TIBOLA - · PDF fileapãrutã în urmã cu 45 de zile, ... Pacienta nu...

If you can't read please download the document
Transcript of TIBOLA - · PDF fileapãrutã în urmã cu 45 de zile, ... Pacienta nu...
TIBOLA
TIBOLA
ALEXANDRU OAN*, MARIUS IRIMIE*, GABRIELA STOLERIU**, SMARANDA OAN***,VERONICA ILIESCU***
249
* Universitatea Transilvania Braov, Facultatea de Medicin, Braov / Transilvania University of Brasov, Faculty of Medicine, Brasov.** UMF Iai, Catedra de Dermatologie / UMF Iasi, Dermatology Department.*** SC Dermamed SRL Braov / SC Dermamed SRL Brasov.
Summary
TIBOLA (tick-borne lymphadenopathy) is arickettsiosis transmitted to humans through a tick of theDermacentor genus, most commonly incriminatedpathogen being Rickettsia slovaca.
A 55-year-old female patient was consulted for aninflammatory red purple plaque, infiltrated, round with adiameter of 2 cm, located in the upper part of the scalp andemerged after 45 days, about 10 days after a tick biteoccurred in February 2015, during a walk in a forest. Thesting was initially accompanied by an itchy edematouserythema of the cephalic region. The inflammatory plaquewas accompanied by painful right laterocervicallymphadenopathy. The patient did not have fever orimpaired general condition. Common blood and biochemicallaboratory investigations were normal. Antibody testingfor Borrelia burgdorferi was negative. She was treated withdoxycycline 200 mg/day for 3 weeks with the disappearanceof the inflammatory lesion and the laterocervicallymphadenopathy and the persistence of a residual alopecicarea. TIBOLA diagnosis was established based on clinical,anamnestic criteria and improvement under treatment withdoxycycline.
The epidemiological characteristics of TIBOLA are:seasonal distribution in the cold months of the year(September to May) and geographical location in theMediterranean and Eastern Europe. The averageincubation is 7 days. Clinical diagnosis of TIBOLA is basedon the following binding specific criteria: the bite of a largetick on the upper body (90% on the hairy skin of the head),necrotic eschar at the site of the tick bite surrounded byfixed erythematous halo and painful regionallymphadenopathy (occipital , cervical) and nonspecific
Rezumat
TIBOLA (tick-borne lymphadenopathy) este orickettsioz transmis la om printr-o cpu din genulDermacentor, agentul patogen cel mai frecvent incriminatfiind Rickettsia slovaca.
Pacient n vrst de 55 ani a fost consultat pentru oplac inflamatorie roie violacee, infiltrat, rotund avnddiametrul de 2 cm, localizat la nivelul vertexului iaprut n urm cu 45 de zile, la aproximativ 10 zile dupo neptur de cpu survenit n luna februarie 2015, ntimpul unei plimbri ntr-o pdure. neptura a fostnsoit iniial de un eritem edematos pruriginos al regiuniicefalice. Placa inflamatorie era nsoit de adenopatielaterocervical dreapt dureroas. Pacienta nu prezentafebr i nici alterarea strii generale. Investigaiile delaborator hematologice i biochimice uzuale au fostnormale. Serologia pentru Borrelia burgdorferi a fostnegativ. Tratamentul a fost efectuat cu doxiciclin 200mg/zi timp de 3 sptmni cu dispariia leziuniiinflamatorii i a adenopatiei laterocervicale i persistenadoar a unei zone alopecice reziduale. Diagnosticul deTIBOLA a fost stabilit pe baza criteriilor clinice,anamnestice i evoluiei bune sub tratamentul cuDoxiciclin.
Caracteristicile epidemiologice de TIBOLA sunt:distribuirea sezonier n lunile reci ale anului (septembrie-mai) i localizarea geografic n ri mediteraneene i aleEuropei de Est. Incubaia medie este de 7 zile. Clinic,diagnosticul de TIBOLA se bazeaz pe urmtoarele criteriiobligatorii specifice: neptura unei cpue de maridimensiuni pe partea superioar a corpului (90% pe pieleaproas a capului), escar necrotic de inocularenconjurat de un halou eritematos fix i adenopatie
CAZURI CLINICECLINICAL CASES
250
DermatoVenerol. (Buc.), 60: 249-254
Introducere
TIBOLA (tick-borne lymphadenopathy) esteo rickettsioz transmis la om printr-o cpu dingenul Dermacentor, agentul cauzal cel maifrecvent incriminat fiind Rickettsia slovaca.Tabloul clinic asociaz prezena nepturii decpu, escarei inflamatorii la locul de inocularei adenopatiei locoregionale. Au fost propuse ialte denumiri pentru acest sindrom precumDEBONEL (DErmacentor - BOrne Necrosis -Erythema Lymphadenopathy)1 i SENLAT (ScalpEschar and Neck LymphAdenopathy after Tick-bite)2.
Caz clinic
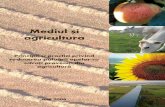
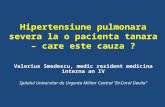
Pacient n vrst de 55 ani a fost consultatpentru o plac inflamatorie, pruriginoas,localizat la nivelul vertexului afirmativ aprutn urm cu aproximativ 45 de zile. Leziunea adebutat la aproximativ 10 zile dup o nepturde cpu n timpul unei plimbri ntr-o pduredin zona montan n luna februarie a anului 2015.Pacienta nu a prezentat febr i nici alterareastrii generale, iar tratamentul cu betalactaminenu a fost eficient. La examenul dermatologic aprezentat o plac inflamatorie roie-violacee,infiltrat, rotund cu diametrul de 2 cm,localizat la nivelul vertexului nsoit deadenopatie laterocervical dreapt dureroas,ganglionii avnd diametrul de pn la 2 cm(Fig.1, Fig.2). Investigaiile de laborator
Introduction
TIBOLA (tick borne lymphadenopathy) is arickettsiosis transmitted to humans through atick of the Dermacentor genus, the most commoncausative agent being Rickettsia Slovaca. Theclinical presentation associate the presence of atick bite, an inflammatory eschar at theinoculation site and regional lymphadenopathy.Other names have been proposed for thissyndrome such as DEBONEL (DErmacentor -BOrne Necrosis - Erythema Lymphadenopathy)1
i SENLAT (Scalp Eschar and NeckLymphAdenopathy after Tick-bite)2.
Clinical case
A 55-year-old female patient was consultedfor an itchy inflammatory plaque, located in theupper part of the scalp and emerged 45 days ago.The lesion appeared about 10 days after a tickbite occurred in February 2015, during a walk ina mountain forest. The patient did not have feveror impaired general condition and the treatmentwith beta-lactam antibiotics was inefficient. Thedermatological exam describes a red purple,inflamatory plaque, infiltrated and round with adiameter of 2 cm, located in the upper part of thescalp, accompanied by painful right laterocervicallymphadenopathy, with lymph nodes up to 2 cmin diameter (Fig.1, Fig.2). Common blood andbiochemical laboratory investigations werenormal. Antibody testing for Borrelia burgdorferi
regional dureroas (occipital, cervical) i pe criteriiminore nespecifice: cefalee, febr, artromialgii, astenie,erupie cutanat. Diagnosticul de certitudine se bazeaz peexaminrile microbiologice dintre care cea mai utilizat esteimunofluorescena indirect. Evoluia afeciunii este rapidfavorabil sub tratament cu dispariia febrei n cteva zile ia adenopatiei ntr-o sptmn cu persistena unei alopeciicicatriciale pe locul escarei. Tratamentul de elecie estedoxiciclina la aduli i macrolidele de ultim generaie(azitromicina i claritromicina) la copii i femeile gravide.
TIBOLA este o rickettsioz cu o emergen n creteren Romnia, n parte cauzat rspndirii cpuelor dingenul Dermacentor.
Cuvinte cheie: TIBOLA, DEBONEL, Rickettsiaslovaca, neptur de cpu, Dermacentor.
Intrat n redacie: 6.10.2015Acceptat: 27.11.2015
Received: 6.10.2015Accepted: 27.11.2015
minor criteria: headache, fever, arthromyalgia, asthenia,rash. A certainty diagnosis is based on microbiologicalexaminations of which indirect immunofluorescence is themost widely used. The evolution of the disease is rapidlyimproving under treatment with the disappearance of thefever in a few days and the lymphadenopathy in a week witha persistent cicatricial alopecia on the eschar. The treatmentof choice is doxycycline for adults and new-generationmacrolides (azithromycin and clarithromycin) in childrenand pregnant women.
TIBOLA is a rickettsiosis with a growing emergence inRomania, in part because of the spread of ticks of the genusDermacentor.
Key words: TIBOLA, DEBONEL, Rickettsia slovaca,tick bite, Dermacentor.
hematologice i biochimice uzuale au fostnormale. Serologia pentru Borrelia burgdorferi afost negativ. Pacienta a urmat tratament cudoxiciclin 200 mg/zi timp de 3 sptmni cudispariia att a leziunii inflamatorii ct i aadenopatiei laterocervicale dup dou sptmnide tratament, la finalul tratamentului persistndo zon alopecic rezidual pe locul plciieritematoase iniiale. Diagnosticul de TIBOLA afost stabilit pe baza criteriilor anamnestice, clinicei a evoluiei favorabile sub tratamentul cuDoxiciclin.
Discuii
Agentul patogen cel mai frecvent incriminatn TIBOLA este R. slovaca, izolat n 1968 nRepublica Ceh i avnd ca vector o cpu maredin genul Dermacentor. Raoult i colab. (1997)descriu cazul unui pacient care prezenta oleziune unic de inoculare pe pielea proas acapului nsoit de adenopatie cervical3. Untablou clinic similar este gsit n acelai an deLakos la 27 pacieni descriindu-l sub numele deTIBOLA (TIck BOrne LymphAdenopathy), unsindrom constnd din asocierea unei escareinflamatorii de inoculare, adenit locoregional ineptur de insect4. Alturi de R. slovaca, napariia TIBOLA sunt incriminate i alterickettioze sau bacterii intracelulare precum R.raoultii5, Bartonella henselae6, Francisellatularensis7.
was negative. The patient was treated withdoxycycline 200 mg/day for 3 weeks with thedisappearance of the inflammatory lesion and thelaterocervical lymphadenopathy after 2 weeks oftreatment and the persistence of a residualalopecic area at the end of the treatment. TIBOLAdiagnosis was established based on clinical,anamnestic criteria and improvement undertreatment with doxycycline.
Discutions
The most frequent incriminated pathogen inTIBOLA is R. slovaca, isolated in 1968 in theCzech Republic transmitted by large Dermacentorticks. Raoult et al. (1997) describe a patient whoshows a single inoculation lesion on hairy skin ofthe head accompanied by cervical lym-phadenopathy3. A similar clinical picture isfound in the same year by Lakos in 27 patientsdescribing it as TIBOLA (TIck BOrneLymphAdenopathy), a syndrom