Morphological features of melanocytic tumors with depigmented halo
5
Rom J Morphol Embryol 2015, 56(2 Suppl):659–663 ISSN (print) 1220–0522 ISSN (on-line) 2066–8279 REVIEW Morphological features of melanocytic tumors with depigmented halo: review of the literature and personal results ROXANA-IOANA NEDELCU 1) , SABINA ANDRADA ZURAC 2) , ALICE BRÎNZEA 1) , MIRELA-DANIELA CIOPLEA 2) , GABRIELA TURCU 3,4) , RALUCA POPESCU 4) , CĂTĂLIN-MIHAI POPESCU 4) , DANIELA ADRIANA ION 1) 1) Department of Pathophysiology II, “Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania 2) Department of Pathology, Colentina Clinical Hospital, Bucharest, Romania; “Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania 3) Department of Medicine, Yale University School of Medicine, New Haven, CT, USA 4) Department of Dermatology I, Colentina Clinical Hospital, Bucharest, Romania; “Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania Abstract Halo (Sutton’s) phenomenon has been described as a depigmented halo that is associated most commonly with acquired melanocytic nevi; but it may be associated with various types of melanocytic skin tumors, melanoma being the most concerning. Different authors have been preoccupied with elucidating morphological features of melanocytic tumors associated with a depigmented halo. We reviewed the literature and discussed the main features of melanocytic halo tumors regarding histopathological, immune microenvironment profile and dermato- scopic appearance. We highlighted similarities and differences between Sutton’s nevus and halo melanoma, also presenting relevant aspects of our results. Depigmented halo must be regarded as a phenomenon that may be associated with different types of melanocytic tumors and with a broad spectrum of histopathological atypia degree. Certain correlations between the shape, diameter, symmetry observed in clinical examination, histopathological appearance, dermatoscopic aspect of peritumoral halo and central tumor type could not be established due to insufficient data and contrasting results. Further studies are expected to add valuable information regarding the depigmented halo tumors features. Keywords: halo (Sutton’s) nevus, melanocytic tumor, melanoma, halo depigmentation, regression. Introduction Depigmented halo phenomenon was first reported in medical literature as leukoderma acquisitum centrifugum, in 1916, by Sutton [1]. Actually, the depigmented halo was first represented in a painting by the artist Grünewald in the XVIth century [2]. Halo shaped depigmentation was described in asso- ciation with numerous skin tumors and inflammatory lesions [3]. In this paper, we will discuss the morpholo- gical and pathophysiological features of the melanocytic skin lesions with halo. Sutton’s phenomenon is most commonly associated with acquired nevi [4], but also with melanoma, melanoma metastases, congenital nevo- cellular nevi, blue nevi, Spitz nevi, dysplastic melanocytic nevi, Mongolian spot [5]. Halo nevus, also known as Sutton’s nevus, is a melanocytic nevus surrounded by a depigmented rim. The presence of halo shaped depigmentation correlates with the onset of nevus regression, evolving toward total tumor resorption with the possibility of subsequent repigmentation [4]. The prevalence of Sutton’s nevi is about 1% in the general population, being more common in children and young adults of both sexes [4, 6]. Vitiligo is the disease most often associated with Sutton’s nevi. A family history of vitiligo or Sutton’s nevi was reported in some patients. The existence of halo nevi and other vitiliginous depigmentations has also been reported in patients with melanoma [7–9]. Any anatomical distribution is possible, but several authors reported a predilection of Sutton’s nevi for the trunk and for the posterior chest, when multiple nevi are present [9]. Histopathological appearance of melano- cytic lesions with halo Acquired melanocytic nevus with halo – the halo tumor prototype Halo nevus history is usually represented by the appearance of a circular depigmented area around an acquired benign melanocytic nevus. The natural evolution of Sutton’s nevi has not yet been adequately studied and reported in literature. The lesion progresses towards complete regression in several months, years, or some- times in more than a decade [10]. Over 50% of halo nevi were reported to get complete disappearance of the central pigment nevus [11]. Halo nevus pathogenesis is not completely elucidated, being considered over time an immunological, post- inflammatory or neurotropic phenomenon. However, there is strong evidence that immunological mechanisms are at the base of melanocytic destruction: the presence of an inflammatory lymphocytic infiltrate that leads to R J M E Romanian Journal of Morphology & Embryology http://www.rjme.ro/
Transcript of Morphological features of melanocytic tumors with depigmented halo

Rom J Morphol Embryol 2015, 56(2 Suppl):659–663
ISSN (print) 1220–0522 ISSN (on-line) 2066–8279
RREEVVIIEEWW
Morphological features of melanocytic tumors with depigmented halo: review of the literature and personal results
ROXANA-IOANA NEDELCU1), SABINA ANDRADA ZURAC2), ALICE BRÎNZEA1), MIRELA-DANIELA CIOPLEA2), GABRIELA TURCU3,4), RALUCA POPESCU4), CĂTĂLIN-MIHAI POPESCU4), DANIELA ADRIANA ION1)
1)Department of Pathophysiology II, “Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania 2)Department of Pathology, Colentina Clinical Hospital, Bucharest, Romania; “Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania
3)Department of Medicine, Yale University School of Medicine, New Haven, CT, USA 4)Department of Dermatology I, Colentina Clinical Hospital, Bucharest, Romania; “Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania
Abstract Halo (Sutton’s) phenomenon has been described as a depigmented halo that is associated most commonly with acquired melanocytic nevi; but it may be associated with various types of melanocytic skin tumors, melanoma being the most concerning. Different authors have been preoccupied with elucidating morphological features of melanocytic tumors associated with a depigmented halo. We reviewed the literature and discussed the main features of melanocytic halo tumors regarding histopathological, immune microenvironment profile and dermato-scopic appearance. We highlighted similarities and differences between Sutton’s nevus and halo melanoma, also presenting relevant aspects of our results. Depigmented halo must be regarded as a phenomenon that may be associated with different types of melanocytic tumors and with a broad spectrum of histopathological atypia degree. Certain correlations between the shape, diameter, symmetry observed in clinical examination, histopathological appearance, dermatoscopic aspect of peritumoral halo and central tumor type could not be established due to insufficient data and contrasting results. Further studies are expected to add valuable information regarding the depigmented halo tumors features.
Keywords: halo (Sutton’s) nevus, melanocytic tumor, melanoma, halo depigmentation, regression.
Introduction
Depigmented halo phenomenon was first reported in medical literature as leukoderma acquisitum centrifugum, in 1916, by Sutton [1]. Actually, the depigmented halo was first represented in a painting by the artist Grünewald in the XVIth century [2].
Halo shaped depigmentation was described in asso-ciation with numerous skin tumors and inflammatory lesions [3]. In this paper, we will discuss the morpholo-gical and pathophysiological features of the melanocytic skin lesions with halo. Sutton’s phenomenon is most commonly associated with acquired nevi [4], but also with melanoma, melanoma metastases, congenital nevo-cellular nevi, blue nevi, Spitz nevi, dysplastic melanocytic nevi, Mongolian spot [5].
Halo nevus, also known as Sutton’s nevus, is a melanocytic nevus surrounded by a depigmented rim. The presence of halo shaped depigmentation correlates with the onset of nevus regression, evolving toward total tumor resorption with the possibility of subsequent repigmentation [4]. The prevalence of Sutton’s nevi is about 1% in the general population, being more common in children and young adults of both sexes [4, 6]. Vitiligo is the disease most often associated with Sutton’s nevi. A family history of vitiligo or Sutton’s nevi was reported in some patients. The existence of halo nevi and other
vitiliginous depigmentations has also been reported in patients with melanoma [7–9]. Any anatomical distribution is possible, but several authors reported a predilection of Sutton’s nevi for the trunk and for the posterior chest, when multiple nevi are present [9].
Histopathological appearance of melano-cytic lesions with halo
Acquired melanocytic nevus with halo – the halo tumor prototype
Halo nevus history is usually represented by the appearance of a circular depigmented area around an acquired benign melanocytic nevus. The natural evolution of Sutton’s nevi has not yet been adequately studied and reported in literature. The lesion progresses towards complete regression in several months, years, or some-times in more than a decade [10]. Over 50% of halo nevi were reported to get complete disappearance of the central pigment nevus [11].
Halo nevus pathogenesis is not completely elucidated, being considered over time an immunological, post-inflammatory or neurotropic phenomenon. However, there is strong evidence that immunological mechanisms are at the base of melanocytic destruction: the presence of an inflammatory lymphocytic infiltrate that leads to
R J M ERomanian Journal of
Morphology & Embryologyhttp://www.rjme.ro/

Roxana-Ioana Nedelcu et al.
660
progressive destruction of nevi cells; the presence of antibodies against nevi cells [11]. Recent studies high-lighted similarities and differences between events that occur in regression of melanoma, vitiligo and in Sutton’s phenomenon [12, 13].
When the presence of cytotoxic markers in the inflam-matory infiltrate of Sutton’s nevi was studied, the result was not the expected one: none of the markers was expressed by more than 10% of lymphocytes [14]. Because of the predominance of CD8+ T-cells in the inflammatory infiltrate, the cytotoxic mechanism is thought to play a role in the immune-mediated destruction of melanocytes.
Thus, in Sutton’s nevi was usually described an inflammatory cellular infiltrate surrounding symmetrically the nevus, consisting mainly of T-lymphocytes. B-lym-phocytes, Langerhans cells and macrophages are absent or rarely observed [15]. It has been described the significant presence of CD8+ cells, expressing CD69 [16]. Although a clinically visible depigmented halo exists, histopathology may not reveal an inflammatory infiltrate in each case. In other situations, it may be described an important inflammatory infiltrate, although the halo is not clinically obvious. Clinicopathological correlation in halo nevus diagnosis is very important.
Sutton’s nevus stage with complete disappearance of nevus cells is not characterized by the development of fibrosis. Probably, at least in part, lack of fibrosis is due to the profile of the inflammatory cytokines, such as increased expression of antifibrinogenic cytokine TNF-α [12, 17]. In a study where halo nevi were classified according to the nevus type and the degree of atypia, the authors proposed that the halo nevi should not be considered a single clinicopathological entity. Depigmen-ted halo must be regarded as a phenomenon that may be associated with different types of nevi and with a broad spectrum of histopathological atypia degree. Almost half of the analyzed Sutton’s nevi expressed a significant degree of atypia and the majority nevi were compounds, junctional or intradermal nevi. Figures 1 and 2 reveal relevant aspects from two patients with halo nevocellular nevi. Sutton’s phenomenon has also been described in association with Spitz nevus [5].
In one study, the authors examined 17 cases of halo Spitz nevi confirmed histologically. In only two cases, the depigmented halo was clinically evident. In other cases, authors described recent changes in the appearance of nevi, irregular pigmentation. Halo Spitz nevi cases represented 1.3% of total Spitz nevi diagnosed in that period [18].
Ultrastructural characterization of Sutton’s nevi mela-nocytes shows poorly differentiated cells in the upper dermis. These cells still present melanosomes at the same level of differentiation and poorly represented organelles in cytoplasm [12].
Halo melanoma
Association between vitiliginous depigmentation and melanoma and/or its metastases has been reported in various studies and may present different clinical forms. Melanoma with depigmented halo is rare, but it represents the most worrisome differential diagnosis of vitiliginous halo melanocytic tumors. Because depigmented halo is associated more frequently with benign nevi than with
melanoma, it is generally regarded as a sign of safety for the benign nature of central tumor, which may lead to diagnostic and therapeutic errors. Halo melanoma incorrect approach may be favored by its evolution to complete regression, process similar to that of benign halo nevus. Unfortunately, in halo melanoma cases with complete regression, it has been reported local and distant metastasis [19]. Regression is more common in adults [20]. It is considered that the halo associated with melanoma has a more asymmetric shape comparative with that associated with melanocytic nevi [21] and patients are older in the first case [19].
It is extremely important to distinguish halo nevus from regressing melanoma. The main differences between the histopathological appearance of a halo nevus and melanoma can be summarized as follows: in Sutton’s nevi, nevi cells are arranged in nests, while in the mela-noma are described isolated atypical melanocytes in the epidermis and atypical melanocytes aggregates in the dermis; well-known difference between symmetric appea-rance of the nevus and the asymmetric one of the mela-noma; mature cells without mitosis or with rare mitosis characteristic for nevus when compared with numerous mitotic immature cells in melanoma; diffuse character, throughout entire lesion, of lymphocytic infiltration in Sutton nevus but concentrated inflammatory infiltrate in periphery, in melanoma [22].
Nevi cells destruction, characteristic for the biological evolution of the halo nevi, has not resulted in the deve-lopment of fibrosis. On the other hand, the destruction of tumor cells during the regression of melanoma results in the papillary dermal fibrosis during final stage of resorption [17]. The absence of fibrosis in the Sutton’s nevi can be explained by the different profile of cytokines compared to the phenomenon of regression of melanoma, as we mentioned earlier [12].
Ultrastructurally, melanocytic cells analyzed in the regression of melanoma are strongly activated, being in an environment rich in cytokines; melanosomes in different stages of differentiation and numerous cytoplasmic orga-nelles are present. In contrast, melanocytes from the halo nevi are poorly differentiated immunological, melanosomes shows the same level of differentiation and poor repre-sentation of cytoplasmic organelles [12].
Features of the relationship between central melanocytic nevus and depig-mented halo
The natural history of halo nevi has not been ade-quately studied. It was reported that more than half of Sutton’s nevi completely regress [11]. In a recently publi-shed retrospective study, the biological evolution of Sutton’s nevi was studied over a period of 17 years, yielded the following results: in 51% of cases there was no change in the nevus or peritumoral halo; in 14.3% of cases, partial regression and the presence of the halo were observed; 4.1% of nevi are fully regressed, persistent depigmentation being present; 22.4% have evolved with the repigmentation, obtaining the normal skin color [10]. Sutton’s nevi generally persist over a period of years and sometimes progresses to complete regression.

Morphological features of melanocytic tumors with depigmented halo: review of the literature and personal results
661
Figure 1 – Mixed nevocellular nevus with halo (female, 26-year-old, periumbilical
tumor): (A) Nevi cells proliferation, some pigmented, arranged in scattered nests
at the level of dermo-epidermal junction and in the papillary dermis; marked lymphocytic inflammatory infiltrate intratumoral extended to the level of
epidermis, causing tumor architecture fading, sometimes embedding and isolating nevus cells. HE staining,
×50; (B) Detail of the previous image. Nevi cells nests dissected by the inflammatory infiltrate. HE staining, ×100.
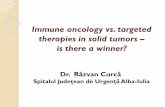
Figure 2 – Mixed nevocellular nevus with inflammatory infiltrate halo type (male, 37-year-old, posterior chest): (A and B) Nevocellular proliferation arranged in nests at dermal level, with minimal junctional representation; marked lymphocytic inflammatory infiltrate intra and peritumoral (HE staining: A, ×50; B, ×100); (C and D) Nevus cells have large size, hypertrophic nuclei, rare moderate atypia and intracytoplasmic melanin pigment deposition; mitotical activity not identified (HE staining, ×200); (E) Nevi cell are positive for S100 (S100 immunostaining, ×100); (F) HMB45 positive in tumor with expression lost profound (HMB45 immunostaining, ×100); (G–L) The tumor cells are positive for E-cadherin (G, ×100), MMP1 (H, ×100), MMP3 (I, ×100), MMP11 (J, ×100), MMP13 (K, ×200), p16 (L, ×200).

Roxana-Ioana Nedelcu et al.
662
The size of the achromic halo varies; most frequently, it has been reported in the literature as having values between 0.5 and 5 cm [9]. Factors influencing the halo diameter were not studied until recently, and the signi-ficance of this diameter and a possible correlation between the diameter of the halo and the one of the central nevus are evaluated in recent studies [23].
Rongioletti et al. have described a linear correlation between the diameters of both the nevus and the halo and proposed the existence of “melanocyte antigen units” (MAU). Melanocyte antigenic unit would be defined by melanocytes, which extend radially from the central melanocytic lesion, having the same phenotype and being functionally dependent on the central nevus. This unit is not usually clinically detectable, becoming visible only in halo nevi and halo melanomas. Also, the concept of melanocytic antigen unit could bring a new explanation relevant to the etiopathogenesis of the recurrent melano-cytic nevus. The melanocytic recurrent nevus could rise from the adjacent melanocytes level of the surgically removed primary nevus, melanocytes that were not clini-cally visible during excision. Currently, it is considered that this melanocytic pigmented lesion originate in the deep follicle melanocytes, which were not removed during the excision of primary nevus [23]. Another situation where melanocytic antigen unit can bring new relevant
explanations refers to melanoma tumor margins, sugges-ting the existence of a satellite area around the tumor, dependent on tumoral melanocytes [23].
Dermatoscopic features of melanocytic halo tumors
Kolm et al. analyzed dermatoscopically 138 halo nevi from 87 patients. Globular and homogeneous patterns were typical aspects of halo nevi, a small percentage showing reticular pattern. Thirty-three of nevi were followed up and, although significant changes were described in halo and nevus diameter after six months, no tumors pattern changes were noticed [21].
Recent studies have described dermatoscopic aspects specific to halo melanocytic lesions, facilitating halo melanoma diagnosis [21]. This may present a multi-component model: atypical pigment network, irregular globules, points, radial structures and irregular vascular pattern. Dermatoscopic patterns of melanocytic resorption were also highlighted: white/blue veil, scar appearance. These clinical and dermatoscopic features are strongly associated with melanoma and when its noticed the histo-pathological examination is necessary [24]. The above-mentioned differences between halo melanoma and halo nevus are illustrated in Figure 3.
Figure 3 – Clinical and dermatoscopic aspect of halo melanoma (A–C) in
comparison with the halo nevus (D and E).
Conclusions and future perspectives
Halo (Sutton’s) phenomenon has been described as a depigmented halo that is associated most commonly with acquired melanocytic nevi. Depigmented halo may be associated with various types of melanocytic skin tumors, melanoma being the most concerning. It is extremely important to distinguish halo nevus from regressing melanoma. When clinical and dermatoscopic assessments emphasize atypia of melanocytic tumors with depigmented halo, histopathological evaluation should be considered. In Sutton’s nevi, nevi cells are arranged in nests, while in the melanoma are described isolated atypical melanocytes in the epidermis and atypical mela-nocytes aggregates in the dermis. Mature cells without
mitosis or with rare mitosis are characteristic for nevus when compared with numerous mitotic immature cells in melanoma. The lymphocytic infiltrate has usually a diffuse character, throughout entire Sutton’s nevus but it is more concentrated in periphery of melanoma.
The destruction of tumor cells during the regression of melanoma results in the papillary dermal fibrosis during final stage of resorption. Sutton’s nevi cells destruction is not characterized by the development of fibrosis.
Further studies are expected to add valuable information regarding the depigmented halo features. Melanocytic lesions with depigmented halo are also important topics for current research, Sutton’s phenomenon being an anti-melanocytic antitumoral immunity model.

Morphological features of melanocytic tumors with depigmented halo: review of the literature and personal results
663
Conflict of interests The authors declare that they have no conflict of
interests.
Author contribution All the authors had equal contributions to the article.
Acknowledgments This paper is partially supported by the Sectoral
Operational Programme Human Resources Development (SOP HRD), financed from the European Social Fund and by the Romanian Government under the contract number POSDRU/159/1.5/S/137390. This paper is partially supported by Executive Agency for Higher Education, Research, Development and Innovation (UEFISCDI) under the contract number PN-II-PT-PCCA-2013-4-1407 (Project No. 190).
References [1] Sutton RL. An unusual variety of vitiligo (leukoderma acquisitum
centrifugum). J Cutan Dis, 1916, 34:797–800. [2] Borroni C, Vignati G. Should Sutton nevus really be called
Grünewald–Sutton nevus? Am J Dermatopathol, 1993, 15(5): 506–508.
[3] Nedelcu RI. Morphoclinical and pathophysiological implications of autoimmune depigmentation related to melanocytic lesions. PhD Thesis, “Carol Davila” University of Medicine and Phar-macy, Bucharest, Romania, November 2013.
[4] Bolognia JL, Jorizzo JL, Rapini RP, Ortonne JP. Vitiligo and other disorders of hypopigmentation. In: Bolognia JL, Jorizzo JL, Rapini RP, Ortonne JP (eds). Dermatology. 2nd edition, Mosby–Elsevier, 2008, 947–974.
[5] Mooney MA, Barr RJ, Buxton MG. Halo nevus or halo phenomenon? A study of 142 cases. J Cutan Pathol, 1995, 22(4):342–348.
[6] Stierman SC, Tierney EP, Shwayder TA. Halo congenital nevocellular nevi associated with extralesional vitiligo: a case series with review of the literature. Pediatr Dermatol, 2009, 26(4):414–424.
[7] Epstein WL, Sagebeil R, Spitler L, Wybran J, Reed WB, Blois MS. Halo nevi and melanoma. JAMA, 1973, 225(4):373–377.
[8] Albert DM, Todes-Taylor N, Wagoner M, Nordlund JJ, Lerner AB. Vitiligo or halo nevi occurring in two patients with choroidal melanoma. Arch Dermatol, 1982, 118(1):34–36.
[9] Speeckaert R, van Geel N, Vermaelen KV, Lambert J, Van Gele M, Speeckaert MM, Brochez L. Immune reactions in benign and malignant melanocytic lesions: lessons for immuno-therapy. Pigment Cell Melanoma Res, 2011, 24(2):334–344.
[10] Aouthmany M, Weinstein M, Zirwas MJ, Brodell RT. The natural history of halo nevi: a retrospective case series. J Am Acad Dermatol, 2012, 67(4):582–586.
[11] Frank SB, Cohen HJ. The halo nevus. Arch Dermatol, 1964, 89(3):367–373.
[12] Moretti S, Spallanzani A, Pinzi C, Prignano F, Fabbri P. Fibrosis in regressing melanoma versus nonfibrosis in halo nevus upon melanocyte disappearance: could it be related to a different cytokine microenvironment? J Cutan Pathol, 2007, 34(4):301–308.
[13] de Vijlder HC, Westerhof W, Schreuder GM, de Lange P, Claas FH. Difference in pathogenesis between vitiligo vulgaris and halo nevi associated with vitiligo is supported by an HLA association study. Pigment Cell Res, 2004, 17(3):270–274.
[14] Fernandez-Flores A, Saeb-Lima M. The inflammatory infiltrate of melanocytic nevus. Rom J Morphol Embryol, 2014, 55(4): 1277–1285.
[15] Zeff RA, Freitag A, Grin CM, Grant-Kels JM. The immune response in halo nevi. J Am Acad Dermatol, 1997, 37(4):620–624.
[16] Fernández-Herrera J, Fernández-Ruiz E, López-Cabrera M, García-Díez A, Sánchez-Madrid F, González-Amaro R. CD69 expression and tumour necrosis factor-alpha immunoreactivity in the inflammatory cell infiltrate of halo naevi. Br J Dermatol, 1996, 134(3):388–393.
[17] Blessing K, McLaren KM. Histological regression in primary cutaneous melanoma: recognition, prevalence and signifi-cance. Histopathology, 1992, 20(4):315–322.
[18] Harvell JD, Meehan SA, LeBoit PE. Spitz’s nevi with halo reaction: a histopathological study of 17 cases. J Cutan Pathol, 1997, 24(10):611–619.
[19] Rubegni P, Nami N, Risulo M, Tataranno D, Fimiani M. Melanoma with halo. Clin Exp Dermatol, 2009, 34(6):749–750.
[20] Requena C, Botella-Estrada R, Traves V, Nagore E, Almenar S, Guillén C. Problems in defining melanoma regression and prognostic implication. Actas Dermosifiliogr, 2009, 100(9): 759–766.
[21] Kolm I, Di Stefani A, Hofmann-Wellenhof R, Fink-Puches R, Wolf IH, Richtig E, Smolle J, Kerl H, Soyer HP, Zalaudek I. Dermoscopy patterns of halo naevi. Arch Dermatol, 2006, 142(12):1627–1632.
[22] Zabawski EJ Jr, Cockerell CJ. Halo nevus. http://emedicine. medscape.com/article/1057446-overview, 2012.
[23] Rongioletti F, Cecchi F, Rebora A. Halo phenomenon in melanocytic nevi (Sutton’s nevi). Does the diameter matter? J Eur Acad Dermatol Venereol, 2011, 25(10):1231–1232.
[24] Arpaia N, Cassano N, Vena GA. Regressing cutaneous malignant melanoma and vitiligo-like depigmentation. Int J Dermatol, 2006, 45(8):952–956.
Corresponding author Roxana Ioana Nedelcu, MD, PhD, Department of Pathophysiology II, Clinical Department No. 2, “Carol Davila” University of Medicine and Pharmacy, Bucharest; “Matei Balş” National Institute of Infectious Diseases – HIV/AIDS and Infectious Diseases Academy, 3rd Floor, Room 302, 1 Dr. Calistrat Grozovici Street, 021105 Bucharest, Romania; Phone +40721–916 624, e-mail: [email protected] Received: April 18, 2015
Accepted: July 21, 2015