pain was increasing with the activity. During physical examination of the medial calcaneal tubercule and proximal part of plantar fascia, there was pain, that aggravated with palpation. The patients enrolled into study were divided into two groups randomly. One of the group received steroid treatment, the other group received ESWT treatment. The point where the maximum tenderness and pain was occurring; the steroid group had (n=15) 3 mg betametason acetate, 3.947 mg betametasondisodium phosphate and 20mg 2% prilocain injection; the ESWT group (n=15) had ESWT treatment (ILITH-ESWT, ELMSTechMedical, New York, USA) 15Hz frequency, 20 Barr Energy and 2000 shocks/session once a week for total 3 sessions. Patients admitted to supine position and injections were done in a sterile area at optimum conditions. The most tender and the painful point localized with palpation. This point is sterilized with alcohol and betadine. The injection was done at 45 degree angle from 1cm. distal and just medial to this point to center of the heel was aimed laterally, superiorly and dorsally. Severity of the patients’ pain were noted to 10 cm length visual analog pain scale (VAS) four times; just before the treatment, one week after the treatment, one month after the treatment and three months after the treatment. During the study, all treatment modalities were done by the same physician. Patients’ VAS scores were followed by another physician. Any side effect of treatments of both groups wasn’t determined during therapy and follow up. Statistical Analyses. All informations analyzed by using SPSS 15.0 Package Software. While defining the data descriptive statistics used and to evaluate if there is a significant difference between the VAS Score of Steroid Group and Vas score of ESWT Group, we used independent samples T-test. For intragroup evaluation Paired Samples T-test was used.
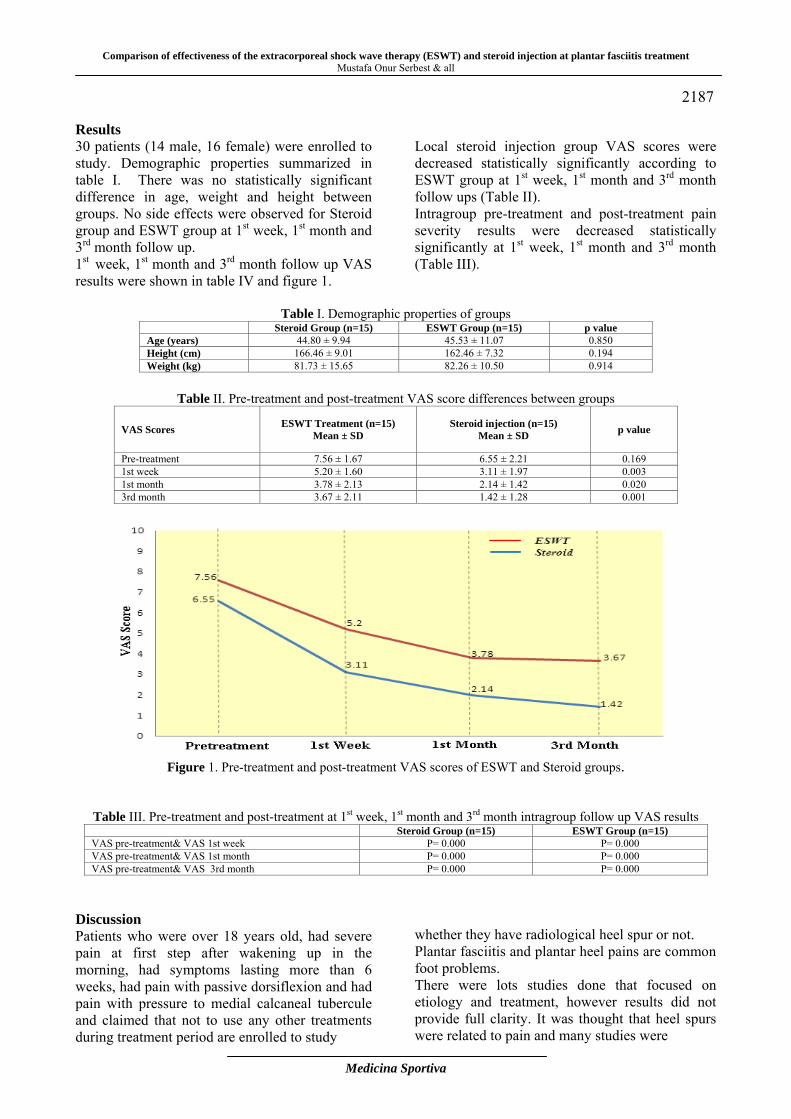
Comparison of effectiveness of the extracorporeal shock wave therapy (ESWT) and steroid injection at plantar fasciitis treatment Mustafa Onur Serbest & all
Medicina Sportiva
2187 Results 30 patients (14 male, 16 female) were enrolled to study. Demographic properties summarized in table I. There was no statistically significant difference in age, weight and height between groups. No side effects were observed for Steroid group and ESWT group at 1st week, 1st month and 3rd month follow up. 1st week, 1st month and 3rd month follow up VAS results were shown in table IV and figure 1.
Local steroid injection group VAS scores were decreased statistically significantly according to ESWT group at 1st week, 1st month and 3rd month follow ups (Table II). Intragroup pre-treatment and post-treatment pain severity results were decreased statistically significantly at 1st week, 1st month and 3rd month (Table III).
Table I. Demographic properties of groups Steroid Group (n=15) ESWT Group (n=15) p value Age (years) 44.80 ± 9.94 45.53 ± 11.07 0.850 Height (cm) 166.46 ± 9.01 162.46 ± 7.32 0.194 Weight (kg) 81.73 ± 15.65 82.26 ± 10.50 0.914
Table II. Pre-treatment and post-treatment VAS score differences between groups
VAS Scores ESWT Treatment (n=15) Mean ± SD
Steroid injection (n=15) Mean ± SD p value
Pre-treatment 7.56 ± 1.67 6.55 ± 2.21 0.169 1st week 5.20 ± 1.60 3.11 ± 1.97 0.003 1st month 3.78 ± 2.13 2.14 ± 1.42 0.020 3rd month 3.67 ± 2.11 1.42 ± 1.28 0.001
Figure 1. Pre-treatment and post-treatment VAS scores of ESWT and Steroid groups.
Table III. Pre-treatment and post-treatment at 1st week, 1st month and 3rd month intragroup follow up VAS results Steroid Group (n=15) ESWT Group (n=15)VAS pre-treatment& VAS 1st week P= 0.000 P= 0.000 VAS pre-treatment& VAS 1st month P= 0.000 P= 0.000 VAS pre-treatment& VAS 3rd month P= 0.000 P= 0.000
Discussion Patients who were over 18 years old, had severe pain at first step after wakening up in the morning, had symptoms lasting more than 6 weeks, had pain with passive dorsiflexion and had pain with pressure to medial calcaneal tubercule and claimed that not to use any other treatments during treatment period are enrolled to study
whether they have radiological heel spur or not. Plantar fasciitis and plantar heel pains are common foot problems. There were lots studies done that focused on etiology and treatment, however results did not provide full clarity. It was thought that heel spurs were related to pain and many studies were

Comparison of effectiveness of the extracorporeal shock wave therapy (ESWT) and steroid injection at plantar fasciitis treatment
Mustafa Onur Serbest & all
Medicina Sportiva
2188 Because it can be determined generally in population. Prevalence of heel spur does not related by gender, but increases with age (20). Weight increase facilitates the heel spur formation. In our study most of patients were obese and elder aged. Similarly Prichasuk et al. (2) showed that at their study, which was looking for if there was a relation between pes planus and calcaneal spur, most of the patients were obese. Over weight and age are the major factors that lowers the calcaneal slope and leads to calcaneal spur formation (2). Treatment of the disease is mainly conservative. In addition to physical therapy modalities; Achilles tendon and plantar fascia stretching, modification of activities are usually suggested treatment methods (21). Surgery is recommended for the patients who are resistant to treatment modalities and who has foot deformities (22). Low dose radiotherapy and shock waves has been started to use in last decades (5, 23). Iontophoresis, microwave and ultrasound are commonly used physical therapy modalities (20, 24, 25). ESWT is recommended as an effective treatment. Purpose of ESWT treatment is not to remove heel spur, but to reduce inflammation and pain. Buch et al. determined that there was no radiological change at heel spur after treatment (26). Different investigation for the effectiveness of ESWT in the treatment of plantar fasciitis has been done. Different treatment protocols were created by different machines, different energy intensity and different session numbers. Even there are so many protocols, it is impossible to say that one is superior to another (27). In a randomized controlled trial, Rompe et al. compared 2 different ESWT protocols in their study which applied to 112 patients. For group 1, three session EWST treatment was done in 2 weeks, ESWT was undertaken with 1000 shock for group 1. Three session ESWT treatment was done 3 sessions in 2 weeks for the second group. ESWT was undertaken with 10 shocks for group 2. In group 1, VAS scores were decreased from 77 to 19, but in group 2 there was not a statistically significant decrease on 6th week after treatment (28). In our study, 15 Hz frequency, 20 Barr Energy and 2000 shocks/session for a total of 3 sessions, ESWT treatment with 1 week intervals was performed. 1 week after treatment, VAS scores were decreased from 7.56 to 5, 2, 1 month after
the treatment VAS scores decreased from 7.56 to 3.78 and 3 month after the treatment VAS scores decreased from 7.56 to 3.67 and those results were statistically significant. Successful results were obtained through repetitive low energy ESWT application in short and medium term. In a meta-analyses, success for chronic plantar fasciitis had a ratio as 88% (29). In this study, the steroid group had 3 mg betametason acetate, 3.947 mg betametasondisodium phosphate and 20 mg 2% prilocain injection. Steroid groups VAS scores were decreased from 6.55 to 3.11 at 1st week; 6.55 to 2.14 at 1st month and 6.55 to 1.42 at 3rd month. According the study, both of the groups 1st week, 1st month and 3rd month VAS scores were decreased statistically significantly On the other hand studies focused on the treatment of heel spur, US guided or local steroid injection with palpation have been found successful. Kane et al. (30) showed that US-guided injection is not superior to palpation-determined injection. Genç et al. showed that steroid injection is effective for plantar fasciitis treatment (31). Crawford et al. (32) showed that with only one steroid injection, well-being was continued for a month, but in the 3rd month effects were lasted. In our study, it is revealed that local steroid injection is more effective than ESWT treatment at 1st week, 1st month and 3rd month after treatments. In our study significant treatment success was obtained both steroid and ESWT treatment. hen the groups compared with each other, the success of steroid treatment group is superior to ESWT treatment group. Porter et al. similarly showed that steroid treatment is more effective than ESWT treatment (33). Conclusions As a result of the study, both steroid injection and ESWT application are effective and safe treatment methods in heel pain caused by plantar fasciitis and are alternative methods for surgical treatment. We also consistent with the literature, found that local steroid injection application provided significantly greater decrease in pain according to ESWT treatment. To define the effective treatment method for plantar fasciitis, cost/effectiveness analysis and placebo-controlled, new researches which is used other conservative treatment methods, are needed.
Comparison of effectiveness of the extracorporeal shock wave therapy (ESWT) and steroid injection at plantar fasciitis treatment Mustafa Onur Serbest & all
Medicina Sportiva
2189 References 1. DeMaio M, Paine R, Mangine RE, Drez D Jr
(1993). Plantarfasciitis. Orthopedics; 16(10):1153-63.
2. Prichasuk S, Subhadrabandhu T (1994). The relationship of pes planus and calcaneal spur to plantar heelp ain. Clin Orthop; 306:192-6.
3. Cosentino R, Falsetti P, Manca S, De Stefano R, Frati E,Frediani B, Baldi F, Selvi E, Marcolongo R: (2001). Efficacy of extracorporeal shock wave treatment in calcanealen the sophytosis. AnnRheumDis; 60(11):1064-7.
4. Aldridge T. Diagnosing heel pain in adults (2004). Am Fam Physician; 70:332-8.
5. Mücke R, Schönekaes K, Micke O, Seegenschmiedt MH, Berning D,Heyder R (2003). Low-Dose Radiotherapy for Painful Heel Spur. Strahlenther Onkol; 179:774-8.
6. Yücel I, Yazıcı B, Değirmenci E, Erdoğmuş B, Doğan S (2009). Comparison of ultrasound-, palpation-, and scintigraphy-guided steroid injections in the treatment of plantar fasciitis. Arch Orthop Trauma Surg. 129(5):695-701
7. Toker S, Kılıncoğlu V, Güven M, Özkan N K, Gülcan E, Aksakallı E, Akman B (2008). Early and mid-term results of calcaneal spur treatment with local corticosteroid and anesthetic agent. The Medical Journal of SSK Göztepe Educational Hospital; 23(2): 59-62.
8. Davis PF, Severud E, Baxter DE (1994). Painful heel syndrome: results of non-operative treatment. Foot Ankle Int; 15: 531-535.
9. Miller MD (1992). Review of orthopedics. Philadelphia: WB Saunders Company; pp 107-119.
10. Tallia AF, Cardone DA (2003). Diagnostic and Therapeutic Injection of the Ankle and Foot. American Fam Physician; 68(7): 1356-62.
11. Michelsson O, Konttinen YT, Paavolainen P, Santavirta S (2005). Plantar heel pain and its 3-mode 4-stage treatment. Mod Rheumatol; 15:307-14.
12. Henney JE (2000). From the Food and Drug Aministration: shock wave for heel pain. JAMA; 284: 2711.
13. Chaussy C, Eisenberger F, Wanner K (1976). The use of shock waves for the destruction of renal calculi with out direct contact. UrolRes; 181:352-357.
14. Vulpiani MC, Trischitta D, Trovato P, Vetrano M,Ferretti A (2009). Extra corporeal shock wave therapy (ESWT)in Achilles tendinopathy. A long-term follow-up observational study. J Sports Med Phys Fitness; 49(2): 171-6.
15. Ogden JA, Alvarez R, Levitt R, Cross GL, MarlowM (2001). Shock wave therapy for chronic proximal plantar fasciitis. Clin Orthop Relat Res; (387):47-59.
16. Buch M, Knorr U, Fleming L, Theodore G,
AmendolaA, Bachmann C et al (2002). Extracorporeal shock wave therapy in symptomatic heel spurs. An overview. Orthopade; 31: 637-44.
17. Speed CA, Nichols D, Wies J, Humphreys H, RichardsC, Burnet S, et al (2003). Extracorporeal shock wave therapy for plantar fasciitis. A double blind randomised controlled trial. J Orthop Res; 21:937-940.
18. Kudo P, Dainty K, Clarfield M, Coughlin L, Lavoie P, Lebrun C (2006). Randomized, Placebo-Controlled, Double-Blind Clinical Trial Evaluating the Treatment of Plantar Fasciitis with an Extracorporeal Shock wave Therapy (ESWT) Device: A North American Confirmatory Study. J Orthop Res; 24(2):115-23.
19. Dietrich S, AdamF, KreutzA, RuppS, KohnD, SeilR 92005). Ultrasonographic evaluation at 6-month follow-up plantar fasciitis after extracorporeal shock wave therapy. Arch Orthop Trauma Surg; 125:6-9.
20. Williams PL, Smibert JG, Cox R,Mitchell R,Klenerman L (1987). Imaging study of the painful heel syndrome. Foot Ankle; 7:345.
21. Perlick L, Boxberg W, Giebel G. (1998). High energy shock wave treatment of the painful heel spur. Unfallchirurg; 101:914-8.
22. Hoppenfield S, deBoer P (1994). Exposures in Orthopedics: The Anatomic Approach. 2 nd ed. Philadelphia: J. B. Lippincott Company.
23. Chen HS, Chen LMC, Huang TW (2001). Treatment of Painful Heel Sendrome With Shock Waves. Clin Orthop; 387:47-9.
24. Boike Am, Snyder AJ, Roberto PD, Tabbert WG (1993). Heel spur surgery. A transverse plantar approach. J Am Podiatr Med Assoc; 83:39-42.
25. Dailey JM (1991). Differential diagnosis and treatment of heel pain. Clin Podiatr Med Surg; 8:153-66.
26. Buch M, Schlangmann BA, Lubbers C, Trager D,Siebert WE (1998). Results of shock wave therapy of calcaneal spurs from the Orthopedic Hospital in Kassel: influence of various parametres on the outcome In: Siebert W, Bunch M, editors. Extracorporeal shock waves in orthopedics. Berlin: Springer, pp 30-35.
27. Tornese D,Mattei E,Lucchesi G,Bandi M,Ricci G,Melegati G (2008). Comparison of two extracorporeal shock wave therapy techniques for the treatment of painful subcalcaneal spur. A randomized controlled study. Clinical Rehabilitation; 22: 780-87.
28. Rompe JD, Decking J, Schoellner C, Nafe B (2003). Shock Wave Application for Chronic Plantar Fasciitis in Running Athletes: A Prospective, Randomized, Placebo-Controlled Trial. The American Journal of Sports Medicine; 31(2): 268-75.
Comparison of effectiveness of the extracorporeal shock wave therapy (ESWT) and steroid injection at plantar fasciitis treatment
Mustafa Onur Serbest & all
Medicina Sportiva
2190 29. Ogden JA, Alvarez RG, Marlow M (2002).
Shockwave therapy for chronic plantar fasciitis: a meta-analysis. Foot Ankle Int.; 23:301-308.
30. Kane D, Geaney T, Shanaha M, Duffy G, Bresnihan B, Gibney R, et al (2001). The role of ultrasonography in the diagnosis and management of idiopathic plantar fasciitis. Rheumatology; 40:1002-8.
31. Genc H, Saracoğlu M, Nacır B, Erdem HR, Kacar M (2003). Ultrasonographic evaluation of plantar fasciitis steroid injection site. Rheumatol Med Rehab; 14(1):16-20.
32. Crawford F, Atkins D, Young P, Edwards J (1999). Steroid injection for heel pain: evidence of short term effectiveness. A randomized controlled trial. Rheumatology; 38:974-7.
33. Porter MD, Shaldbolt B (2005). Intralesional corticosteroid injection versus extracorporeal shock wave therapy for plantar fasciopaty. Clin J Sport Med; 15:119-124.
Corresponding Author Prof. Dr. Cem Çetin Medicine Faculty of Suleyman Demirel University, Department of Sports Medicine, 32260 Isparta, Turkey E-mail: [email protected] Phone: +90 246 2119260 Received: May 27, 2013 Accepted: July 23, 2013

Medicina Sportiva (2013), vol. IX, no 3, 2191-2197 Romanian Sports Medicine Society
Our experience in treating femoral diaphyseal fractures and their most common complications Radu Ciuvică1, Mirela Vasilescu2, Anca Bordianu3 Anca Mirela Ionescu 4, Ştefan Cristea5
1Department of Orthopedics and Traumatology, University of Medicine and Pharmacy Carol Davila, Clinical Emergency Hospital Bagdasar-Arseni, Bucharest 2Kinesiology and Sports Medicine Department, University of Craiova 3Department of Plastic and Reconstructive Surgery, University of Medicine and Pharmacy Carol Davila, Clinical Emergency Hospital Bagdasar-Arseni, Bucharest 4Sports Medicine Department, University of Medicine and Pharmacy Carol Davila, Bucharest 5Department of Orthopedics and Traumatology, University of Medicine and Pharmacy Carol Davila, Clinical Emergency Hospital Sf. Pantelimon, Bucharest, Romania
Abstract. State of paper's purpose. The femoral diaphyseal fractures are one of the most frequent and serious traumatic disorders encountered in orthopedic practice which can lead to severe squeals if not managed correctly. This study analyzes the femoral diaphyseal fractures surgically treated in two large trauma centers from Bucharest during 5 years. We assessed the treatment methods, the associated lesions and the most frequent complications. The most frequent late complication found in our series of patients was the nonunion, which accounted for 14,7% of the cases. Considering the frequency and the severity of this complication the study tried to elaborate a treatment algorithm and a new classification for the nonunion and to evaluate the results of the surgical treatment of femoral diaphyseal nonunion. Key words: femoral diaphyseal fracture, internal fixation, complications, nonunion. Introduction Femoral diaphyseal fractures represent a frequent pathological entity in trauma surgery, being severe lesions which can lead to very important functional squeals if not correctly managed (1). The incidence of femoral diaphyseal fractures vary between different countries and between different areas of the same country, the femoral fractures being more frequent in urban areas, due to the greater incidence of motorvehicle accidents (2). The incidence of femoral diaphyseal fractures has two ages – related peaks, one and the most important in young people sustaining high-energy trauma and the second one in elderly people sustaining low-energy trauma such as falling from the same level (3). The association of femoral fractures with other severe injuries often complicates treatment, especially in high energy trauma. The treatment methods evolved from non-operative techniques such as splinting and traction to operative treatment which is now the golden standard for the treatment of femoral fractures. The internal fixation techniques sustained a remarkable evolution during the last 40 years. Considerable changes occurred in the early operative management of femoral fractures,
particularly in the context of a multiply injured patient. Nowadays the internal fixation methods vary a lot, depending on the fracture type, the soft tissues condition, the associated injuries and the surgeon’s experience. The commonest method of internal fixation for the closed femoral diaphyseal fractures is the intramedullary nail, reamed or unreamed. The femoral diaphyseal fractures are associated with early and late complications that can affect the functional outcome. One of the most important and functional impairing late complication is the nonunion, which occurs more frequently if an unreamed intramedullary nail is used for the fixation of the fracture. The nonunion is difficult to define due to the great variety of fracture patterns and associated lesions, but is generally accepted that a nonunion represents the lack of bone healing nine months after the fracture fixation, with no sign of progressive healing for three months (4). Nonunions are caused by a large number of factors such as impaired bone vascularity, infection, excessive fracture site mobility, large bone defects, soft tissue interposition, the use of nonsteroidal anti-inflammatory drugs (5), certain neurological
2191
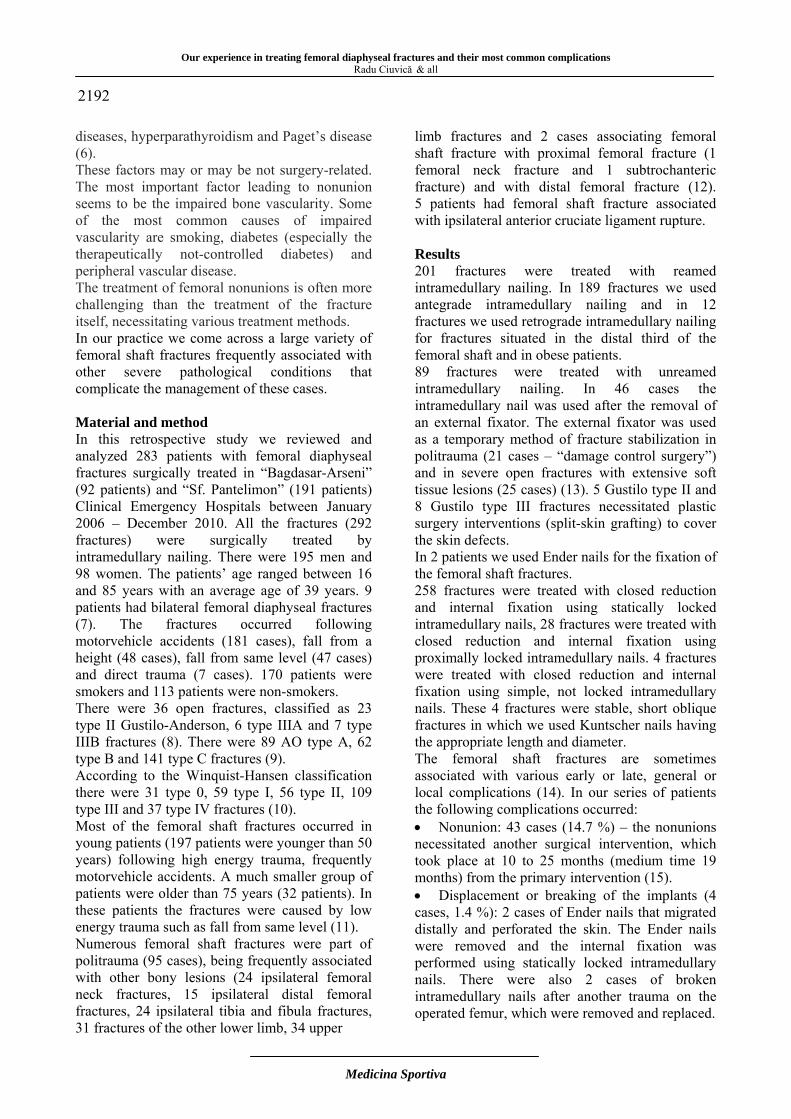
Our experience in treating femoral diaphyseal fractures and their most common complications
Radu Ciuvică & all
Medicina Sportiva
2192 diseases, hyperparathyroidism and Paget’s disease (6). These factors may or may be not surgery-related. The most important factor leading to nonunion seems to be the impaired bone vascularity. Some of the most common causes of impaired vascularity are smoking, diabetes (especially the therapeutically not-controlled diabetes) and peripheral vascular disease. The treatment of femoral nonunions is often more challenging than the treatment of the fracture itself, necessitating various treatment methods. In our practice we come across a large variety of femoral shaft fractures frequently associated with other severe pathological conditions that complicate the management of these cases. Material and method In this retrospective study we reviewed and analyzed 283 patients with femoral diaphyseal fractures surgically treated in “Bagdasar-Arseni” (92 patients) and “Sf. Pantelimon” (191 patients) Clinical Emergency Hospitals between January 2006 – December 2010. All the fractures (292 fractures) were surgically treated by intramedullary nailing. There were 195 men and 98 women. The patients’ age ranged between 16 and 85 years with an average age of 39 years. 9 patients had bilateral femoral diaphyseal fractures (7). The fractures occurred following motorvehicle accidents (181 cases), fall from a height (48 cases), fall from same level (47 cases) and direct trauma (7 cases). 170 patients were smokers and 113 patients were non-smokers. There were 36 open fractures, classified as 23 type II Gustilo-Anderson, 6 type IIIA and 7 type IIIB fractures (8). There were 89 AO type A, 62 type B and 141 type C fractures (9). According to the Winquist-Hansen classification there were 31 type 0, 59 type I, 56 type II, 109 type III and 37 type IV fractures (10). Most of the femoral shaft fractures occurred in young patients (197 patients were younger than 50 years) following high energy trauma, frequently motorvehicle accidents. A much smaller group of patients were older than 75 years (32 patients). In these patients the fractures were caused by low energy trauma such as fall from same level (11). Numerous femoral shaft fractures were part of politrauma (95 cases), being frequently associated with other bony lesions (24 ipsilateral femoral neck fractures, 15 ipsilateral distal femoral fractures, 24 ipsilateral tibia and fibula fractures, 31 fractures of the other lower limb, 34 upper
limb fractures and 2 cases associating femoral shaft fracture with proximal femoral fracture (1 femoral neck fracture and 1 subtrochanteric fracture) and with distal femoral fracture (12). 5 patients had femoral shaft fracture associated with ipsilateral anterior cruciate ligament rupture. Results 201 fractures were treated with reamed intramedullary nailing. In 189 fractures we used antegrade intramedullary nailing and in 12 fractures we used retrograde intramedullary nailing for fractures situated in the distal third of the femoral shaft and in obese patients. 89 fractures were treated with unreamed intramedullary nailing. In 46 cases the intramedullary nail was used after the removal of an external fixator. The external fixator was used as a temporary method of fracture stabilization in politrauma (21 cases – “damage control surgery”) and in severe open fractures with extensive soft tissue lesions (25 cases) (13). 5 Gustilo type II and 8 Gustilo type III fractures necessitated plastic surgery interventions (split-skin grafting) to cover the skin defects. In 2 patients we used Ender nails for the fixation of the femoral shaft fractures. 258 fractures were treated with closed reduction and internal fixation using statically locked intramedullary nails, 28 fractures were treated with closed reduction and internal fixation using proximally locked intramedullary nails. 4 fractures were treated with closed reduction and internal fixation using simple, not locked intramedullary nails. These 4 fractures were stable, short oblique fractures in which we used Kuntscher nails having the appropriate length and diameter. The femoral shaft fractures are sometimes associated with various early or late, general or local complications (14). In our series of patients the following complications occurred: • Nonunion: 43 cases (14.7 %) – the nonunions necessitated another surgical intervention, which took place at 10 to 25 months (medium time 19 months) from the primary intervention (15). • Displacement or breaking of the implants (4 cases, 1.4 %): 2 cases of Ender nails that migrated distally and perforated the skin. The Ender nails were removed and the internal fixation was performed using statically locked intramedullary nails. There were also 2 cases of broken intramedullary nails after another trauma on the operated femur, which were removed and replaced.

Our experience in treating femoral diaphyseal fractures and their most common complications Radu Ciuvică & all
Medicina Sportiva
2193 • Infectious complications – there were 5 superficial infections and 3 deep infections (osteomyelitis). The superficial infections were treated with debridement and lavage associated with broad spectrum antibiotic treatment. 2 cases with deep infection necessitated implant removal and the use of an external fixator for the fracture stabilization. In the third case of deep infection, with clinical appearance 8 months postoperatively, we decided to keep the implant in place until the bony union (11 months postoperatively) associated with intravenous and oral antibiotic treatment. • Malunion – 24 cases, 17 of which necessitated a second intervention to restore the femoral length, axis and rotation. The nonunion was defined as the lack of bony union 9 months after the internal fixation of the fracture or the lack of callus formation progression (radiological assessed) for three consecutive months. The nonunion is the most frequent late complication of femoral shaft fractures. According to the Weber classification of nonunions there were 25 cases of hypertrophic nonunion, 12 cases of oligotrophic nonunion and 6 cases of atrophic nonunion. The treatment of nonunion was surgical in all cases and it consisted in: reaming and replacement of the intramedullary nail with a larger diameter intramedullary nail – 15 cases; plate and screws internal fixation associated with decortication and the use of bone graft – 10 cases; dynamization of the intramedullary nail – 9 cases; plate and screws internal fixation – 3 cases; compression external fixator – 2 cases; bone substitute applied in the cortical bone defect – 2 cases; bone graft and decortication– 2 cases. In a limited number of cases we used complementary treatment methods such as ultrasound therapy (14 cases) and shock wave therapy (8 cases). These complementary therapies seem to have favorable effects for the new bone formation but our experience in the use of these methods is restraint. To assess the effectiveness of these methods it’s necessary to perform studies on larger number of patients. Discussions Considering the severity of this complication and the importance of its correct treatment we tried to elaborate an algorithm for the treatment of nonunions, by grouping the nonunions by their type according to the Weber classification (hypertrophic or oligo/atrophic nonunion) (16), the amount of callus formed at the fracture site
being an expression of the bone biological activity, by the presence or absence of a bone defect at the fracture site and its dimensions and by the stability of the fracture site after the internal fixation. We grouped the nonunions as type H (hypertrophic) or type A (atrophic), according to the Weber classification (hypertrophic or oligo/atrophic), D considering the type and dimensions of the bone defect at the fracture site (D0 – no bone defect, D1 – small dimensions bone defect, D2 – large dimensions bone defect, D3 – segmental bone defect) and S considering the stability of the internal fixation (S0 – unstable internal fixation, S1 – stable internal fixation). According to this classification, the nonunions are grouped as it follows: • Hypertrophic nonunion without bone defect with stable internal fixation (HD0S1) • Hypertrophic nonunion with small bone defect with stable internal fixation (HD1S1) • Hypertrophic nonunion without bone defect with unstable internal fixation (HD0S0) • Hypertrophic nonunion with small bone defect with unstable internal fixation (HD1S0) • Atrophic or oligotrophic nonunion with small bone defect with stable internal fixation (AD1S1) • Atrophic or oligotrophic nonunion with large bone defect with stable internal fixation (AD2S1) • Atrophic or oligotrophic nonunion with segmental bone defect with stable internal fixation (AD3S1) • Atrophic or oligotrophic nonunion with small bone defect with unstable internal fixation (AD1S0) • Atrophic or oligotrophic nonunion with large bone defect with unstable internal fixation (AD2S0) • Atrophic or oligotrophic nonunion with segmental bone defect with stable internal fixation (AD3S0) The nonunion were treated according to this classification. In the HD0S1 and HD1S1 nonunions we dynamized the statically locked nails. For the HD0S0 and HD1S0 nonunions it was necessary to remove the intramedullary nail and to use another internal fixation method: reaming followed by the use of a larger diameter nail, compression plate or external fixator that produced compression at the fracture site. The AD1S1 nonunions were treated by the dynamization of the statically locked nails. For the AD2S1 and AD3S1 nonunions we applied autologuos bone graft from the iliac crest or bone

Our experience in treating femoral diaphyseal fractures and their most common complications
Radu Ciuvică & all
Medicina Sportiva
2194 substitute at the nonunion site, without exchanging the fixation method. In AD1S0 nonunions we exchanged the intramedullary nail with a larger diameter statically locked nail, after the reaming of the intramedullary canal. In AD2S0 nonunions we reamed the intramedullary canal, exchanged the intramedullary nail with a larger diameter statically locked nail and applied autologous bone grafts at the nonunion site. The AD3S0 nonunions were treated using different methods: reaming of the intramedullary canal and exchanging the nail with a larger diameter nail, removing of the nail and fixation of the nonunion site with plate and screws (17). In all of these cases we applied autologous bone graft or bone substitute at the nonunion site. Conclusions The femoral diaphyseal fractures are a very important entity in trauma surgery that are frequently associated with life-threatening lesions and are sometimes followed by severe late complications, the most frequent being the nonunion (18). The soft tissues condition is of major importance for the initial treatment of the fracture, but also for the late outcome. Some cases with extensive soft tissues lesions necessitate plastic surgery interventions to insure the appropriate coverage of the bone and by that to reduce the risk of infection and help the healing process minimizing the vascular impairment. The plastic surgery interventions are needed in severe
open fractures (Gustilo type II and III) (19). The nonunion is probably the most challenging complication to treat, its treatment necessitating specific fixation methods, being time consuming and requiring an excellent surgical knowledge and experience in treating such cases (20). The causes leading to nonunion are numerous (impaired bone vascularity, infection, excessive fracture site mobility, large bone defects, compartment syndrome (21), soft tissue interposition, the use of nonsteroidal anti-inflammatory drugs). The most important factor leading to nonunion is the impairment of bone vascularity, while the most important surgery-related factor seems to be the excessive fracture site mobility. The amount of resources used to manage these complex cases and their complications and the difficulty encountered in choosing the appropriate treatment method suggest that the implementation of a new classification for the femoral nonunions followed by a treatment algorithm based on this classification could ease the decision making process regarding the treatment method to follow in a specific case and may lead to better therapeutic results. Case 1: 44 yrs old male, motorvehicle accident, right femoral shaft fracture AO type C, left supracondylar femoral fracture AO type, minor head injury. The treatment consisted in closed reduction and internal fixation of both fractures, using an antegrade reamed statically locked intramedullary nail for the femoral shaft fracture and a retrograde unreamed statically locked intramedullary nail for the supracondylar fracture, with good postoperative results.
Case 2: 26 yrs old male, professional soccer player, victim of a motorvehicle accident (driver) that resulted in politrauma (multiple rib fractures, thoracic contusion, head injury, open complex left femoral shaft fracture Gustilo-Anderson type II,
AO type C3, Winquist-Hansen grade IV). Closed reduction and internal fixation of the femoral fracture using an intramedullary unreamed nail, statically locked. 12 months after the surgical intervention an atrophic nonunion developed. The
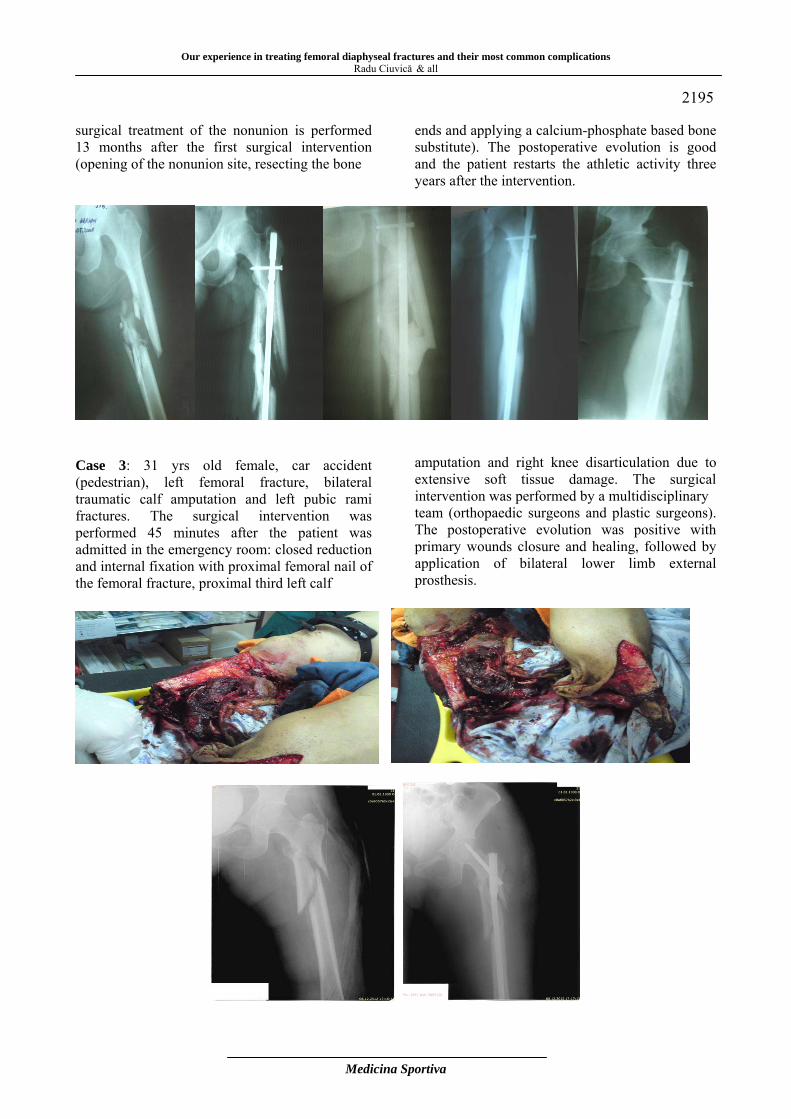
Our experience in treating femoral diaphyseal fractures and their most common complications Radu Ciuvică & all
Medicina Sportiva
2195 surgical treatment of the nonunion is performed 13 months after the first surgical intervention (opening of the nonunion site, resecting the bone
ends and applying a calcium-phosphate based bone substitute). The postoperative evolution is good and the patient restarts the athletic activity three years after the intervention.
Case 3: 31 yrs old female, car accident (pedestrian), left femoral fracture, bilateral traumatic calf amputation and left pubic rami fractures. The surgical intervention was performed 45 minutes after the patient was admitted in the emergency room: closed reduction and internal fixation with proximal femoral nail of the femoral fracture, proximal third left calf
amputation and right knee disarticulation due to extensive soft tissue damage. The surgical intervention was performed by a multidisciplinary team (orthopaedic surgeons and plastic surgeons). The postoperative evolution was positive with primary wounds closure and healing, followed by application of bilateral lower limb external prosthesis.
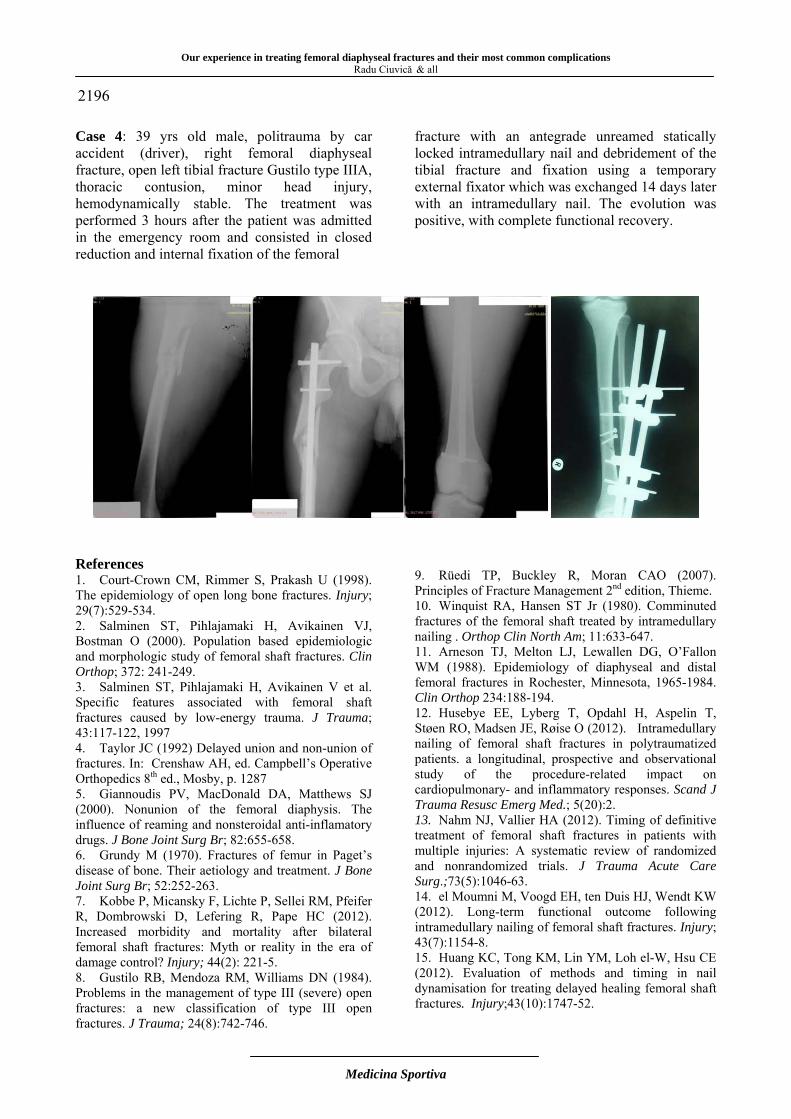
Our experience in treating femoral diaphyseal fractures and their most common complications
Radu Ciuvică & all
Medicina Sportiva
2196 Case 4: 39 yrs old male, politrauma by car accident (driver), right femoral diaphyseal fracture, open left tibial fracture Gustilo type IIIA, thoracic contusion, minor head injury, hemodynamically stable. The treatment was performed 3 hours after the patient was admitted in the emergency room and consisted in closed reduction and internal fixation of the femoral
fracture with an antegrade unreamed statically locked intramedullary nail and debridement of the tibial fracture and fixation using a temporary external fixator which was exchanged 14 days later with an intramedullary nail. The evolution was positive, with complete functional recovery.
References 1. Court-Crown CM, Rimmer S, Prakash U (1998). The epidemiology of open long bone fractures. Injury; 29(7):529-534. 2. Salminen ST, Pihlajamaki H, Avikainen VJ, Bostman O (2000). Population based epidemiologic and morphologic study of femoral shaft fractures. Clin Orthop; 372: 241-249. 3. Salminen ST, Pihlajamaki H, Avikainen V et al. Specific features associated with femoral shaft fractures caused by low-energy trauma. J Trauma; 43:117-122, 1997 4. Taylor JC (1992) Delayed union and non-union of fractures. In: Crenshaw AH, ed. Campbell’s Operative Orthopedics 8th ed., Mosby, p. 1287 5. Giannoudis PV, MacDonald DA, Matthews SJ (2000). Nonunion of the femoral diaphysis. The influence of reaming and nonsteroidal anti-inflamatory drugs. J Bone Joint Surg Br; 82:655-658. 6. Grundy M (1970). Fractures of femur in Paget’s disease of bone. Their aetiology and treatment. J Bone Joint Surg Br; 52:252-263. 7. Kobbe P, Micansky F, Lichte P, Sellei RM, Pfeifer R, Dombrowski D, Lefering R, Pape HC (2012). Increased morbidity and mortality after bilateral femoral shaft fractures: Myth or reality in the era of damage control? Injury; 44(2): 221-5. 8. Gustilo RB, Mendoza RM, Williams DN (1984). Problems in the management of type III (severe) open fractures: a new classification of type III open fractures. J Trauma; 24(8):742-746.
9. Rüedi TP, Buckley R, Moran CAO (2007). Principles of Fracture Management 2nd edition, Thieme. 10. Winquist RA, Hansen ST Jr (1980). Comminuted fractures of the femoral shaft treated by intramedullary nailing . Orthop Clin North Am; 11:633-647. 11. Arneson TJ, Melton LJ, Lewallen DG, O’Fallon WM (1988). Epidemiology of diaphyseal and distal femoral fractures in Rochester, Minnesota, 1965-1984. Clin Orthop 234:188-194. 12. Husebye EE, Lyberg T, Opdahl H, Aspelin T, Støen RO, Madsen JE, Røise O (2012). Intramedullary nailing of femoral shaft fractures in polytraumatized patients. a longitudinal, prospective and observational study of the procedure-related impact on cardiopulmonary- and inflammatory responses. Scand J Trauma Resusc Emerg Med.; 5(20):2. 13. Nahm NJ, Vallier HA (2012). Timing of definitive treatment of femoral shaft fractures in patients with multiple injuries: A systematic review of randomized and nonrandomized trials. J Trauma Acute Care Surg.;73(5):1046-63. 14. el Moumni M, Voogd EH, ten Duis HJ, Wendt KW (2012). Long-term functional outcome following intramedullary nailing of femoral shaft fractures. Injury; 43(7):1154-8. 15. Huang KC, Tong KM, Lin YM, Loh el-W, Hsu CE (2012). Evaluation of methods and timing in nail dynamisation for treating delayed healing femoral shaft fractures. Injury;43(10):1747-52.

Our experience in treating femoral diaphyseal fractures and their most common complications Radu Ciuvică & all
Medicina Sportiva
2197 16. Weber BG, Cech O (1976). Pseudarthrosis: pathology, biomechanics, therapy, results, Bern, Switzerland, Hans Huber. 17. Khanfour AA, Zakzouk SA (2012). Distal femur non-union after interlocked intramedullary nailing. Successful augmentation with wave plate and strut graft. Acta Orthop Belg;78(4):492-9. 18. Søjbjerg JO, Eiskjaer S, Møller-Larsen F (1990). Locked nailing of comminuted and unstable fractures of the femur. J Bone Joint Surg Br; 72:23-25. 19. Court-Brown CM, Quaba AA (1996). The relationship between plastic surgery and orthopaedic trauma surgery. In: Court-Brown CM, McQueen MM, Quaba AA eds. Management of Open Fractures, London, Martin Dunitz, 157-164. 20. Hak DG, Lee SS, Goulet JA (2000). Success of exchange reamed intramedullary nailing for femoral shaft nonunion or delayed union. J Orthop Trauma; 14:178-182. 21. Schwartz JT, Brumback RJ, Lakatos R et al (1989). Acute compartment syndrome of the thigh. J Bone Joint Surg Am; 71: 392-400. Corresponding author Radu Ciuvică Department of Orthopedics and Traumatology University of Medicine and Pharmacy Carol Davila Bucharest, Romania E-mail: [email protected] Received: March 20, 2013 Accepted: July 10, 2013

Medicina Sportiva (2013), vol. IX, no 3, 2198-2202 Romanian Sports Medicine Society
Beneficial effect of aerobic exercise and green tea on serum antioxidants Amani Sandyani S1, Erfani Karimzadeh Toosi A2, Sariri R3, Razmi N1 1Science and Research Branch, Islamic Azad University, Fars, Iran 2 Gastrointestinal and Liver Disease Research Center, Guilan University of Medical Sciences, Rasht, Iran 3Department of Biochemistry, University of Guilan, Rasht, Iran Abstract. Introduction. Production of free radicals is a natural process during various metabolic events. The process may be altered due to various internal and external factors. Increased antioxidant capacity is one of the responses of human body against attack of free radicals. Many factors may affect the antioxidant capacity with various potential values in health and disease. The aim of this study was assessment of antioxidant potential in plasma after aerobic exercise, consumption of green tea and combination of both. Material and Method. Three groups of 35 healthy women (mean age 30.1±1.5 years) entered the study. The first group was composed of those attending an aerobic training course, the second group agreed to drink 3 mugs of green tea a day and the last group agreed to do both tests. Their blood samples were collected three times during the study, i.e. beginning, after two weeks and at the end. Results. A significant increase in catalase activity and uric acid concentration together with decreased concentration of malondialdehyde was observed. Conclusions. Enhanced activity of antioxidants in plasma is the beneficial effect of aerobic exercise, green tea and, most interesting, synergism of both. Since production of malondialdehyde is marker of cell damage, its reduced concentration after the period of treatment is indicative of increased natural resistance of the body to free radical attack. Key words: serum antioxidants, malondialdehyde, aerobic exercise, green tea, health. Introduction Free radicals are reactive oxygen or nitrogen species, having unpaired electrons. Within a living organism, free radicals can produce harmful effects due to their tendency to react with proteins and DNA by absorbing their electrons. Production of free radicals is a natural process during various metabolic events. The process may be altered due to various internal and external factors. Increased antioxidant capacity is one of the responses of human body against attack of free radicals. Malondialdehyde (MDA) is a low molecular weight aldehyde that is formed due to the attack of oxidative species on polyunsaturated fatty acids present in the phospholipid structure of cell membrane. In the case of an imbalance between oxidants and antioxidants sever oxidative damage may be resulted. This condition includes oxidative modification of cellular macromolecules, induction of cell death by apoptosis or necrosis and structural tissue damage. Measurement of any alternation in the level of MDA, therefore, can be considered a valuable screening tool as a biomarker of oxidative damage (1). Thus, one of
the important aims of this research was to determining whether MDA serum levels are associated with health improving habits including regular exercise and supplementation with natural antioxidants. We assumed that MDA serum levels may be used as biomarkers to predict health status. The antioxidant system in human serum protects body form attack of free radicals. The system contains enzymatic and non-enzymatic mechanisms, both of which may change in response of external and internal factors. The most important antioxidant enzymes are catalase, peroxidase and superoxide dismutase. On the other hand, non-enzymatic antioxidants are smaller molecules such as ascorbic acid, a water soluble vitamin, and uric acid, the end product of purine catabolism. It has been recommended that to maintain cardio respiratory fitness a program of aerobic type exercise for 20-60 min, three to five times per week at intensities of 50-80% VO2max is necessary for healthy adults (2).
2198
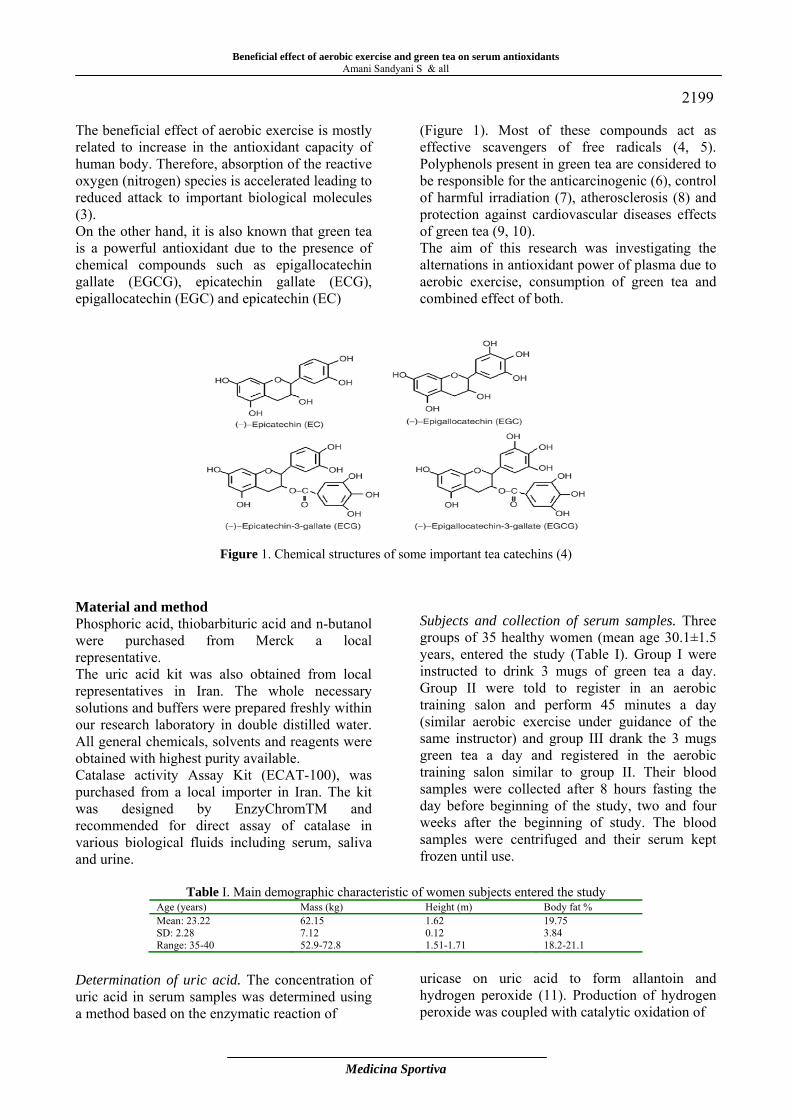
Beneficial effect of aerobic exercise and green tea on serum antioxidants Amani Sandyani S & all
Medicina Sportiva
2199 The beneficial effect of aerobic exercise is mostly related to increase in the antioxidant capacity of human body. Therefore, absorption of the reactive oxygen (nitrogen) species is accelerated leading to reduced attack to important biological molecules (3). On the other hand, it is also known that green tea is a powerful antioxidant due to the presence of chemical compounds such as epigallocatechin gallate (EGCG), epicatechin gallate (ECG), epigallocatechin (EGC) and epicatechin (EC)
(Figure 1). Most of these compounds act as effective scavengers of free radicals (4, 5). Polyphenols present in green tea are considered to be responsible for the anticarcinogenic (6), control of harmful irradiation (7), atherosclerosis (8) and protection against cardiovascular diseases effects of green tea (9, 10). The aim of this research was investigating the alternations in antioxidant power of plasma due to aerobic exercise, consumption of green tea and combined effect of both.
Figure 1. Chemical structures of some important tea catechins (4) Material and method Phosphoric acid, thiobarbituric acid and n-butanol were purchased from Merck a local representative. The uric acid kit was also obtained from local representatives in Iran. The whole necessary solutions and buffers were prepared freshly within our research laboratory in double distilled water. All general chemicals, solvents and reagents were obtained with highest purity available. Catalase activity Assay Kit (ECAT-100), was purchased from a local importer in Iran. The kit was designed by EnzyChromTM and recommended for direct assay of catalase in various biological fluids including serum, saliva and urine.
Subjects and collection of serum samples. Three groups of 35 healthy women (mean age 30.1±1.5 years, entered the study (Table I). Group I were instructed to drink 3 mugs of green tea a day. Group II were told to register in an aerobic training salon and perform 45 minutes a day (similar aerobic exercise under guidance of the same instructor) and group III drank the 3 mugs green tea a day and registered in the aerobic training salon similar to group II. Their blood samples were collected after 8 hours fasting the day before beginning of the study, two and four weeks after the beginning of study. The blood samples were centrifuged and their serum kept frozen until use.
Table I. Main demographic characteristic of women subjects entered the study Age (years) Mass (kg) Height (m) Body fat % Mean: 23.22 SD: 2.28 Range: 35-40
62.15 7.12 52.9-72.8
1.62 0.12 1.51-1.71
19.75 3.84 18.2-21.1
Determination of uric acid. The concentration of uric acid in serum samples was determined using a method based on the enzymatic reaction of
uricase on uric acid to form allantoin and hydrogen peroxide (11). Production of hydrogen peroxide was coupled with catalytic oxidation of
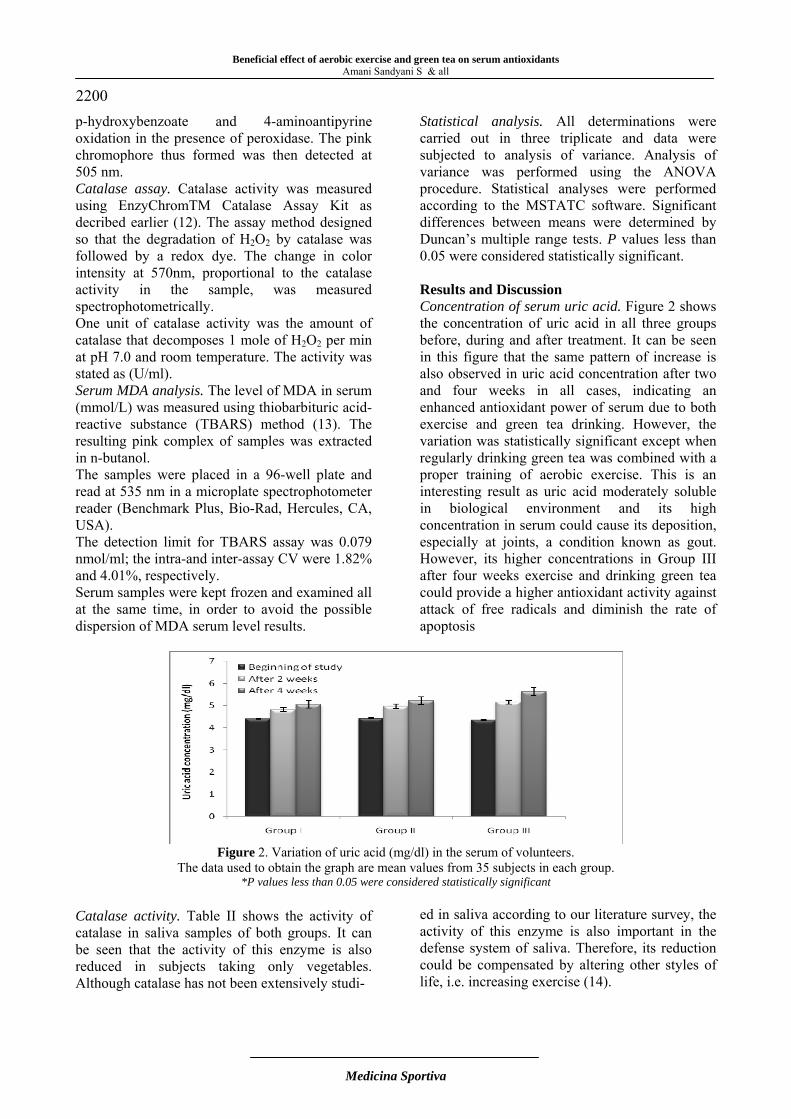
Beneficial effect of aerobic exercise and green tea on serum antioxidants
Amani Sandyani S & all
Medicina Sportiva
2200 p-hydroxybenzoate and 4-aminoantipyrine oxidation in the presence of peroxidase. The pink chromophore thus formed was then detected at 505 nm. Catalase assay. Catalase activity was measured using EnzyChromTM Catalase Assay Kit as decribed earlier (12). The assay method designed so that the degradation of H2O2 by catalase was followed by a redox dye. The change in color intensity at 570nm, proportional to the catalase activity in the sample, was measured spectrophotometrically. One unit of catalase activity was the amount of catalase that decomposes 1 mole of H2O2 per min at pH 7.0 and room temperature. The activity was stated as (U/ml). Serum MDA analysis. The level of MDA in serum (mmol/L) was measured using thiobarbituric acid-reactive substance (TBARS) method (13). The resulting pink complex of samples was extracted in n-butanol. The samples were placed in a 96-well plate and read at 535 nm in a microplate spectrophotometer reader (Benchmark Plus, Bio-Rad, Hercules, CA, USA). The detection limit for TBARS assay was 0.079 nmol/ml; the intra-and inter-assay CV were 1.82% and 4.01%, respectively. Serum samples were kept frozen and examined all at the same time, in order to avoid the possible dispersion of MDA serum level results.
Statistical analysis. All determinations were carried out in three triplicate and data were subjected to analysis of variance. Analysis of variance was performed using the ANOVA procedure. Statistical analyses were performed according to the MSTATC software. Significant differences between means were determined by Duncan’s multiple range tests. P values less than 0.05 were considered statistically significant. Results and Discussion Concentration of serum uric acid. Figure 2 shows the concentration of uric acid in all three groups before, during and after treatment. It can be seen in this figure that the same pattern of increase is also observed in uric acid concentration after two and four weeks in all cases, indicating an enhanced antioxidant power of serum due to both exercise and green tea drinking. However, the variation was statistically significant except when regularly drinking green tea was combined with a proper training of aerobic exercise. This is an interesting result as uric acid moderately soluble in biological environment and its high concentration in serum could cause its deposition, especially at joints, a condition known as gout. However, its higher concentrations in Group III after four weeks exercise and drinking green tea could provide a higher antioxidant activity against attack of free radicals and diminish the rate of apoptosis
Figure 2. Variation of uric acid (mg/dl) in the serum of volunteers.
The data used to obtain the graph are mean values from 35 subjects in each group. *P values less than 0.05 were considered statistically significant
Catalase activity. Table II shows the activity of catalase in saliva samples of both groups. It can be seen that the activity of this enzyme is also reduced in subjects taking only vegetables. Although catalase has not been extensively studi-
ed in saliva according to our literature survey, the activity of this enzyme is also important in the defense system of saliva. Therefore, its reduction could be compensated by altering other styles of life, i.e. increasing exercise (14).
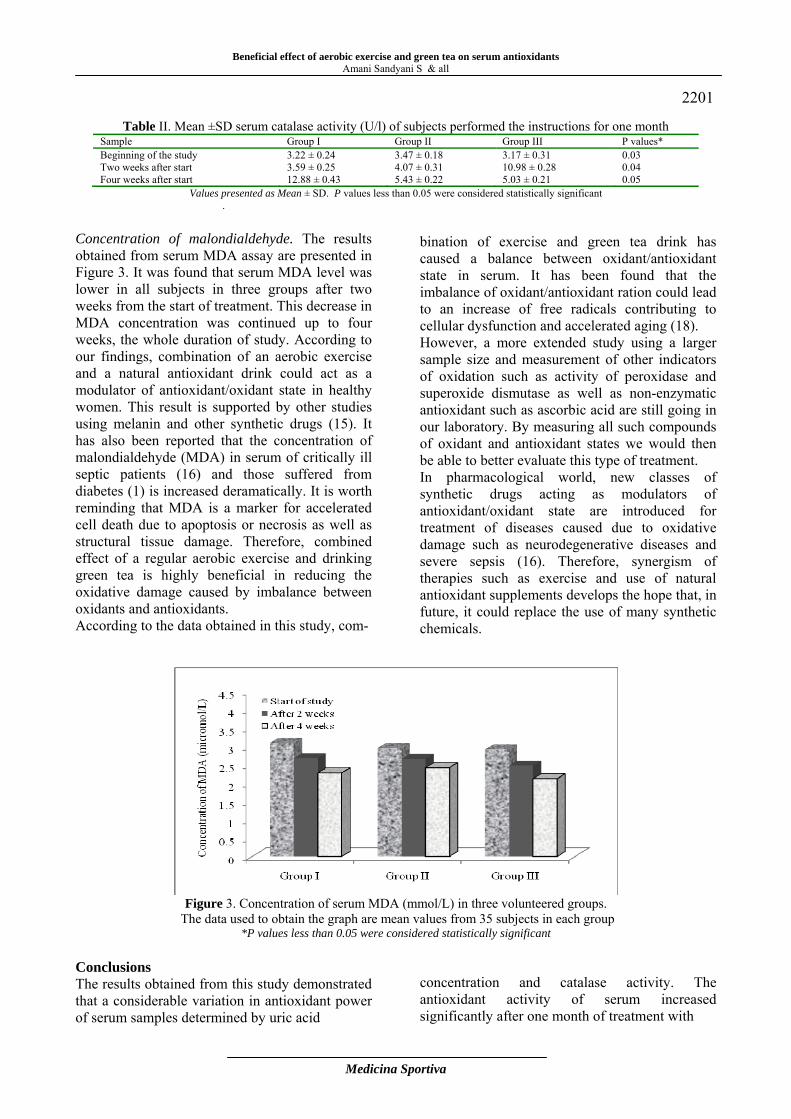
Beneficial effect of aerobic exercise and green tea on serum antioxidants Amani Sandyani S & all
Medicina Sportiva
2201
Table II. Mean ±SD serum catalase activity (U/l) of subjects performed the instructions for one month Sample Group I Group II Group III P values* Beginning of the study Two weeks after start Four weeks after start
3.22 ± 0.24 3.59 ± 0.25 12.88 ± 0.43
3.47 ± 0.18 4.07 ± 0.31 5.43 ± 0.22
3.17 ± 0.31 10.98 ± 0.28 5.03 ± 0.21
0.03 0.04 0.05
Values presented as Mean ± SD. P values less than 0.05 were considered statistically significant.
Concentration of malondialdehyde. The results obtained from serum MDA assay are presented in Figure 3. It was found that serum MDA level was lower in all subjects in three groups after two weeks from the start of treatment. This decrease in MDA concentration was continued up to four weeks, the whole duration of study. According to our findings, combination of an aerobic exercise and a natural antioxidant drink could act as a modulator of antioxidant/oxidant state in healthy women. This result is supported by other studies using melanin and other synthetic drugs (15). It has also been reported that the concentration of malondialdehyde (MDA) in serum of critically ill septic patients (16) and those suffered from diabetes (1) is increased deramatically. It is worth reminding that MDA is a marker for accelerated cell death due to apoptosis or necrosis as well as structural tissue damage. Therefore, combined effect of a regular aerobic exercise and drinking green tea is highly beneficial in reducing the oxidative damage caused by imbalance between oxidants and antioxidants. According to the data obtained in this study, com-
bination of exercise and green tea drink has caused a balance between oxidant/antioxidant state in serum. It has been found that the imbalance of oxidant/antioxidant ration could lead to an increase of free radicals contributing to cellular dysfunction and accelerated aging (18). However, a more extended study using a larger sample size and measurement of other indicators of oxidation such as activity of peroxidase and superoxide dismutase as well as non-enzymatic antioxidant such as ascorbic acid are still going in our laboratory. By measuring all such compounds of oxidant and antioxidant states we would then be able to better evaluate this type of treatment. In pharmacological world, new classes of synthetic drugs acting as modulators of antioxidant/oxidant state are introduced for treatment of diseases caused due to oxidative damage such as neurodegenerative diseases and severe sepsis (16). Therefore, synergism of therapies such as exercise and use of natural antioxidant supplements develops the hope that, in future, it could replace the use of many synthetic chemicals.
Figure 3. Concentration of serum MDA (mmol/L) in three volunteered groups.
The data used to obtain the graph are mean values from 35 subjects in each group *P values less than 0.05 were considered statistically significant
Conclusions The results obtained from this study demonstrated that a considerable variation in antioxidant power of serum samples determined by uric acid
concentration and catalase activity. The antioxidant activity of serum increased significantly after one month of treatment with
Beneficial effect of aerobic exercise and green tea on serum antioxidants
Amani Sandyani S & all
Medicina Sportiva
2202 aerobic training and drinking green tea. On the other hand, the decreased serum level of MDA, a marker of cell death, is indicative of higher resistance of cells to oxidative damage. Interestingly, it was found that both effects were more enhanced by combined treatment with exercise and green tea supplementation. It is, therefore, both health treatments could not only reduce MDA levels, but it also caused an increased in the levels of other antioxidant compounds uric acid and catalase. Therefore, based on the results obtained from the present study, it is generally concluded that the beneficial effect of aerobic exercise in terms of resistance to antioxidant attack considerably improved when a source of natural antioxidant is used as a food or drink supplement. Acknowledgements. The authors express their sincere thanks to University of Guilan for financial support. References 1. Mahreen R, Mohsin M, Nasreen Z, Siraj M, Ishaq
M (2010). Significantly increased levels of serum malonaldehyde in type 2 diabetics with myocardial infarction. Int J Diabetes Dev Ctries; 30: 49–51.
2. American College of Sport Medicine (2011). Position stand on the recommended quantity and quality of exercise for developing and maintaining cardio respiratory and muscular fitness in healthy adults. Med Sci Sports Exerc; 22: 265-274.
3. Afzalpour ME, Gharakhanlou R, Gaeini AA, Mohebbi H, Hedayati M, Khazaei M (2008). The effects of aerobic exercises on the serum oxidized LDL and total antioxidant capacity in non-active men CVD Prevention and Control; 3(2):77-82.
4. Salah N, Miller NJ, Parganga G, Tifburg L, Bolwell GP and Rice-Evan C (1995). Polyphenolic flavonols as scavengers of aqueous phase radicals and as chain-breaking antioxidants. Archives of Biochemistry and Biophysics; 322: 339-346.
5. Khan N, Mukhtar H (2013). Tea and health: Studies in humans Curr Pharm Des; 2013 Feb 19 (Epub ahead of print) PMID: 23448443.
6. Gu JW, Makey KL, Tucker KB, Chinchar E, Mao X, Pei I, Thomas EY, Miele L (2013). EGCG, a major green tea catechin suppresses breast tumor angiogenesis and growth via inhibiting the activation of HIF-1α and NFκB, and VEGF expression. Vasc Cell; 5(1): 9-16.
7. Davari H, Haddad F, Moghimi A, Farhad Rahimi M, Ghavamnasiri MR (2012). Study of Radioprotective Effect of Green Tea against Gamma Irradiation Using Micronucleus Assay on Binucleated Human Lymphocytes. Iran J Basic Med Sci; 15(5): 1026-31.
8. Cai Y, Kurita-Ochiai T, Hashizume T, Yamamoto
M (2013). Green tea epigallocatechin-3-gallate attenuates Porphyromonas gingivalis-induced atherosclerosis. Pathog Dis; 67(1): 76-83.
9. Kokubo Y, Iso H, Saito I, Yamagishi K, Yatsuya H, Ishihara J, Inoue M, Tsugane S (2013). The impact of green tea and coffee consumption on the reduced risk of stroke incidence in Japanese population: the Japan public health center-based study cohort. Stroke; 44(5): 1369-74.
10. Hertog MJL, Fresken EJM, Hollman PCH, Katan MB and Kromhout D (1993). Dietary antioxidative flavonoids and risk of coronary heart disease: the Zutphen Elderly Study Lancet; 342:1007-1011.
11. Giuseppe Lippi, Martina Montagnana, Massimo Franchini, Emmanuel J. Favaloro, Giovanni Targher (2008). The paradoxical relationship between serum uric acid and cardiovascular disease. Clinica Chimica Acta; 392(1-2):1-7.
12. Sariri R , Damirchi A, Nazari Y (2013). Salivary antioxidant variations in athletes after intense exercise. Medicina Sportiva (Romanian Sports Medicine Society); IX(1): 2043- 2050.
13. Kikugawa K, Kojima T, Yamaki S, Kosugi H (1992) Interpretation of the thiobarbituric acid reactivity of rat liver and brain homogenates in the presence of ferric ion and ethylediaminotetraacetic acid. Anal Biochem 202: 249-255.
14. Leff JA, Oppegard MA, Curiel TJ, Brown KS, Schooley RT, Repine JE (1992). Progressive increases in serum catalase activity in advancing human immunodeficiency virus infection. Free Radic Biol Med; 13(2): 143-9.
15. Sener G, Toklu H, Kapucu C, Ercan F, Erkanli G, et al. (2005). Melatonin protects against oxidative organ injury in a rat model of sepsis. Surg Today; 35: 52-59.
16. Lorente L, Martín MM, Abreu-González P, Domínguez-Rodríguez A, Labarta L, Díaz C, et al (2013). Prognostic value of malondialdehyde serum levels in severe sepsis: A multicenter study. PLoS One; 8(1): e53741.
17. Andrades ME, Morina A, Spasić S, Spasojević I: Bench-to-bedside review (2011) Sepsis from the redox point of view. Crit Care; 15:230-237.
18. Moustafa AH, Ali EM, Mohamed TM, Abdou HI (2009). Oxidative stress and thyroid hormones in patients with liver diseases. Eur J Intern Med; 20:703-708.
Corresponding author Sariri Reyhaneh Department of Biology, Gilan University Rasht, Iran Fax: +98 131 3220912 E-mail: [email protected] Received: May 31, 2013 Accepted: August 7, 2013

Medicina Sportiva (2013), vol. IX, no 3, 2203-2208 Romanian Sports Medicine Society
Posterolateral knee instability in patients with anterior cruciate ligament lesion - clinical and MRI evaluation (case presentation) Ion Bogdan Codorean1, Ioan Codorean 2, Stefan Mitulescu1, Eduard Cernat1
1Department of Orthopedics and Traumatology, University of Medicine and Pharmacy Carol Davila, Central Military Hospital, Bucharest, Romania 2Medical CenterMedas, Magnetic Resonance Department, Bucharest, Romania Abstract. This paper is a retrospective study between January 2007 - September 2012, and refers to a group of 1347 patients with acute or old traumatic injury, with instability of the knee (anteroposterior or combined) and Magnetic Resonance Imaging (MRI) examination showed isolated or associated lesions of anterior cruciate ligament (ACL). Out of 1347 patients a group of 117 (8.6%) patients was selected , in whom MRI examination revealed associated lesions to the stability structures from the postero-lateral compartment. The paper is showing the spectrum of lesions identified by MRI in the postero-lateral compartment and their correlation with the mechanism of injury and the data from the clinical exam and the special tests for the clinical assessment of rotational instability. The study will present statistics on identified injuries and their MRI images. The highest incidence of lesions that have generated rotational instability included the popliteal anatomical complex formed by the popliteofibular ligament, postero-lateral capsule, arcuate ligament, fabelofibular ligament, fibular collateral ligament, biceps femoris tendon and lateral gastrocnemius tendon. To be able to give fast and accurate diagnostic information to the surgeon, with therapeutic significance, to confirm or rule out the clinical diagnostic of posterolateral rotational instability requires a good knowledge of the anatomy of the posterolateral compartment being known the vast anatomical variation and the small dimension of these structures. Not being able to recognise and treat the posterolateral compartment lesions contribute to ACL reconstruction failure due to significantly increased forces that will stress the graft with varus loading at various degrees of flexion. Key words: knee instability, traumatic injury, Magnetic Resonance Imaging. Introduction Knee joint instability is due to acute or chronic, isolated or associated injuries of the stability structures represented by the anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), medial collateral ligaments, (MCL) and lateral collateral ligament (LCL) ilio-tibial tract (ITT) and capsular or noncapsulare components of posterolateral (PLC)and posteromedial compartments (PMC). The objective of this study is to present the diagnostic performance of MRI in confirming or rule out the presence of a lesional substrate in clinical suspicion of posterolateral rotatory instability in patients with ACL rupture requiring arthroscopic ligament reconstruction. Material and methods This paper is a retrospective study from January 2007 - September 2012 conducted in several imaging diagnostic centers in Bucharest, and refers to a group of 1347 patients with acute or cronic traumatic history, with instability of the
knee (anteroposterior or combined) and the MRI examination showed isolated or associated lesions of ACL.The images were acquired with different equipment, 3T Philips Achieva (293 patients) 1.5 T Philips Achieva (513 patients), 1.5 T GE (454 patients ) 1.5 T Toshiba (87 patients). Patients were examined by a protocol that included: - clinical examination - insisting on anamnesis to identify the mechanism of injury, physical examination, special clinical tests for posterolateral joint instability detection compared with the contralateral knee, Lachmann test, external rotation recurvatum test, posterolateral drawer test, varus stress testing and reverse pivot shift test. Results Table I presents the injury spectrum associated to medial and posteromedial compartments (PMC) in patients with total and partial rupture of the anterior cruciate ligament, MRI identified in patients in the study group.
2203
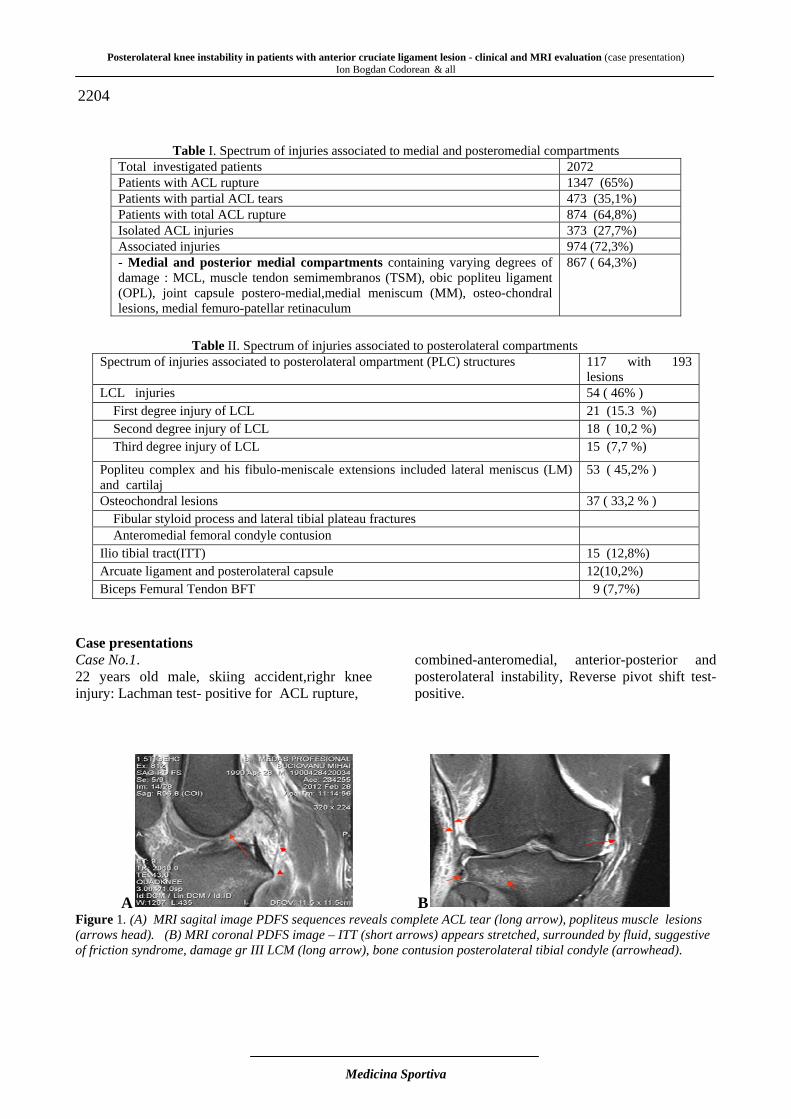
Posterolateral knee instability in patients with anterior cruciate ligament lesion - clinical and MRI evaluation (case presentation)
Ion Bogdan Codorean & all
Medicina Sportiva
2204
Table I. Spectrum of injuries associated to medial and posteromedial compartments
Total investigated patients 2072 Patients with ACL rupture 1347 (65%) Patients with partial ACL tears 473 (35,1%) Patients with total ACL rupture 874 (64,8%) Isolated ACL injuries 373 (27,7%) Associated injuries 974 (72,3%) - Medial and posterior medial compartments containing varying degrees of damage : MCL, muscle tendon semimembranos (TSM), obic popliteu ligament (OPL), joint capsule postero-medial,medial meniscum (MM), osteo-chondral lesions, medial femuro-patellar retinaculum
867 ( 64,3%)
Table II. Spectrum of injuries associated to posterolateral compartments
Spectrum of injuries associated to posterolateral ompartment (PLC) structures 117 with 193 lesions
LCL injuries 54 ( 46% ) First degree injury of LCL 21 (15.3 %) Second degree injury of LCL 18 ( 10,2 %) Third degree injury of LCL 15 (7,7 %)
Popliteu complex and his fibulo-meniscale extensions included lateral meniscus (LM) and cartilaj
53 ( 45,2% )
Osteochondral lesions 37 ( 33,2 % ) Fibular styloid process and lateral tibial plateau fractures Anteromedial femoral condyle contusion Ilio tibial tract(ITT) 15 (12,8%) Arcuate ligament and posterolateral capsule 12(10,2%) Biceps Femural Tendon BFT 9 (7,7%)
Case presentations Case No.1. 22 years old male, skiing accident,righr knee injury: Lachman test- positive for ACL rupture,
combined-anteromedial, anterior-posterior and posterolateral instability, Reverse pivot shift test- positive.
A B Figure 1. (A) MRI sagital image PDFS sequences reveals complete ACL tear (long arrow), popliteus muscle lesions (arrows head). (B) MRI coronal PDFS image – ITT (short arrows) appears stretched, surrounded by fluid, suggestive of friction syndrome, damage gr III LCM (long arrow), bone contusion posterolateral tibial condyle (arrowhead).
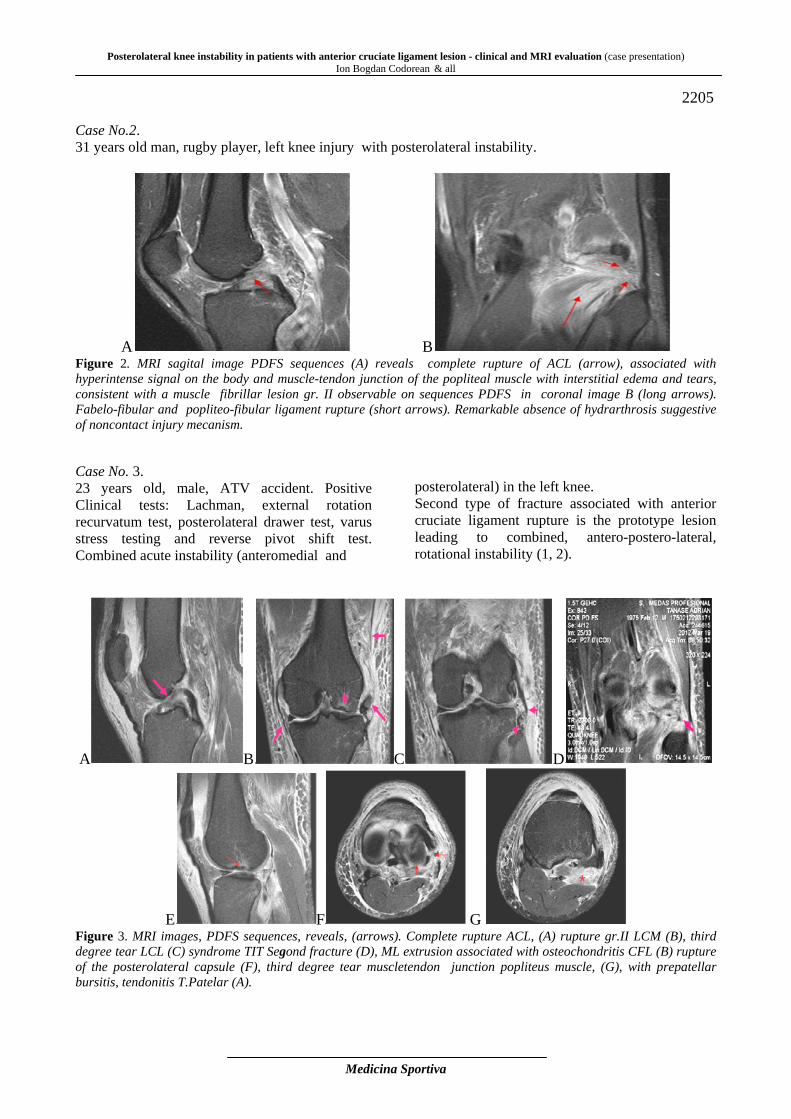
Posterolateral knee instability in patients with anterior cruciate ligament lesion - clinical and MRI evaluation (case presentation) Ion Bogdan Codorean & all
Medicina Sportiva
2205
Case No.2. 31 years old man, rugby player, left knee injury with posterolateral instability.
A B Figure 2. MRI sagital image PDFS sequences (A) reveals complete rupture of ACL (arrow), associated with hyperintense signal on the body and muscle-tendon junction of the popliteal muscle with interstitial edema and tears, consistent with a muscle fibrillar lesion gr. II observable on sequences PDFS in coronal image B (long arrows). Fabelo-fibular and popliteo-fibular ligament rupture (short arrows). Remarkable absence of hydrarthrosis suggestive of noncontact injury mecanism. Case No. 3. 23 years old, male, ATV accident. Positive Clinical tests: Lachman, external rotation recurvatum test, posterolateral drawer test, varus stress testing and reverse pivot shift test. Combined acute instability (anteromedial and
posterolateral) in the left knee. Second type of fracture associated with anterior cruciate ligament rupture is the prototype lesion leading to combined, antero-postero-lateral, rotational instability (1, 2).
A B C D
E F G Figure 3. MRI images, PDFS sequences, reveals, (arrows). Complete rupture ACL, (A) rupture gr.II LCM (B), third degree tear LCL (C) syndrome TIT Segond fracture (D), ML extrusion associated with osteochondritis CFL (B) rupture of the posterolateral capsule (F), third degree tear muscletendon junction popliteus muscle, (G), with prepatellar bursitis, tendonitis T.Patelar (A).

Posterolateral knee instability in patients with anterior cruciate ligament lesion - clinical and MRI evaluation (case presentation)
Ion Bogdan Codorean & all
Medicina Sportiva
2206 Case No 4. 27 years old male, football player.IRM examination 7 days after a knee injury with swelling, pain on the lateral side, positive Lachman test, anterior-posterior instability and posterolateral instability.
Popliteus muscle is the primary lateral stabilizer of the knee. Stress forcing with lateral rotation of the tibia can seriously affect the popliteal tendon, which usually breaks at the muscle-tendon junction. (3,4)
A
Figure 4. MRI images, PDFS, sagittal (A), coronal (B), interruption of continuity ACL, and hyperintensity signal on the body and muscle-tendon junction of the popliteus muscle (A, arrows.). In image B is distinguished the erased fibrillar drawing trough hemorrhagic fluid infiltration of the popliteal muscle (long arrow). It is visible also the entire trajectory of the lateral collateral ligament in a single image suggestive of anterior translation of the tibia(.short arrow). Discussion The rotational instability of the posterolateral compartment of the knee is a complex and challenging entity both in terms of diagnosis and treatment (3). Posterolateral compartment structures include both static and dynamic stabilizers. Ilio-tibial tract (TIT), biceps tendon, (TB) lateral head of the gastrocnemius muscle (CLMGnM) and popliteus muscle (MpopL) are dynamic stabilizers. Lateral collateral ligament (LCL), arcuate ligament, (LARC)) fabelo-fibular ligament (LFF) and popliteo-fibular ligament (PFL) are the static stabilizers). Biomechanical studies have shown that static stabilizers cooperate to limit the posterior tibial displacement, rotation and varus tibial external rotation. PLC knee injuries are uncommon but can result if not treated properly in chronic disability due to cartilage degeneration and osteoarthritis (4). Isolated posterolateral compartment lesions rarely occur, most commonly they are associated with ACL, PCL tears and tibial plateau fractures (5). MR imaging is currently the technique of choice for viewing posttraumatic lesions of the stability structures of the knee (4, 6, 7). In our study MRI showed the ACL tear peripheral compartments of the knee). In our study MRI showed ACL tears from the peripheral compartments of the knee. Thus out of 974 injuries associated with ACL ruptures, MRI examination revealed lesions of the medial and
posterior medial compartment in various degrees of injury including: medial collateral ligament (MCL), semimembranosus tendon (TMS), oblique popliteal ligament (LOP) , posteromedial joint capsule (CapsPM,) medial meniscus (MM), osteo-chondral lesions, (LOC) the medial retinaculum (RetM) 867 (64.3%). Concomitant lesions to the posterolateral compartment structures was identified in 117 patients (8.6%), showing damage in two or more of the posterolateral structures, the most important in terms of stability is represented by the lateral collateral ligament (LCL) representing 46%; lateral meniscus (ML); muscle-tendon popliteal unit (UMTPopl) including popliteofibular ligament (LPopl F) and posterolateral joint capsule (Caps PL) to 45.2% and osteochondral injuries including Segond fractures and fractures of the fibular styloid process have represented 33.2%. In 17% of the patients the injuries were caused by direct trauma to the proximal anteromedial and posteromedial region of the tibia with the knee close to full extension; in 67% of the patients the lesions were produced by indirect mechanism (hyperextension and external rotation); in 16% of cases the mechanism was complex comprising a combination of forces (varus with hyperextension or varus with direct trauma to the posterior proximal tibia with the knee flexed - dashboard injury. The injuries were due to a particular type of
B
Posterolateral knee instability in patients with anterior cruciate ligament lesion - clinical and MRI evaluation (case presentation) Ion Bogdan Codorean & all
Medicina Sportiva
2207 direct or indirect forces, or a combination, and occurred in team sports like football, handball, rugby, basketball involving an abrupt change in direction of motion, a strong and extended contact between players and in individual sports like skiing, tennis, recreational. The lesions responsible for instability were correlated with clinical diagnosis, stability tests and arthroscopic findings. Clinical symptoms varied with the intensity of the trauma, the degree of instability and the association of lesions from other compartments. Patients with acute trauma presented with pain and swelling of the posterolateral region of the knee. After the pain and the swelling have subsided, patients experienced signs of instability at the objective clinical examination in hyperextension or varus. Patients with chronic PLC injuries complained of pain at the medial joint line compression and / or lateral, and at the palpation of the posterolateral knee aspect; signs of chronic instability felt when climbing and descending stairs. We evaluated the asymmetry in external rotation of the tibia through the dial test. The test was performed at both 30° and 90° of knee flexion. The increased amplitude of the external rotation at 30°, compared to the 90° of knee flexion may indicate an isolated lesion of the posterolateral compartment, while broader external rotation at both 30° and 90° indicate a lesion both PLC and posterior cruciate ligament (PCL), an increase of 10° from the normal considered significant.. We emphasize the need for early diagnosis of these PCL associated lesions for the primary repair, rather than delayed reconstruction. The failure to recognize and treating a PCL injury only by ACL reconstruction is the major cause of revisions surgery. In a study of 66 patients with ACL reconstruction, 24% of the failures were attributable to unrecognized preoperative lateral laxity. Biomechanical studies have shown that the posterior laxity increases the stress experienced by the graft used in ACL reconstruction (8). Conclusions In our study, the damage of PLC structures in patients with ACL ruptures is having a much lower incidence (8.6%) compared with injuries of the medial compartment (64.3%), but these injuries are more debilitating, requiring reparatory or reconstruction surgery. In acute trauma cases, clinical symptomatology is "covered" by the clinical signs of highly severe concomitant lesions , clinical tests in assesing stability in external rotation and varus stress,
performed in different degrees of flexion is difficult to perform.MRI is the technique of choice in pre-operative identification of traumatic lesions of the ACL and anatomical structures of PLC as well as postoperative management. To perform an accurate assessment of injuries , it requires a good knowledge of PLC anatomical structures being known the vaste anatomical variations and the small dimensions of this structures.Knowing the anatomy and the normal and pathologic MRI appearance of posterolateral horn structures of the knee in patients with ACL rupture and rotatory instability, the radiologist provides important diagnostic data by highlighting the damaged structures. The failure in recognizing and treatment of PCL injuries of chronic posterolateral rotatory instability is considered the most common cause of graft failure in ACL reconstruction. References
1. Nicholas JA. (1973). The Five-One Reconstruction for Anteromedial Instability of the Knee Indications, Technique, and the Results in fifty-two patients J Bone Joint Surg Am; 55(5): 899-922.
2. RecondoJA, Salvador E, Villanua JA, Barrera MC, Gervas C, Alustiza JM (2000). Lateral stabilizing structures of the knee: functional anatomy and injuries assessed with MR imaging. RadioGraphics; 20(spec issue): 91–102.
3. Emily N. Vinson, Nancy M. Major and Clyde A. Helms (2008). The Posterolateral Corner of the Knee. American Journal of Roentgenology; 190(2): 449-458.
4. Hywel Davies, Andrew Unwin and Paul Aichroth(2004), The posterolateral corner of the knee. Anatomy, biomechanics and management of injuries Injury; 35(1): 68-75.
5. Eric T. Ricchetti, Brian J. Sennett, ; G. Russell Huffman, (2008). Acute and Chronic Management of Posterolateral Corner Injuries of the Knee Orthopedics; 31(5): 121-127.
6. David A. Pacholke , Clyde A. Helms (2007), MRI of the posterolateral corner injury: A concise review. Journal of Magnetic Resonance Imaging Volume 26,(2): 250–255
7. Fanelli GC, Orcutt DR, Edson CJ (2005). The multiple-ligament injured knee: evaluation, treatment, and results. Arthroscopy; 21(7): 471 –486.
8. Codorean BI, Codorean I, Toma GS (2009). MRI in the diagnosis of ACL injury and associated lesions. Medicina Sportiva (Romanian Sports Medicine Journal); 5(4):1183-1191.
Posterolateral knee instability in patients with anterior cruciate ligament lesion - clinical and MRI evaluation (case presentation)
Ion Bogdan Codorean & all
Medicina Sportiva
2208
9. Harner CD, Vogrin TM, Hoher J, Ma CB, Woo SL. (2000); Biomechanical analysis of a posterior cruciate ligament reconstruction. Deficiency of the posterolateral structures as a cause of graft failure. Am J Sports Med.; 28(1): 32–39.
Corresponding author Ion Bogdan Codorean Department of Orthopedics and Traumatology University of Medicine and Pharmacy Carol Davila Central Military Hospital Bucharest, Romania E-mail: [email protected] Phone: 040722232555 Received: May 29, 2013 Accepted: August 10, 2013
AUTHORS INDEX
Apostol Adela 2147 Amani Sandyani S 2198 Berteanu Mihai 2147 Bordianu Anca 2191 Cem Cetin 2185 Cernat Eduard 2203 Ciuvică Radu 2191 Codorean Ioan 2203 Codorean Ion Bogdan 2203 Cristea Ştefan 2191 Elys Costa de Sousa 2171 Erfani Karimzadeh Toosi A 2166 Erfani Karimzadeh Toosi A 2198 Fabiana Tenório 2171 Halil İbrahim Kaya 2185 Ionescu Anca Mirela 2147, 2191 Levent Özçakar 2160 Michelle Vasconcelos de Oliveira 2171 Mitulescu Stefan 2203 Mustafa Hilmi Demir 2185 Mustafa Onur Serbest 2175 Nesrin Yağci 2160 Ojoawo Adesola O 2177 Oni Michael, 2177 Popoola O 2177 Razmi N 2198 Rezaei A 2166 Sabriye Ercan 2185 Sariri Kh R 2166 Sariri R 2198 Senem Güner 2160 Uğur Cavlak 2160 Vanessa Carla Monteiro 2171 Vasilescu Mirela 2147, 2191
JOURNAL STRUCTURE Medicina Sportiva is the journal of Romanian Sports Medicine Society and including: editorials, guides articles, original papers, clinical studies, news in sport medicine. The articles are submitted electronically to Editor-in-Chief or Managing Editor. Manuscripts are considered if they are submitted only to Medicina Sportiva and therefore should not be under consideration for publication elsewhere, either in part or in whole. Only the authors are responsible for the scientific context and legal aspects of the articles. Editors may make necessary changes to articles in accordance with guidelines for authors. Guidelines for authors All manuscripts must be submitted in English. Guides articles. Content: the article must to include theoretical and practical aspects that must to be report to actual researches in sport medicine. Size: the article must to have no more then 12 pages. Format: the text must to be compact and can has few subtitles. Original papers. Content: original papers must to include fundamentals research and clinical research regarding diagnostic and treatment. Size: 8-10 pages, 4-5 imagining documents (graphics, images, etc.). Format: the text must to be structure in introduction (present stage of the research), aim and scope of study, material and method, results, discussion, conclusions (must to present personal conclusions). Case reports. Content: clinical aspects and research that can show new ways and conclusions regarding morphologic evaluation and clinic assessment, therapeutic conclusions and evolution. Size: 3-5pages, 1-2 original demonstrations and researches. Format: case report, discussion and comparative study in report with actualities studies. Organization of the manuscript Each manuscript should follow the sequence: Title, Abstract and Keywords, Main text (Introduction, Methods, Results, Discussion), Acknowledgements, References, Tables, Figures, Graphics and Schemes (with captions). Tables, Figures and Schemes are to be typed on separate pages at the end of the manuscript. Ensure that each illustration or table has a caption attached, which should comprise a brief title and a description. Explain all symbols and abbreviations used. Do not imbed figures or tables into the text. The tables, figures and schemes must be in the final published size, not oversized. Illustrations and tables that have appeared elsewhere must be accompanied by written permission to reproduce them from the original publishers. This is necessary even if you are an author of the borrowed material. Borrowed material should be acknowledged in the captions in the exact wording required by the copyright holder. If not specified, use this style: “Reproduced by kind permission of . . . (publishers) from . . . (reference)”. Identifiable clinical photographs must be accompanied by written permission from the patient. Text style of the manuscript All manuscripts must to be edited in MS Word: - page setup format A4, margins at 2cm on all sides; - font style Times New Roman, without capital letter, size=14 for title (bold), 12 for authors (regular), 12 for affiliation (italic) 10 for abstract (regular), 10 for key words (italic), 11 for main text and (regular), 10 for references (regular, except the title of books and journals which will be written italic). - paragraph: indentation = 0, alignment left for title, authors, affiliation, key words and justified for abstract, main text , acknowledgements and references ; line spacing = single, column = one. Title: should be simple, concise and informative. Capitalize the first word only. Author names should appear as used for conventional publication, with first and middle names or initials followed by surname. If multiple authors have the same affiliation, one listing of the affiliation should be used, preceded by the full list of those authors on the line above. Addresses of corresponding authors should contain all information necessary for an effective correspondence (postal addresses, e-mail, fax and telephone number). Abstract: begin the section with the word Abstract in bold font. The authors prepare a structured abstract of not more than 300 words. The abstract should be an explicit summary of the paper and must include (at least) four headings: aim, methods, results, conclusion. Immediately after the abstract, provide a maximum of 3–6 keywords, preferably taken from Index Medicus or Excerpta Medica Index. Acknowledgments: Acknowledgments should be included before the References section. References: in the text identify references by Arabic numeral in brackets, using Oxford system. The list of references should include only those publications witch are cited in the text. References should be presented in consecutive order as they are cited in the text. References should be cited in the text by placing sequential numbers in brackets (for example, (1), (3-5) ). The first six authors should be presented. Examples: a) Journals: name of authors, initial of surname, years of publish in brackets, title of paper, title of periodical (italic), volume, page (Ryder, JW, Bassel Duby R, Olson EN, Zierath, JR (2003). Skeletal muscle reprogramming by activation of calcineurin improves insulin action on metabolic pathways. J. Biol. Chem. 278, 298 304); b) Books: name of authors, years of publish in brackets, title of papers or capitol, title of book or monograph (italic), editors, city, pages (Booth FW, Baldwin KM (1995). Muscle plasticity: energy demanding and supply processes. In: Handbook of physiology. Rowell LB, Shepherd JT (eds). Oxford University Press, New York, pp 1076-1121). c) Proceedings: name of authors, initial of surname, years of publish in brackets, title of paper, title of periodical (italic), editors, city, pages. Manuscripts are welcomed from all countries, and may be submitted for consideration on the understanding that they have not been previously published elsewhere, either in print or electronically, and that they are not under consideration
by any other publisher. Authors wishing to include figures or text passages that have already been published elsewhere are required to obtain permission from the copyright holder(s) and to include evidence that such permission has been granted when submitting their papers. Authors are required to ensure that no material submitted as part of a manuscript infringes existing copyrights, or the rights of a third party. The author who submits the manuscript for publication should ensure that all coauthors are included on the paper, and that all coauthors have seen the final version of the article and have agreed to its submission for publication. Research carried out on humans must be in compliance with the Helsinki Declaration, adopted by the 18th World Medical Assembly, Helsinki, Finland, June 1964 and any experimental research on animals must follow internationally recognized guidelines. By submitting a manuscript to our journal, each author explicitly confirms that the manuscript meets the highest ethical standards for authors and coauthors. The manuscript should contain a statement that has been approved by the appropriate ethical committees related to the institution(s) in which it was performed and that subjects gave informed consent to the work. Studies involving experiments with animals must state that their care was in accordance with institution guidelines. Patients' and volunteers' names, initials, and hospital numbers should not be used. In a case report, the subject's written consent should be provided. It is the author's responsibility to ensure all appropriate consents have been obtained. Patients have a right to privacy. Therefore identifying information, including patients images, names, initials, or hospital numbers, should not be included in videos, recordings, written descriptions, photographs, and pedigrees unless the information is essential for scientific purposes and you have obtained written informed consent for publication in print and electronic form from the patient (or parent, guardian or next of kin where applicable). If such consent is made subject to any conditions, Universitaria Publisher must be made aware of all such conditions. Written consents must be provided to Universitaria Publisher on request. Even where consent has been given, identifying details should be omitted if they are not essential. If identifying characteristics are altered to protect anonymity, such as in genetic pedigrees, authors should provide assurance that alterations do not distort scientific meaning and editors should so note. If such consent has not been obtained, personal details of patients included in any part of the paper and in any supplementary materials (including all illustrations and videos) must be removed before submission. Any material received without such evidence will be assumed to originate from the authors. The responsibility is only of the authors. Upon receipt of a manuscript the editor will notify the corresponding author that the submission has been received. Received manuscripts are first examined by the Medicina Sportiva editors. Manuscripts with insufficient priority for publication are rejected. Manuscripts not prepared in the advised style will be sent back to authors without scientific review. The manuscript will undergo a blinded review process. Under this process the editor will forward (electronically) the manuscript to two independent reviewers, members of the Scientific Board. After the review process has been completed the main author will be notified via e-mail either of acceptance, revision or rejection of the manuscript. If revision was recommended, this should be completed and returned to the editor within 4 weeks. Authors' rights As an author you (or your employer or institution) may do the following: •make copies (electronic) of the article for your own personal use, including for your own classroom teaching use •present the article at a meeting or conference and to distribute copies of the article to the delegates attending such a meeting •for your employer, if the article is a “work for hire”, made within the scope of your employment, your employer may use all or part of the information in the article for other intra-company use (e.g., training) •retain patent and trademark rights and rights to any processes or procedure described in the article •include the article in full or in part in a thesis or dissertation (provided that this is not to be published commercially) •use the article or any part thereof in a printed compilation of your works, such as collected writings or lecture notes (subsequent to publication of your article in the journal) •prepare other derivative works, to extend the article into book-length form, or to otherwise re-use portions or excerpts in other works, with full acknowledgement of its original publication in the journal Submission of articles and papers Authors are encouraged to submit their manuscripts via e-mail to: - Editor in Chief: Vasilescu Mirela, e-mail: medsprt @yahoo.com