MECILLINAM
1
337 gia, abdominal pain, and glomerulonephritis.2,3 Such patients usually have complement disorders and raised erythro- cyte-sedimentation rates. We found no haematological abnor- malities, serum cryoglobulins, or evidence of systemic disease in any of our patients whose serum-complement (C3) levels were normal (six patients) or slightly raised (two patients). The presence of neutrophils and eosinophils in the inflammatory infiltrate after multiple cold challenge is of espec- ial interest because chemotactic factors for eosinophils4 and neutrophils’ have previously been found in venous blood from urticated skin following cold challenge in cold urticaria. Cold urticaria is an expression of an immediate hypersensi- tivity reaction in which histamine is thought to be the major inflammatory mediator.6 Vasculitis has not previously been de- scribed as a feature of essential acquired cold urticaria, so its arousal by repeated cold challenge in our patients presumably reflects sustained injury to small cutaneous blood vessels. Whether this injury is due mainly to pharmacological or to im- munological processes or to a mixture of both needs further clarification. Institute of Dermatology, London E9 6BX R. A. J. EADY M. W. GREAVES MECILLINAM SIR,-Our experience of the activity of mecillinam against gram-negative bacilli has been less favourable than that of Dr Chattopadhyay and Dr Thomas (Jan. 28, p. 214). Our methods were very similar, except for the use of ’Iso-sensitest’ agar (Oxoid) and a standardised inoculum of 105 colony-form- ing units of bacteria. When mecillinam was tested against ampicillin (and amoxycillin) resistant enterobacteria its acti- vity was comparable with that of carbenicillin, but it was less active than seven cephalosporins and cefoxitin (see table). We studied 87 recent isolates from urines and 11 from wounds; all were from different patients with no epidemiological connec- tion. We did not observe the bimodal distribution of mecillinam susceptibilities reported by Chattopadhyay and Thomas who IN-VITRO SUSCEPTIBILITY OF 98 AMPICILLIN-RESISTANT GRAM-NEGATIVE BACILLI TO BETA-LACTAM ANTIBIOTICS * Susceptible to 10 mg/l of antibiotic (except for carbenicillin 50 mg/1). t Results with cephalothin, cephalexin, cephradine, cephazolin, cefur- oxime, cefoxitin, and cefamandole were similar in these conventional tests. 117 were P. mirabilis. found minimum inhibitory concentrations (M.!.c.s) either between 0.1 and 1 mg/1 or 100 mg/1 and above. When test sys- tems were used which allowed bacteria to enter the logarithmic growth phase and produce p4actamases before encountering 2. Soter, N. A., Austen, K. F., Gigli, I. J. invest. Derm. 1974, 63, 485. 3. Soter, N. A. New Engl. J. Med. 1977, 296, 1440. 4. Soter, N. A., Wasserman, S. I., Austen, K. F. ibid. 1976, 294, 698. 5. Wasserman, S. I., Soter, N. A., Center, D. M., Austen, K. F. J. clin. Invest. 1977, 60, 189. 6. Kaplan, A. P., Gray, L., Shaff, R. E., Horakova, Z., Beaven, M. A. J., Allergy clin. Immun. 1975, 55, 394. the antibiotic’ mecillinam (carbenicillin and cephaloridine, cephalothin, cephazolin, and cefamandole) was partially inac- tivated, and all six antibiotics were very vulnerable to P4acta- mase preparations, including the clinically important enzyme from Escherichia coli (TEM)2 This susceptibility can be corre- lated with a large-inoculum effect, which is most striking with mecillinam. Enzyme susceptibility and inoculum effect were minimal with cephradine, cefuroxime, and cefoxitin, while cephalexin gave intermediate values. Despite our disappointment with the antibacterial activity of mecillinam, and its vulnerability to &bgr;-lactamases, the anti- biotic’s unusual mode of action, discussed in your editorial of Feb. 4 (p. 252), is of great interest. Unlike other p-lactam agents, it converts gram-negative rods to large osmotically stable round or oval cells, over a wide range of concentrations. This effect is probably due-at least in E.coli-to the affinity of the antibiotic for the type 2 "penicillin-binding protein" only, which seems to have the extraordinarily specific function of producing transpeptidation (a final stage in cell-wall synthe- sis) at the "corners" of the bacterial cell. This uniquely re- stricted effect of mecillinam is complementary to the action of other p-lactam antibiotics that inhibit cell-wall synthesis at dif- ferent sites. On this basis, the combination of mecillinam with other p-lactam agents would be expected to be synergistic, and indeed this is often the case both in vitro and in vivo, notably with amoxycillin or cephradine.4 There are, nevertheless, im- portant economic implications if combinations of expensive antibiotics come into widespread use in the future. Gifts of mecillinam, cefoxitin, cefuroxime, and cefamandole were received from Leo Laboratories, Merck Sharp and Dohme, Glaxo Laboratories, and Eli Lilly and Co., respectively. Department of Bacteriology, Westminster Medical School, London SW1P 2AR M. BAKHTIAR S. SELWYN *** A line was dropped from our mecillinam editorial last week (restored in American edition). The second sentence was meant to say: "Other penicillins are synthesised from aminopenicil- lanic acid; mecillinam is derived from amidinopenicillanic acid, and its antibacterial spectrum is different."—ED. L BACTERIAL OVERGROWTH SYNDROME AFTER ACUTE NONSPECIFIC DIARRHŒA SIR,-In support of the findings of Roberts et a1.5 we have recently seen two patients (male aged 49, female aged 67) with bacterial overgrowth syndrome following acute nonspecific diarrhoea. Each had travelled to Mexico where they had an acute episode of watery diarrhoea (8-10 bowel movements/day) which lasted for five days and then became chronic (3-5 un- formed stools/day and weight loss). The patients were seen by us 1 month and 3 months respectively after the initial episode. There was no anatomical abnormality. Infectious diarrhoea was ruled out because stool culture for Shigella, Salmonella, enterotoxigenic Eschericia coli (heat-labile or heat-stable- toxin-producing) and Vibrio parahcemolyticus was negative. No ova or parasites were seen in the stool preparation. There was no significant antibody titre to heat-labile toxin of entero- toxigenic E. coli. colonisation factor of E. coli H-10407 was negative. Duodenal biopsy was normal and Giardia lamblia was absent both by direct observation and by routine his- tology. In duodenal aspirates, a pure culture of Pseudomonas (108 colonies/ml) was recovered from patient 1 and Entero- bacter (106 colonies/ml) and a-Streptococcus (102 colonies/ml) from patient 2. 1. Bakhtiar, M., Selwyn, S. Proc. 10th int. Chemother. Congr. (in the press). 2. Selwyn, S. J. antimicrob. Chemother. 1977, 3, 161. 3. Spratt, B. G. ibid. 1977, 3, suppl. B, p. 13. 4. Kerry, D. W., Hamilton-Miller, J. M. T., Brumfitt, W. ibid. 1977, 3, Suppl. B, p. 53. 5. Roberts, S. H., James, O., Jarvis, E. H. Lancet, 1977, ii, 1193.
Transcript of MECILLINAM

337
gia, abdominal pain, and glomerulonephritis.2,3 Such patientsusually have complement disorders and raised erythro-cyte-sedimentation rates. We found no haematological abnor-malities, serum cryoglobulins, or evidence of systemic diseasein any of our patients whose serum-complement (C3) levelswere normal (six patients) or slightly raised (two patients). Thepresence of neutrophils and eosinophils in the inflammatoryinfiltrate after multiple cold challenge is of espec-ial interest because chemotactic factors for eosinophils4 andneutrophils’ have previously been found in venous blood fromurticated skin following cold challenge in cold urticaria.
Cold urticaria is an expression of an immediate hypersensi-tivity reaction in which histamine is thought to be the majorinflammatory mediator.6 Vasculitis has not previously been de-scribed as a feature of essential acquired cold urticaria, so itsarousal by repeated cold challenge in our patients presumablyreflects sustained injury to small cutaneous blood vessels.Whether this injury is due mainly to pharmacological or to im-munological processes or to a mixture of both needs furtherclarification.
Institute of Dermatology,London E9 6BX
R. A. J. EADYM. W. GREAVES
MECILLINAM
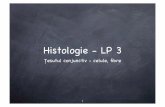
SIR,-Our experience of the activity of mecillinam againstgram-negative bacilli has been less favourable than that of DrChattopadhyay and Dr Thomas (Jan. 28, p. 214). Ourmethods were very similar, except for the use of ’Iso-sensitest’agar (Oxoid) and a standardised inoculum of 105 colony-form-ing units of bacteria. When mecillinam was tested againstampicillin (and amoxycillin) resistant enterobacteria its acti-vity was comparable with that of carbenicillin, but it was lessactive than seven cephalosporins and cefoxitin (see table). Westudied 87 recent isolates from urines and 11 from wounds; allwere from different patients with no epidemiological connec-tion.We did not observe the bimodal distribution of mecillinam
susceptibilities reported by Chattopadhyay and Thomas who
IN-VITRO SUSCEPTIBILITY OF 98 AMPICILLIN-RESISTANTGRAM-NEGATIVE BACILLI TO BETA-LACTAM ANTIBIOTICS
* Susceptible to 10 mg/l of antibiotic (except for carbenicillin 50mg/1).t Results with cephalothin, cephalexin, cephradine, cephazolin, cefur-oxime, cefoxitin, and cefamandole were similar in these conventionaltests.
117 were P. mirabilis.
found minimum inhibitory concentrations (M.!.c.s) eitherbetween 0.1 and 1 mg/1 or 100 mg/1 and above. When test sys-tems were used which allowed bacteria to enter the logarithmicgrowth phase and produce p4actamases before encountering
2. Soter, N. A., Austen, K. F., Gigli, I. J. invest. Derm. 1974, 63, 485.3. Soter, N. A. New Engl. J. Med. 1977, 296, 1440.4. Soter, N. A., Wasserman, S. I., Austen, K. F. ibid. 1976, 294, 698.5. Wasserman, S. I., Soter, N. A., Center, D. M., Austen, K. F. J. clin. Invest.
1977, 60, 189.6. Kaplan, A. P., Gray, L., Shaff, R. E., Horakova, Z., Beaven, M. A. J.,
Allergy clin. Immun. 1975, 55, 394.
the antibiotic’ mecillinam (carbenicillin and cephaloridine,cephalothin, cephazolin, and cefamandole) was partially inac-tivated, and all six antibiotics were very vulnerable to P4acta-mase preparations, including the clinically important enzymefrom Escherichia coli (TEM)2 This susceptibility can be corre-lated with a large-inoculum effect, which is most striking withmecillinam. Enzyme susceptibility and inoculum effect wereminimal with cephradine, cefuroxime, and cefoxitin, whilecephalexin gave intermediate values.
Despite our disappointment with the antibacterial activityof mecillinam, and its vulnerability to &bgr;-lactamases, the anti-biotic’s unusual mode of action, discussed in your editorial ofFeb. 4 (p. 252), is of great interest. Unlike other p-lactamagents, it converts gram-negative rods to large osmoticallystable round or oval cells, over a wide range of concentrations.This effect is probably due-at least in E.coli-to the affinityof the antibiotic for the type 2 "penicillin-binding protein"only, which seems to have the extraordinarily specific functionof producing transpeptidation (a final stage in cell-wall synthe-sis) at the "corners" of the bacterial cell. This uniquely re-stricted effect of mecillinam is complementary to the action ofother p-lactam antibiotics that inhibit cell-wall synthesis at dif-ferent sites. On this basis, the combination of mecillinam withother p-lactam agents would be expected to be synergistic, andindeed this is often the case both in vitro and in vivo, notablywith amoxycillin or cephradine.4 There are, nevertheless, im-portant economic implications if combinations of expensiveantibiotics come into widespread use in the future.
Gifts of mecillinam, cefoxitin, cefuroxime, and cefamandole werereceived from Leo Laboratories, Merck Sharp and Dohme, GlaxoLaboratories, and Eli Lilly and Co., respectively.
Department of Bacteriology,Westminster Medical School,London SW1P 2AR
M. BAKHTIARS. SELWYN
*** A line was dropped from our mecillinam editorial last week(restored in American edition). The second sentence was meantto say: "Other penicillins are synthesised from aminopenicil-lanic acid; mecillinam is derived from amidinopenicillanicacid, and its antibacterial spectrum is different."—ED. L
BACTERIAL OVERGROWTH SYNDROME AFTERACUTE NONSPECIFIC DIARRHŒA
SIR,-In support of the findings of Roberts et a1.5 we haverecently seen two patients (male aged 49, female aged 67) withbacterial overgrowth syndrome following acute nonspecificdiarrhoea. Each had travelled to Mexico where they had anacute episode of watery diarrhoea (8-10 bowel movements/day)which lasted for five days and then became chronic (3-5 un-formed stools/day and weight loss). The patients were seen byus 1 month and 3 months respectively after the initial episode.There was no anatomical abnormality. Infectious diarrhoeawas ruled out because stool culture for Shigella, Salmonella,enterotoxigenic Eschericia coli (heat-labile or heat-stable-
toxin-producing) and Vibrio parahcemolyticus was negative.No ova or parasites were seen in the stool preparation. Therewas no significant antibody titre to heat-labile toxin of entero-toxigenic E. coli. colonisation factor of E. coli H-10407 was
negative. Duodenal biopsy was normal and Giardia lambliawas absent both by direct observation and by routine his-tology. In duodenal aspirates, a pure culture of Pseudomonas(108 colonies/ml) was recovered from patient 1 and Entero-
bacter (106 colonies/ml) and a-Streptococcus (102 colonies/ml)from patient 2.
1. Bakhtiar, M., Selwyn, S. Proc. 10th int. Chemother. Congr. (in the press).2. Selwyn, S. J. antimicrob. Chemother. 1977, 3, 161.3. Spratt, B. G. ibid. 1977, 3, suppl. B, p. 13.4. Kerry, D. W., Hamilton-Miller, J. M. T., Brumfitt, W. ibid. 1977, 3, Suppl.
B, p. 53.5. Roberts, S. H., James, O., Jarvis, E. H. Lancet, 1977, ii, 1193.