Nonorganic hearing loss. Malingering, factitious or ... · PDF file38 Georgescu M.G. et al...
6
Rom J Leg Med [22] 35-40 [2014] DOI: 10.4323/rjlm.2014.35 © 2014 Romanian Society of Legal Medicine 35 Nonorganic hearing loss. Malingering, factitious or conversion disorder? Mădălina Gabriela Georgescu 1,2,* , Carmen Ioana Stan 3 , Andreea Natalia Marinescu 4 , Diana Loreta Păun 1,5 _________________________________________________________________________________________ Abstract: is paper aims to draw attention on the diagnostic of nonorganic hearing loss. It is a common diagnostic present mostly in children with apparent sudden sensorineural hearing loss and in adults who intentionally or not claim to have a hearing problem. Material and methods. Two case-reports of nonorganic hearing loss - an adult male patient who complains of leſt ear hearing loss aſter a physical aggression – head trauma in the leſt temporal region and an eight years-old boy with school problems who thought he had a hearing problem. Both patients were sent for audiological evaluation in the ENT Institute. Discrepancy between pure tone audiometry and speech test determined the audiologist to extend the audiological evaluation with objective methods – acoustic immitance, otoacoustic emissions and auditory brainstem response. Results. Objective audiological examination revealed normal hearing in the both ears in both patients. Conclusions. Uncommon informal behavior as well as discrepancies between different tests should suggest a nonorganic hearing loss which must be completely evaluated. Electrophysiologic methods are most used nowadays in these patients. Key Words: nonorganic hearing loss, malingering hearing loss, factitious hearing loss, objective audiology. 1) “Carol Davila” University of Medicine, Bucharest, Romania * Corresponding author: MD, PhD, Lecturer, Institute of Phono-Audiology and Functional ENT Surgery, Tel.: +40722544115, 21 st Mihail Cioranu street, District 5, zip code: 050751, Bucharest, Romania, Email: [email protected] 2) Institute of Phono-Audiology and Functional ENT Surgery, Audiology and Vestibulogy Dept., Bucharest, Romania 3) Ilfov County Hospital, ENT Department, Ilfov, Romania 4) Institute of Phono-Audiology and Functional ENT Surgery, Otologic Surgery Dept., Bucharest, Romania 5) “C. I. Parhon” National Institute of Endocrinology, Bucharest, Romania N onorganic hearing loss (NOHL) is a term used to describe a hearing loss that appears greater than can be explained by auditory system lesion and pathophysiology [1] and in which subjective hearing level is different from objective one. “Nonorganic hearing loss”, “pseudohypoacusis” or “functional hearing loss” is equivalent terms [2]. NOHL represents the most frequent etiology of sudden hearing loss in children [3], even though this diagnostic is oſten forgot. In literature [4] there is a recommended nomenclature with different categories of NOHL based on the degree of intent (intentional or unintentional) and type of gain (internal or external) (Table 1). NOHL in children is most frequently bilateral and is caused by a psychological / psychiatric problem - factitious or conversion disorder. In factitious, children play a sick role, in order to avoid facing school or collectivities problems. More serious are problems in conversion disorder, when children truly think they have a hearing problem as an expression of their poor
Transcript of Nonorganic hearing loss. Malingering, factitious or ... · PDF file38 Georgescu M.G. et al...

Rom J Leg Med [22] 35-40 [2014]DOI: 10.4323/rjlm.2014.35© 2014 Romanian Society of Legal Medicine
35
Nonorganic hearing loss.Malingering, factitious or conversion disorder?
Mădălina Gabriela Georgescu1,2,*, Carmen Ioana Stan3, Andreea Natalia Marinescu4, Diana Loreta Păun1,5
_________________________________________________________________________________________ Abstract: This paper aims to draw attention on the diagnostic of nonorganic hearing loss. It is a common diagnostic present mostly in children with apparent sudden sensorineural hearing loss and in adults who intentionally or not claim to have a hearing problem. Material and methods. Two case-reports of nonorganic hearing loss - an adult male patient who complains of left ear hearing loss after a physical aggression – head trauma in the left temporal region and an eight years-old boy with school problems who thought he had a hearing problem. Both patients were sent for audiological evaluation in the ENT Institute. Discrepancy between pure tone audiometry and speech test determined the audiologist to extend the audiological evaluation with objective methods – acoustic immitance, otoacoustic emissions and auditory brainstem response. Results. Objective audiological examination revealed normal hearing in the both ears in both patients. Conclusions. Uncommon informal behavior as well as discrepancies between different tests should suggest a nonorganic hearing loss which must be completely evaluated. Electrophysiologic methods are most used nowadays in these patients. Key Words: nonorganic hearing loss, malingering hearing loss, factitious hearing loss, objective audiology.
1) “Carol Davila” University of Medicine, Bucharest, Romania* Corresponding author: MD, PhD, Lecturer, Institute of Phono-Audiology and Functional ENT Surgery, Tel.: +40722544115, 21st Mihail Cioranu street, District 5, zip code: 050751, Bucharest, Romania, Email: [email protected]) Institute of Phono-Audiology and Functional ENT Surgery, Audiology and Vestibulogy Dept., Bucharest, Romania3) Ilfov County Hospital, ENT Department, Ilfov, Romania4) Institute of Phono-Audiology and Functional ENT Surgery, Otologic Surgery Dept., Bucharest, Romania5) “C. I. Parhon” National Institute of Endocrinology, Bucharest, Romania
Nonorganic hearing loss (NOHL) is a term used to describe a hearing loss that appears
greater than can be explained by auditory system lesion and pathophysiology [1] and in which subjective hearing level is different from objective one. “Nonorganic hearing loss”, “pseudohypoacusis” or “functional hearing loss” is equivalent terms [2]. NOHL represents the most frequent etiology of sudden hearing loss in children [3], even though this diagnostic is often forgot. In literature [4] there is a recommended
nomenclature with different categories of NOHL based on the degree of intent (intentional or unintentional) and type of gain (internal or external) (Table 1). NOHL in children is most frequently bilateral and is caused by a psychological / psychiatric problem - factitious or conversion disorder. In factitious, children play a sick role, in order to avoid facing school or collectivities problems. More serious are problems in conversion disorder, when children truly think they have a hearing problem as an expression of their poor

36
Georgescu M.G. et al Nonorganic hearing loss. Malingering, factitious or conversion disorder?
relationships in family. Compared to children, in adults NOHL is mostly unilateral and is intentional (malingering hearing loss). Financial gain is the most common reason which determines people to feign a hearing loss after head injury. Malingering hearing loss is a form of NOHL and this term implies that the subject is consciously pretending to have a worse level of hearing than the real one in order to avoid some responsibility/seeking material compensation.
The source of referral is the first element which should make the audiologist to take into account the diagnostic oh NOHL. Patients sent for audiometry from legal medicine departments due to casualty or violent incidents should be carefully evaluated. History is always valuable, starting even from lowering examiner’s voice level during conversation or whispering at the affected ear during ear examination (otoscopy). Not only the response matters, but also the manner in which these are offered as well as the quality of voice of the subject who claims bilateral deafness. If hearing impaired patients are often taciturn about their hearing problem, the NOHL subject volunteer for unasked or supplementary information. The presence of the muscular reflexes provoked by loud sounds (cochleoauricular/ pupillary/ palpebral reflexes) excludes severe hearing loss. If malingering is suspected, pure tone audiometry (PTA) must by combined with speech audiometry since gross discrepancy between the two above mentioned tests indicates NOHL [5] [3]. The degree of hearing loss in PTA is established based on arithmetic average of 500, 1000 and 2000Hz thresholds. As for speech audiometry, speech recognition threshold (SRT) represents the intensity in dB where the subject repeats correctly 50% of the presented words. Also, more than 10dB difference between PTA thresholds in ascending versus descending methods is an indicator for NOHL [6]. Very useful in detecting NOHL is objective audiology, especially acoustic immitance (tympanometry and acoustic stapedius reflex), otoacoustic emissions (OAE) and auditory evoked potentials (AEP). Normal tympanometry (type A = peak compliance between
+50 and -100daPa) is mandatory in order to search for stapedius reflex and in order to have reliable OEA measurements. Two types of OAE are used: Transient OAE (TEOAE) which is present if external hair cells from the cochlea are functionally, equivalent with hearing level better than 30dB. Distortion products OAE (DP-OAE) allows a larger range of frequencies to be evaluated. Presence of DP-OAE stands for a hearing better than 40dB. Late AEP, especially cortical ones (CAEP) are the
best method to demonstrate the functionality of the entire auditory pathway [7]. More than this CAEP provides threshold information at octave frequencies in the range of 500-4000Hz, but it is very difficult sometimes to keep the subject vigilant and the procedure lasts almost one hour. For this reason auditory brainstem response (ABR) which does not depend on vigilance and lasts much less became the AEP method of choice. ABR have proven to be more reliable than the later responses in identifying NOHL [8, 9]. However, ABR has a limitation due to less frequency specificity since stimulus used is usually the click. The cross-checked principle introduced in audiology by James Jerger for accurate evaluation of hearing level in children is also very useful in detecting NOHL. We consider that the battery test proposed by Berlin [10] for objective audiologic evaluation of hearing in children - acoustic immitance (tympanometry and acoustic reflexes), otoacoustic emissions and auditory brainstem response - is appropriate also for NOHL subjects.
Patients Two patients are presented: 1. 52 years old male patient, GF, who was sent from the “Mina Minovici” National Institute of Legal Medicine to the „Professor Dr. Dorin Hociota” Institute of Phono-Audiology and ENT Functional Surgery for hearing level evaluation. The subject claims that after a physical aggression (hit over the left ear with hand) he lost hearing in his left ear. 2. Eight years old boy, MJ of non-Romanian
Category Austen-Linch, 2004 Aplin&Rowson, 1990
1 Malingering: intentional, motivation, external gain
Minor problems: no serious home or school-based problems
2 Factitious disorder: motivation is to play a sick role, rather intra-psychic gain
School based problems: difficulties arising from transfer to school, poor school attainment, poor peer relationships
3 Conversion disorder: unintentional intent, internal gain
(Deeper) major disturbance: poor relationships with parents/siblings, emotional, family and marital problems
Table 1. Different categorizations of NOHL

Romanian Journal of Legal Medicine Vol. XXII, No 1(2014)
37
nationality, recently moved in Romania, claims to hear very poor and this is the reason for his poor results at school.
MeThods
Audiometry was performed in a soundproof room. Pure tone and speech audiometry were carried out with a clinical audiometer (Madsen OB 822, GN Otometrics, Taastrup, Denmark) with TD39 headphones. Native Romanian language speech list was used for the speech audiometry (disyllabic words) in the adult case. Tympanometry and stapedial reflex measurements were performed using a Madsen Zodiac 901 Middle Ear Analyzer (GN Otometrics, Taastrup, Denmark). DPOAE and ABR were recorded with a BioLogic EP machine (NATUS, USA), with insert phones (click as stimulus).
ResulTs
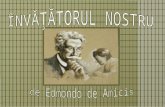
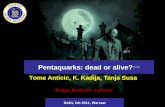
Case 1 Subjective audiometry showed normal hearing in the right ear and severe sensorineural hearing in the left ear, with 45 dB discrepancy between PTA threshold and SRT in the left ear (Fig. 1, 2).
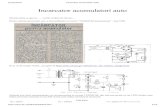
Objective audiological evaluation demonstrated normal hearing in both ears, as well as normal middle ear function (Fig. 3).
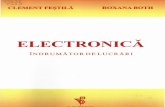
DP-OAE were present in both ears, demonstrating the bilateral normal cochlear function (Fig. 4).
ABR was present in both ears until 25dB HL stimulation, consistent with bilateral normal auditory function (Fig. 5).
Case 2 Subjective audiometry showed bilateral severe sensorineural hearing loss. Speech audiometry could not be performed since the patient does not know Romanian language (Fig. 6). Objective audiological evaluation by means of ABR (Fig. 7) demonstrated normal hearing in both ears.
Figure 1. PTA – normal hearing in the right ear; Severe sensorineural hearing loss in the left ear (85dB).
o - AC right ear< - BC right ear☐ - Masked BC
Mean PTA threshold: 90+90+75 =853
sRT
Figure 2. Speech audiometry – SRT=15dB in the right ear and 40dB in the left ear.
Tympanometry type A in both ears (normal middle ear pressure). Acoustic Stapedius reflex threshold at 80dB/90dB in both ears, in ipsi- and contralateral stimulation.
Figure 3. Acoustic immitance.
Figure 4. DP-OAE (2F1-F2) present in both ears between 2-8kHz.

38
Georgescu M.G. et al Nonorganic hearing loss. Malingering, factitious or conversion disorder?
Figure 5. a) ABR – 25dB HL threshold in both ears; b) - latencies of wave I and V and interpeak I-III and I-V values in normal range.
o - AC right ear; X - AC left ear
Figure 6. PTA – bilateral severe sensorineural hearing loss.
Figure 7. a) ABR – 10dB HL threshold in both ears ; b) latencies of wave I and V and interpeak I-III and I-V values in normal range.

Romanian Journal of Legal Medicine Vol. XXII, No 1(2014)
39
discussioN
As mentioned before, NOHL describes the audiological discrepancies that exist between the real hearing threshold determined objectively and the subjective hearing threshold based on patient‘s response, in the absence of any anatomical or physiological lesion [11]. In case of the adult patient, since no imagistic lesion was determined after the violent incident involving head trauma, malingering hearing loss was considered. The conscious NOHL is based on the psychogenic process of a purposeful, motivated behavior in order to gain financial benefit. NOHL is a common and well-recognized phenomenon in adults, especially if any kind of gain is involved. Intentional feigning of hearing loss after physical aggression seems to be a good option for these patients, since they consider hearing evaluation is based solely on patient’s sensations. In literature a predominance of NOHL in women is cited female:male ratios ranging from 2:1 to 10:1 [12-14]. Most often NOHL is present in both ears, but 28% of NOHL subjects claims unilateral hearing loss [13, 15], of various degrees. In most studies flat or curve sensorineural hearing loss is described [12]. Depending on the cause of NOHL (conscious or unconscious), spontaneous recovery is frequently met in different time-spans, between one and 8 weeks [16] mainly if no financial gain is seek. Completely different happens in malingering NOHL, when litigation proceedings develop. Regarding children, it is already well known about different types of non-organic hearing loss, factitious or conversion disorders, depending on the severity of the psychological problem. NOHL is just a way of expression of these disorders and family, physicians and shrinks have a great importance role in detecting and solving the real problem. We like to highlight the importance of permanent observation of children’s behavior, involvement in their collectivity based activities (kindergarten, school), discussions in family in order to avoid such psychological problems. As mentioned before, in NOHL as factitious disorder, children’s motivation is to play a sick role in order to avoid facing school based problems: difficulties arising from transfer to school, poor school attainment and poor peer relationships. As for NOHL as conversion disorder, children has unintentional intent. (Deeper) major disturbances are present, arising from poor relationships with parents/siblings and children sick an internal gain by feigning hearing loss. However, for an experienced clinician, the diagnosis of NOHL is custom, since it is based on logical protocol and objective measurements. Sometimes it
is more difficult to consider this hypothesis than to demonstrate it. Patient’s behavior during history and subjective audiometry is most relevant for the clinicians. Observation during testing is usually alerting the examiner. Sometimes, due to associate otologic pathology, objective electrophysiologic audiologic measurements (acoustic immitance, otoacoustic emissions-OAE and auditory evoked potentials-AEP) are not enough to diagnose a NOHL. CT scan or MRI centered on the auditory system must be taken into account for differential diagnostic. Especially since in most cases NOHL is referred as sudden sensorineural hearing loss. For unilateral NOHL, Stenger test is a reliable audiological method to rule out NOHL in adult patient - Durmaz et al. reported that the sensitivity, specificity, positive predictive value and negative predictive values of the Stenger test were 70%, 99.4%, 87.5% and 98.4%, respectively [17]. Nowadays, electrophysiologic examinations became rutine: if no middle ear problem is detected in acoustic immitance, OAE is first choice of objective test, since it is noninvasive, easy and very quick. Two types of OAE measurements are available – transient OEA (TEOAE) and distorsion products (DP OAE). TEOAE which has no frequency specificity because the stimulus is the click and the results has no correlation with audiometric thresholds [18], but demonstrates normal function of the external cochlear hair cells. DPOAE has frequency specificity [19] and reveals, if present, a hearing level better than 40dB with good correlation with pure tone audiometry results [20]. Still, hearing develops in the auditory cortex and OAE alone is not enough to demonstrate that the subject hears normally. Early (brainstem) and late (cortical) AEP can demonstrate the transmission of the neural signals in the central auditory pathway. For brainstem AEP (ABR - auditory brainstem response) click is the usually stimulus used for reliable results. It has however, a drawback - information is limited to 2-4 kHz domain. Tone burst was proposed for low-frequency ABR, but electrophysiological threshold results have a larger deviation from audiometric threshold in normal or hearing impaired patients without NOHL.Late AEP (CERA – cortical evoked response audiometry) are the method of choice, since it evaluates the entire auditory pathway, from cochlea to the auditory cortex and can objectively identify the NOHL.
coNclusioNs
Non-organic hearing loss should be consider as differential diagnostic in sudden hearing loss in children and in adults involved in accidents, violence and litigation proceedings. Discrepancy between subjective hearing evaluation and objective audiological measurements in

40
Georgescu M.G. et al Nonorganic hearing loss. Malingering, factitious or conversion disorder?
absence of anatomical lesions is the key for the diagnostic of non-organic hearing loss.
Acknowledgment. The first two authors contributed equally to this article.
References1. Katz J., Medwetsky L., Burkard R., Hood L., Nonorganic hearing loss In: Handbook of Audiology (sixth ed.), Wolters Kluwer, Lippincott
Williams&Wilkins 2009, pp. 699-712.2. Gelfand S.A., Nonorganic hearing loss, S.A. Gelfand (Ed.), Essentials of Audiology (3rd ed.), Thieme, New York (2009), pp. 405–426.3. Rintelmann W.F., Schwan S.A., Blakley B.W., Pseudohypacusis, Otolaryngol. Clin. North Am., 24 (2) (1991), pp. 381–390.4. Austen S., Lynch C., Non-organic hearing loss redefined: understanding, categorizing and managing non-organic behaviour, Int. J. Audiol.,
43 (8) (2004), pp. 449–457.5. Schmidt CM, am Zehnhoff-Dinnesen A, Matulat P, Knief A, Rosslau K, Deuster D, Nonorganic hearing loss in children: audiometry,
clinical characteristics, biographical history and recovery of hearing thresholds, Int J Pediatr otorhinolaryngol. 2013 Jul;77(7):1190-1193.6. Mahdavi, Mohammad-Ebrahim, MSc; Mokari, Nooshin, MSc; Amiri, Zohreh, PhD, Educational Level and Pseudohypacusis in Medico-
Legal Compensation Claims: A Retrospective Study, Archives of Iranian Medicine 14.1 (Jan 2011): 58-60.7. Lightfoot, G., & Kennedy, V., Cortical electric response audiometry hearing threshold estimation: Accuracy, speed and the effects of
stimulus presentation features. Ear Hear, 2006,27(5), 443-456, Knight and Beagley, 1970.8. Hall JW, Handbook of Auditory Evoked Responses. Boston: Allyn and Bacon, 1992; 383-384.9. Schulman-Galambos C., Galambos R., Brain stem evoked response audiometry in newborn hearing screening, Arch. Otolaryngol., 105
(1979), pp. 86–90.10. Berlin CI, Electrophysiological indices of auditory function. In: Martin FN, ed. Pediatric Audiology, Englewood Cliffs, NJ: Prentice Hall,
1978; 13-173.11. Wolf M., Birger M., Ben-Shoshan J., Kronenberg J., Conversion deafness, Ann. Otol. Rhinol. Laryngol., 102 (1993), pp. 349–352.12. Yoshida M., Noguchi A., Uemura T., Functional hearing loss in children, Int. J. Pediatr. Otorhinolaryngol., 17 (1987), pp. 287–295.13. Radkowski D., Cleveland S., Friedman E.M., Childhood pseudohypacusis in patients with high risk for actual hearing loss, Laryngoscope,
108 (1998), pp. 1543–1548.14. Wang Y.P., Wang M.C., Lin H.C., Lee K.S., Conversion deafness presenting as sudden hearing loss, J. Chin. Med. Assoc., 69 (2006), pp.
289–293.15. Gelfand S.A., Silman S., Functional components and resolved thresholds in patients with unilateral nonorganic hearing loss, Br. J. Audiol.,
27 (1993), pp. 29–34.16. Zhao H., Dai C.F., Chi F.L., Wang Z.M., Non-organic hearing loss in Chinese teenagers, Auris Nasus Larynx., 35 (2008), pp. 485–492.17. Durmaz A., Karahatay S., Satar B., Birkent H., Hidir Y., Efficiency of Stenger test in confirming profound, unilateral pseudohypacusis, J.
Laryngol. Otol., 123 (2009), pp. 840–844.18. Smurzynski J., Leonard G., Kim D.O., Lafreniere D.C., Jung M.D., Distortion product otoacoustic emissions in normal and impaired adult
ears, Arch. Otolaryngol. Head Neck Surg., 116 (1990), pp. 1309–1316.19. Glattke T.J., Kujawa S.G., Otoacoustic emissions, Am. J. Audiol., 1 (1991), pp. 29–40.20. Gaskill S.A., Brown A.M., The behavior of the acoustic distortion product, 2f1 − f2, from the human ear and its relation to auditory
sensitivity, J. Acoust. Soc. Am., 88 (1990), pp. 821–839.