2 schimbare tulb alimentatie

of 6
-
Upload
yvonne-ioana -
Category
Documents
-
view
216 -
download
0
Transcript of 2 schimbare tulb alimentatie
-
7/30/2019 2 schimbare tulb alimentatie
1/6
Stages and Processes of Change inEating Disorders: Implications
for TherapyWendy Blake1, Sue Turnbull2 and Janet Treasure21Anna Freud Centre, Maresfield Gardens, London NW3, UK2Eating Disorders Research Unit, Institute of Psychiatry, DeCrespigny Park,London SE5 8AF, UK
The aim of this study was to examine the trans-theoretical model ofchange in 51 anorexia nervosa and 58 bulimia nervosa patientsattending a specialist clinic. Self-report questionnaires were completedas to the stage of change, decisional balance, and processes of changebefore initial assessment. Of the BN patients 80% were in a stage of
action compared to only half of the AN patients. There was a shift indecisional balance between the stages of change. The strong principleof change was supported in that the pros of change were increased byover 1 standard deviation from precontemplation to action. The weakprinciple of change was not supported as there was less shift in thecons. Few processes were used in precontemplation, self re-evaluationwas increased in contemplation and self liberation in action. The trans-theoretical model of change appears to be applicable to patients witheating disorders. These preliminary findings suggest ways in whichtherapy can be targeted to maximize the level of motivation and topromote change itself. # 1997 John Wiley & Sons, Ltd.Clin Psychol Psychother 4, 186191, 1997.No. of Figures: 1. No. of Tables: 3. No. of References: 27.
INTRODUCTION
The difficulties in treating women with eatingdisorders have been described at length (Bruch,1973; Brownell and Foreyt, 1986; Alexander andLumsden, 1994). One of the major hurdles is thatpatients with anorexia nervosa do not regardthemselves as having a problem. This was a featurenoted in the historical descriptions. Lasegue (1873),quoted one of his patients who said, `I do not suffer,
therefore I must be well'. This denial or lack ofinsight is part of the ambivalence that these patientshave about change.
In the addictions understanding and tacklingambivalence is an important part of treatment
(Miller and Rollnick, 1991; Bennett, 1993). Sincoff(1990), when describing approachavoidance tend-encies of a behavioural cognitive and affectivenature, summarizes the subject's ambivalence as aninability to make important life decisions. Janis andMann (1977) argue that resolution of decisionalconflict comes about when losses derived frombehaviour exceed gains, thus encouraging the indi-vidual to seek new solutions to chronic problems.Abelson and Levi (1985) suggested that decisional
conflict can be alleviated when the reluctantdecision-maker is able to determine when theinformation is relevant, and subsequently integratesit in such a way that a decision can then be made.
The notion that people change their behaviour byprogressing through various motivational stageshas been influential in the addiction literature(Tuchfield, 1976; Kanfer and Grimm, 1980). Thetrans-theoretical stages of change model seems to
Correspondence to: Dr Janet Treasure, Eating DisordersResearch Unit, Institute of Psychiatry, DeCrespigny Park,London SE5 8AF, UK. Tel: 44 171 919 3180. Fax: 44 171919 3182. E-mail: [email protected].
CCC 10633995/97/03018606$17.50# 1997 John Wiley & Sons, Ltd.
Clinical Psychology and Psychotherapy, Vol. 4 (3), 186191 (1997)
-
7/30/2019 2 schimbare tulb alimentatie
2/6
offer a comprehensive and coherent view of thisprocess. The key assumptions of the model arefirstly, that to change behaviour, people movethrough a sequence of changes and, secondly, differ-ent processes of change are emphasized duringdifferent stages and encourage a progression
through the stages (Sutton, 1996).The stages of change can be described in terms
of a revolving door metaphor (Prochaska andDiClemente, 1992). The person entering the circleof change is in the stage of precontemplation (notthinking about change seriously). This is followedby the next stage in the model, contemplation(starting to think seriously about changing behav-iour). The contemplation stage is followed by action(making an attempt to stop the behaviour). Theaction stage is followed by the maintenance stage(prolonged cessation of behaviour). Relapse maytypically occur several times whilst cycling through
the earlier stages before achieving long-termmaintenance. Individuals can cycle through thestages several times before achieving long-termmaintenance (Prochaska and DiClemente, 1992).Prochaska and DiClemente (1992) have recentlyadded preparation as a stage between contempla-tion and action. However, the questionnairesavailable for the present study did not include thisstage as it was a pre-treatment sample. The stages ofchange are strongly associated with a particularbalance between the pros and cons of a behaviour,the so-called decisional balance (Prochaska, 1994).
The second core dimension of the model is
the process of change. Prochaska and DiClemente
(1983) identified 10 basic processes. These could bedescribed as covert or overt activities that pre-dominate and are integral to the individual's stageof recovery as they move through the stages ofchange. Whereas the stages refer to when particularshifts in attitude and behaviour take place,
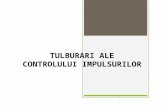
processes attempt to tap into how these shifts occur.The key hypothesis of Stages of Change model isthat different processes, such as consciousness-raising or self-liberation, will predominate at differ-ent stages. Figure 1 shows that during the cycle ofchange the particular processes of change areemphasized (created from Prochaska et al., 1992).This may have implications of clinical relevance inproviding the appropriate focus of treatment forindividuals in particular stages (Prochaska andDiClemente, 1992). A self-treatment book basedupon this model of change has recently beenproduced (Prochaska et al., 1994).
Initially, the Stages of Change model was appliedto the cessation of smoking (Prochaska andDiClemente, 1983; Prochaska et al., 1985, 1988).Subsequently, the model was applied to alcoholand drug abuse, weight control, safe sex andsunscreens (Prochaska et al., 1994). Recently, theStages of Change model has been applied in thefield of eating disorders (Ward et al., 1996). Theresults of this small-scale study with inpatients atthe severe end of the eating disorder spectrumindicate that the trans-theoretical model might alsobe relevant for eating disorders.
The aim of the present study was to examine
whether the Stages of Change model is relevant to
Figure 1. Processes of change. P/C, precontemplation; C, contemplation; A, action; M, maintenance
# 1997 John Wiley & Sons, Ltd. Clinical Psychology and Psychotherapy, Vol. 4(3), 186191 (1997)
Change in Eating Disorders 187
-
7/30/2019 2 schimbare tulb alimentatie
3/6
a broader group, comprising eating disorder out-patients.
METHOD
Subjects
All participants were patients from the south-eastof England referred to a specialist unit at theMaudsley Hospital in London (this is a secondaryor tertiary service). The majority of patients hadprevious treatment from their primary care phys-ician or from their community mental health serviceor from local eating disorder services. The diagnosiswas made by a specialist consultant psychiatristusing structured clinical interviews using criteriafrom the DSM IV: 307.1 AN, 307.51 BN. Concurrentdiagnoses were made using the Clinical Interview
Schedule (CIS) a computerized, validated methodof determining psychopathology (Lewis et al., 1988).
Altogether, 117 questionnaires were collected.Of these three were from patients for whom nodiagnosis was made, two were from obese bingers,and three were not completed sufficiently to beincluded. Of the 109 patients whose questionnaireswere included in the analysis, two were from malesand 107 from females. The age ranges were from16 60 years for participants with a mean of 27 years.Altogether, 51 (47%) participants were diagnosed ashaving anorexia nervosa (AN) (53%) (33 bingepurge subtype; 18 restricting subtype) and 58 as
having bulimia nervosa (BN). The duration of illnesswas shorter in the anorexia patients (mean, 8 years;range 1 20 years); bulimia nervosa (mean 13.8 years;range, 2 27 years). Comorbidity was common:bulimia nervosa (23% depression, 45% anxiety dis-order, 4% OCD); anorexia nervosa purging subtype(50% depression, 4% OCD; 50% anxiety); anorexianervosa restricting subtype (33% depression, 25%OCD, 25% anxiety).
Procedure
Prior to their assessment each of the participants
was asked to complete three questionnaires: aStages of Change algorithm, a Decisional Balancequestionnaire and a Processes of Change question-naire.
Questionnaires
The Stages of Change algorithm is a discretecategorical measure which ascertains the stage of
change from a series of mutually exclusive ques-tions. The eating disorders version used in thisstudy was adapted from Rossi et al. (1995).
The Decisional Balance Inventory for EatingDisorders (DBI-ED) was a 20-item version adaptedfrom Rossi et al. (1995). Statements were scored
using a Likert scale scoring from 15, indicating arange of replies from `not at all important', to`extremely important'. Items represent gains orlosses for self, gains or losses for significant others,self-approval or self-disapproval, and approval ordisapproval of others.
Processes of change were measured using theProcesses of Change questionnaire (PSQ) for weightcontrol (Rossi et al., 1995) adapted for use witheating disorders. This yielded a 48-item instrumentin which eight of the 10 original processes used byProchaska et al. (1988) were deemed relevant.Definitions of the various subscales are as follows
(Prochaska et al., 1992):(1) Consciousness raising: increasing information
about self and problem.(2) Dramatic relief: experiencing and expressing
feelings about one's problems and solutions.(3) Self-re-evaluation: assessing how one feels and
thinks about oneself with respect to a problem.(4) Self-liberation: choosing and commitment to act
or belief in ability to change.(5) Reinforcement management: rewarding one's
self or being rewarded by others for makingchanges.
(6) Counter-conditioning: substituting alternativesfor problem behaviours.
(7) Helping relationships: being open and trustingabout problems with someone who cares.
(8) Stimulus control: avoiding or counteringstimuli that elicit problem behaviours.
The statements were scored using a Likert scalefrom 15 ranging in reply from `not at all' to`extremely'. A `not applicable' option was attachedto some of the anorexic participants' questions,which were then not scored.
Questionnaires are available from authors onrequest.
Statistical Analysis
Data were analysed using SPSS for Windowsversion 6.0 (Norusis, 1993). t-Tests were used totest for group differences in demographic data. Achi-square was used to test for differences indistribution of stages of change and multivariateanalyses of variance (MANOVAs) with Bonferroni
Clinical Psychology and Psychotherapy, Vol. 4(3), 186191 (1997) # 1997 John Wiley & Sons, Ltd.
188 W. Blake, S. Turnbull and J. Treasure
-
7/30/2019 2 schimbare tulb alimentatie
4/6
corrections were used to look at differences betweengroups on processes of change.
RESULTS
Stages of ChangeTable 1 shows the distribution of each diagnosis tothe stages of change. No patients were in themaintenance stage of change and this stage is notconsidered in the analyses.
The distribution across the stages of change weresignificantly different between the groups chi2 15X4, df 1, p 0X00009. The vast majority of thebulimia nervosa patients were in the action stagewhereas the anorexia nervosa patients were moreevenly distributed across the stages with half in theprecontemplation and contemplation stages.
Decisional Balance Inventory
Table 2 shows the mean scores of the pros andcons according to the stage of change (anorexia andbulimia nervosa are shown together as the patternis similar). There was a shift in the decisionalbalance between the stages, the ratio of pros to consbeing: precontemplation 0.82, contemplation 1.3,and action 1.4. These results, in part, support thestrong principle of change as there is an increase inthe pros of change from precontemplation to actionof over 1 standard deviation. However, there is lessshift in the cons between the stages.
Processes of Change
The mean (SEM) scores for the processes areshown by stages of change for all eating disorderstogether in Table 3. All processes were lower in
those in the precontemplation stage. There weresignificant differences on multivariate analysisof variance between stages on self-liberation andself-re-evaluation. Follow-up t-tests showed thatself-liberation was significantly lower in precontem-plation than in action t 2X03 p ` 0X05. Self-re-evaluation was significantly lower in precontem-plation than in contemplation t 2X34 p ` 0X05and action t 3X07 p ` 0X005.
Table 1. Percentage of those in each stage of change
Anorexia nervosa Bulimia nervosan 51 n 58
Precontemplation 12 (23.5%) 2 (3.4%)Contemplation 14 (27.4%) 8 (13.8%)Action 25 (49.0%) 48 (82.8%)
Chi2 15X6, df 2, p ` 0X0005.
Table 2. The pros and cons of change from the Decisional Balance Inventory related to thestages of change
Stage PC Contemplation Action t-testM and SD n 14 n 23 n 72 contrasts
ProsM 24.2 33.3 36.8 PC ` C, AcSD 7.2 8.9 8.0
ConsM 28.6 25.5 26.3 no significant differencesSD 10.5 9.8 8.6
Table 3. Processes and stages of change
Precontemplation Contemplation Actionn 14 n 23 n 72
Mean (SD) Mean (SD) Mean (SD) F-value p-value
Consciousness raising 2.31 (0.87) 2.77 (1.11) 2.50 (1.14) F 0X75 p 0X48Self-liberation 2.19 (0.77) 2.36 (0.95) 2.74 (0.89) F 3X14 p ` 0X05Dramatic relief 2.21 (0.80) 2.57 (1.08) 2.78 (1.18) F 1X53 p 0X22Counter conditioning 2.25 (0.89) 2.23 (1.15) 2.60 (0.92) F 1X64 p 0X20Stimulus control 1.27 (0.45) 1.67 (1.03) 1.68 (0.90) F 1X27 p 0X28Helping relationships 2.46 (1.37) 3.20 (0.89) 3.15 (1.28) F 2X04 p 0X14Self-re-evaluation 2.75 (1.23) 3.58 (0.90) 3.80 (0.89) F 7X11 p ` 0X001Reinforcement management 1.76 (0.53) 1.95 (0.86) 1.67 (0.69) F 1X37 p 0X26
Multivariate analysis of variance, F 2X22, p ` 0X01.
# 1997 John Wiley & Sons, Ltd. Clinical Psychology and Psychotherapy, Vol. 4(3), 186191 (1997)
Change in Eating Disorders 189
-
7/30/2019 2 schimbare tulb alimentatie
5/6
DISCUSSION
The study sprang from a need to understand moreabout ambivalence in patients with eating disordersand the way in which therapeutic interventionsmight be targeted to maximize the level of motiva-
tion to promote change in eating behaviours. Thepatient group is similar to the samples seen at mostspecialist centres in that they have a long durationof illness, a history of unsuccessful interventionsand a high level of co-morbidity. Several interestingpoints of clinical relevance have emerged.
Anorexic patients and bulimic patients were indifferent stages when they presented for treatment.The bulimic patients were most likely to be in actionwhereas more patients with anorexia nervosa werefound to be in precontemplation and contempla-tion. We found that half of those with anorexianervosa were not ready to change their behaviour
when first presenting to the clinic. It is reasonable tospeculate that this might be due to the moreobvious nature of anorexia which might determinethat people often come to the clinic at thesuggestion of relatives or general medical prac-titioners, but they themselves may not be ready forchange. More than 80% of the bulimics wereinitially motivated. The duration of bulimia nervosais greater than that of anorexia nervosa and thesecretive nature of the problem might determinethat by the time people presented for treatment theywere already trying to change their behaviour,although still wishing to exert control over their
weight. The clinical features of anorexia nervosa areegosyntonic whereas this is not true in bulimianervosa where the loss of control over eating is asource of great distress. On the other hand patientswith bulimia nervosa are reluctant to give up theirmethods of weight control. It might have beeninteresting to repeat the application of the trans-theoretical model with weight control rather thanbulimia nervosa as the focus of change. We wouldpredict that fewer cases of bulimia nervosa wouldbe in action if this were the case.
Transition between the stages was associated witha change in the ratio of pros and cons: those in action
had more `pros' for change than those in precon-templation. Prochaska and DiClemente (1992) haveemphasized that the shifting balance between prosand cons is important for those in the contemplationstage. This appears to be the case in eating disordersas the crossover of the ratio of pros and conshappens between precontemplation and contem-plation. Prochaska (1994) observed that the patternin the balance between the pros and cons of change
is consistent across many behaviours. Betweencontemplation and action the pros are increased by1 standard deviation and the cons decreased by0.5 standard deviation (these have been called thestrong and weak principles respectively). Thisfinding has been replicated in another culture using
a different theoretical framework and a differentoperationalization (Dijkstra et al., 1996). However,results of this study do not support the weak prin-ciples of change. This may be because of a differencein the instruments or it may be because thebehaviours relating to eating disorders lead to slim-ness which is highly valued in our society.
As has been found in other conditions pre-contemplation is associated with fewer changeprocesses. Self-re-evaluation was increased in thosein contemplation and self-liberation in the actionstage. This is similar to the generic model (Prochas-ka and DiClement, 1992).
Prochaska and DiClemente (1992) define thetrans-theoretical approach to therapeutic integrationas the differential application of the processes ofchange, at specific stages of change, according to theidentified problem level. This approach has beenapplied to smokers and it has been found that anindividualized trans-theoretical approach per-formed well (Prochaska and DiClemente, 1992).The problem of poor compliance and high drop-outshas bedevilled investigations into the efficacy oftreatment for eating disorders, a trans-theoreticalapproach may limit this problem. We have appliedthe trans-theoretical model to a treatment approach
for eating disorders (Schmidt and Treasure, 1997).Techniques to build upon the processes of con-sciousness raising, dramatic relief, self-re-evaluationand self-liberation are used in the initial stages oftherapy. A motivational interviewing style is used toresolve the conflict relating to the pros and cons ofthe illness. Our pilot data suggests that this is auseful approach.
There are limitations to the findings from thisstudy. It was cross-sectional and involved smallnumbers in comparison with those in studies fromwhich the model was derived. The questionnairesused had to be adapted for this patient group. Our
aim will be to obtain longitudinal measurementswith a larger patient group.
REFERENCES
Abelson, R. P. and Levi, A. (1985). Decision making anddecision theory. In: G. Lindzey and E. Aronson (Eds),
Handbook of Social Psychology, Vol. 1. New York:Random House.
Clinical Psychology and Psychotherapy, Vol. 4(3), 186191 (1997) # 1997 John Wiley & Sons, Ltd.
190 W. Blake, S. Turnbull and J. Treasure
-
7/30/2019 2 schimbare tulb alimentatie
6/6