






Limbile
Pagini
Legal

8/3/2019 Anxietatea La Diabet
1/6
16 June 2011 | Volume 21 | Number 5 PRIMARY HEALTH CARE
Diabetes
PP have diabetes are often highly anxious
during their consultation. This can be the result of
a recent diagnosis, not knowing what to eat, or fear
of needles, hypoglycaemia or losing their feet, their
eyes or their kidney function. Anxiety is just one
of several common emotional and psychological
burdens faced by people with diabetes. Many of
these problems can strongly affect their ability to
manage their condition, leading to poorer glycaemic
control and long-term complications.
These issues have been of such concern that
two organisations, Diabetes UK and NS Diabetes,
convened a working group in 2008 to examine the
literature and good practice in this area, determine
the prevalence of emotional and psychological
problems relating to diabetes and put forward
recommendations for the competencies and types of
interventions required to address the problem.
The working group was jointly chaired by Diabetes
UK and NS Diabetes, with a literature review led by
researchers at the arwickshire Institute of Diabetes,
ndocrinology and Metabolism (ISDM), a clinical
academic collaboration between the University of
CUNTIN ANIT INPP IT DIATSJackie Sturt sets out how and why she helped to establish support services to
address the emotional and psychological needs of patients with diabetes
Summary
Patients with diabetes often face anxiety, low mood
and emotional burden as a result of their condition.
Healthcare professionals need to be aware of this
and the ways in which they can provide help. This
article looks at the possible problems facing patients
and the solutions professionals can offer.
Keywords
Diabetes, depression, anxiety, primary care,
secondary care
arwicks Medical School and University ospitals
Coventry and arwickshire NS Trust (UC).
The group found compelling evidence that services
need to be developed to enhance care and support,
and to improve the psychological wellbeing and
outcomes for people with diabetes (NS Diabetes and
Diabetes UK 2010). It also suggested ways in which
professionals in primary care could better meet the
emotional and psychological needs of patients with
diabetes and, in doing so, improve clinical outcomes.
Quantifying the problemThe emotional and psychological needs of people
with diabetes run on a continuum from healthy
coping through diabetes-related distress to
depression and other conditions sometimes requiring
specialist psychological and psychiatric support. The
needs of a patient on the continuum are influenced
by various factors and may change over time.
Needs will always be shaped by the demands of
the condition and of life, and the interaction between
these demands. They arise in contexts such as
interpersonal relationships, family life, employment
and education. They may be shaped by the cultural
context of the individuals life, the meanings ascribed
to the condition and by religious or spiritual beliefs.
In addition, emotional and psychological issues
are reported by people with diabetes and those
who live with or care for people with the condition.
These issues affecting people with diabetes include
depression, eating disorders, anxiety, needle phobia
and severe mental health conditions. Depression is at
least twice as common in people with diabetes as in
those without it, and studies suggest between 30 and
50 per cent of this depression goes undetected
(Ali et al2006).
8/3/2019 Anxietatea La Diabet
2/6
PRIMARY HEALTH CARE June 2011 | Volume 21 | Number 5 17
Acknowledging that emotional and psychological
issues have a place in consultation can be a first
step towards addressing those problemsCorbis
8/3/2019 Anxietatea La Diabet
3/6
June 2011 | Volume 21 | Number 5 PRIMARY HEALTH CARE18
Diabetes
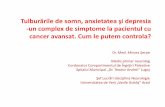
Figure 1 Pyramid describing the prevalence of emotional and psychological
problems in relation to their severity
Level 5
Severe
and complex
mental illness,
requiring specialist
psychiatric intervention(s)
Level 4
More severe psychological
problems that are diagnosable and
require biological treatments, medication
and/or specialist psychological or
psychiatric interventions
Level 3
Psychological problems that are diagnosable/
classifiable but can be treated solely through psychological
interventions, eg mild and some moderate cases of
depression, anxiety st,ates and obsessive/compulsive disorders
Level 2
More severe difficulties with coping, causing anxiety or lowered mood,
with impaired ability to care for self as a result
Level 1
General difficulties coping with diabetes and perceived consequences of this for lifestyle.
Problems at a level common to many or most people receiving the diagnosis
(Adapted from Trigwell et al 2008)
In one ongoing ISDM study, we took a
sample of people from three Coventry P practices
and screened them for depression. They all had
type 2 diabetes, had been diagnosed for at least
six months, were not receiving treatment for
depression and had expressed an interest in taking
part in a psychological intervention. Forty per cent
of those tested demonstrated clinically important
levels of emotional distress or depressive symptoms
measured on the Center for pidemiologic Studies
Depression Scale (adloff 1977).
NS Diabetes and Diabetes UK (2010) looked at
models that have attempted to depict the trajectory
of emotional and psychological needs and found
Figure 1 to be useful in describing the prevalence of
certain problems some formally diagnosable, some
not in relation to their severity. It illustrates the
diversity of need and the broadly inverse relationship
between prevalence and severity of need. At the base
of the pyramid (level 1), needs are common but not
severe, such as general difficulties with coping; at
the top (level 5), needs such as possibly requiring
specialist psychiatric or psychological intervention
are relatively infrequent but severe. evel 1 problems
will be encountered by 60 per cent of people with
diabetes at some point in their lives.
motional or psychological needs at every level are
likely to make the core of diabetes care everyday
self-management harder to achieve. The provision
of emotional and psychological treatment and
support has been found to reduce psychological
distress and improve bA1c, a measure of glycaemic
control, over six to ten weeks in a variety of contexts
(Alam et al2009, inkley et al2006). owever, the
working group found there were major gaps in the
provision of emotional and psychological care for
people with diabetes (NS Diabetes and Diabetes UK
2010). Trigwell et al(2008) showed that 85 per cent
of people with diabetes in the UK have either no
defined access to psychological support and care, or
access only to a local generic mental health serviceat best. Part of the brief of the working group was to
put forward recommendations for commissioners to
ensure services meet the entire spectrum of needs.
Meeting the needFor some commissioners, NS Diabetes and Diabetes
UK (2010) may suggest the need for a complete
overhaul of the way diabetes care is managed.
owever, there are a number of simple, immediate
ways in which healthcare professionals can better
meet the emotional and psychological needs of
people with diabetes, particularly in primary care.
Most patients with a diagnosis of diabetes
receiving treatment in primary care will havetype 2 diabetes, and many of the emotional and
psychological problems they present will be at
levels 1 and 2 of the pyramid model.
esearch has shown that peer support can be
extremely helpful. Programmes such as DSMND,
DAFN and -PT (Patient UK 2010) ensure this
type of support is readily available. Moreover,
social and peer support beyond these formal
programmes can be effective in helping people to
manage diabetes-related distress. Perhaps because
they underestimate the extent to which peer and
social support can be of help, many healthcare
professionals do not ordinarily point patients
towards these kinds of resources.
Not all the solutions are strictly psychological
or therapeutic in nature: for example, joining
organisations such as eight atchers and rambling
groups can help people manage their condition. The
voluntary sector can also be a valuable ally, with
organisations such as Diabetes UK offering support
in the form of volunteer support groups and patient
information. ne of the most effective interventions
8/3/2019 Anxietatea La Diabet
4/6
8/3/2019 Anxietatea La Diabet
5/6
June 2011 | Volume 21 | Number 5 PRIMARY HEALTH CARE2020
Diabetes
achieved by changing the focus of the consultation,
rather than its length, so that appointments are
not centred purely on the clinical requirements of
monitoring diabetes. Acknowledging that emotional
and psychological issues have a place at these
consultations can help to address the problems.
Training in areas such as communication and
patient empowerment is common practice in
primary care, and these skills can improve service
provision for diabetes. Additional techniques, such
as goal-related discussions, counselling skills and
solution-focused therapy, can easily be practised by
non-specialist practitioners (Alam et al2009) and
teams can also be given better guidance on how to
identify more severe emotional and psychological
issues that require specialist intervention.
In these cases, it tends to work better if skills and
competencies development focuses on whole teams
in organisations, rather than selected individualsattending external training sessions. This helps to
embed an understanding that diabetes care involves
elements of clinical and psychological care.
Future of diabetes careThere is a relatively clear distinction between the
care offered by primary and secondary organisations
in managing diabetes. The latter handle almost all
the care requirements for type 1 diabetes, while the
former tend to encounter mostly type 2 diabetes
patients. owever, a shift in service commissioning is
seeing more type 1 patients treated by primary care
services. An increase in the number of type 2 patients
receiving insulin therapy to manage their conditionmeans primary care teams increasingly have the
competencies and confidence to handle more
complex diabetes issues.
These changes make it even more important that
primary care organisations are well equipped to
identify and cope with the range of emotional and
psychological problems associated with diabetes.
People with diabetes should not have to rely for
their psychological help and treatment on the best
efforts of people who are not adequately trained orsupported to carry out that work.
ISDM continues to focus on assessing patients
for diabetes-related distress using the Problem Areas
in Diabetes Scale (Polonsky et al1995). It offers them
the support they need through one-to-one sessions
with diabetes listeners (ox 1) and/or directing
them to other services. ISDM has more work to
undertake, but these first steps are imperative to
making a difference to patients.
Alam R, Sturt J, Winkley K (2009) An updatedmeta-analysis to assess the effectiveness
of psychological interventions delivered by
psychological specialists and generalist clinicans
on glycaemic control and on psychological
status. Patient Education and Counseling. 75,
1, 25-36.
Ali S, Stone MA, Peters JL et al(2006) The
prevalence of co-morbid depression in adults
with type 2 diabetes: a systematic review
and meta-analysis. Diabetic Medicine. 23, 11,
1165-1173.
Improving Access to Pyschological TherapiesTeam (2010) NS: IAPT. www.iapt.nhs.uk (ast
accessed: February 7 2011.)
NHS Diabetes, Diabetes UK (2010) motional
and Psychological Support and Care in Diabetes:
eport from the motional and Psychological
Support orking roup of NS Diabetes and
Diabetes UK. www.diabetes.org.uk/Documents/
eports/motional_and_Psychological_Support_
and_Care_in_Diabetes_2010.pdf (ast accessed:
February 7 2011.)
Patient UK (2010) Diabetes Education and
Self-management Programmes.
www.patient.co.uk/doctor/DSMND.htm(ast accessed: February 7 2011.)
Polonsky WH, Anderson BJ, Lohrer PA et al
(1995) Assessment of diabetes-specific distress.
Diabetes Care. 18, 6, 754-760.
Radloff LS (1977) The CS-D scale: a self-report
depression scale for research in the general
population. Applied Psychological Measurement.
1, 3, 385-401.
Steed L, Cooke D, Newman S (2003) A
systematic review of psycholigical outcomes
following education, self-management and
pyschological intervention in diabetes mellitus.Patient Education and Counseling. 51, 1, 5-15.
Trigwell P, Taylor J-P, Ismail K et al(2008)
Minding the Gap. The Provision of Psychological
Support and Care for People with Diabetes in the
UK. www.diabetes.org.uk/Documents/eports/
Minding_the_ap_psychological_report.pdf (ast
accessed: February 7 2011.)
Winkley K, Eisler I, Ismail K (2006) Psychological
interventions to improve glycaemic control in
patients with type 1 diabetes: systematic review
and meta-analysis of randomised controlled trials.
British Medical Journal. 333, 7558, 65.
References
Jackie Sturt is associate professor
in social and behavioural science
and the primary care research
group lead at the Health Sciences
Research Institute, Warwick
Medical School, and a diabetes
listener at the WISDEM Centre,
University Hospital, Coventry
Box 1 Theory in practice
The author has helped reshape and pioneer support services for people with
diabetes in her area of Coventry and Warwickshire, recently setting up a diabetes
listening service for people with diabetes who are struggling with emotional and
psychological problems. This service consists of 45-minute appointments in theDiabetes WISDEM Centre. These are available to anyone with the condition,
regardless of type or severity. The initial sessions focus on listening and using
person-centred counselling skills. Over time, they become more action-orientated to
help people find coping mechanisms for managing their life with diabetes. People
can book up to six appointments.
Suzy (named changed) was referred by her diabetologist with high anxiety regarding
fear of nocturnal hypoglycaemia. She spent several nights a week alone with her
young daughter, which fuelled her fear of the conditions possible consequences.
During two 45-minute consultations. Suzy was able to articulate attitudes to eating,
insulin and weight that were unexplored. She recognised her evening snacking was
linked to loneliness and boredom, rather than to ensure high blood glucose levels
at bedtime. She implemented a home exercise regime. She found other ways to
occupy her evenings, which helped reduce boredom and snacking, and maintainher weight. She arranged to text a friend each morning to say everything was alright
if she did not, her friend would raise the alarm. Over the sessions her fears began
to diminish.
Bob (name changed) who had bilateral amputations eight months before his
referral, was struggling to come to terms with his disability and this was affecting
his diabetes control. Through a series of sessions, healthcare professionals explored
the broad aspects of his life that his disability was affecting. He began to come
up with solutions and develop confidence in his abilities, despite his new health
status. Instead of being overwhelmed by all his issues, he began to approach them
sequentially, in line with the natural rise and fall of his prioritisation. His aim is to be
sufficiently calm about these issues so that he can think about his diabetes again.
This article has beensubject to double-blind
review and checked using
antiplagiarism software
8/3/2019 Anxietatea La Diabet
6/6
Copyright of Primary Health Care is the property of RCN Publishing Company and its content may not be
copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written
permission. However, users may print, download, or email articles for individual use.
Top Related